 Isabell Nilsson1Jeremy Palmer2Eirini Apostolou1
Isabell Nilsson1Jeremy Palmer2Eirini Apostolou1 Carl-Gerhard Gottfries3Muhammad Rizwan1Charlotte Dahle1
Carl-Gerhard Gottfries3Muhammad Rizwan1Charlotte Dahle1 Anders Rosén1*
Anders Rosén1*- 1Division of Cell Biology, Department of Biomedical and Clinical Sciences, Linköping University, Linköping, Sweden
- 2The Medical School, The University Newcastle upon Tyne, Newcastle upon Tyne, United Kingdom
- 3The Gottfries Clinic AB, Mölndal, Sweden
Metabolic profiling studies have recently indicated dysfunctional mitochondria in myalgic encephalomyelitis/chronic fatigue syndrome (ME/CFS). This includes an impaired function of pyruvate dehydrogenase complex (PDC), possibly driven by serum factor(s), which leads to inadequate adenosine triphosphate generation and excessive lactate accumulation. A reminiscent energy blockade is likely to occur in primary biliary cholangitis (PBC), caused by anti-PDC autoantibodies, as recently proposed. PBC is associated with fatigue and post-exertional malaise, also signifying ME/CFS. We herein have investigated whether ME/CFS patients have autoreactive antibodies that could interfere with mitochondrial function. We found that only 1 of 161 examined ME/CFS patients was positive for anti-PDC, while all PBC patients (15/15) presented significant IgM, IgG, and IgA anti-PDC reactivity, as previously shown. None of fibromyalgia patients (0/14), multiple sclerosis patients (0/29), and healthy blood donors (0/44) controls showed reactivities. Anti-mitochondrial autoantibodies (inner and outer membrane) were negative in ME/CFS cohort. Anti-cardiolipin antibody levels in patients did not differ significantly from healthy blood donors. In conclusion, the impaired mitochondrial/metabolic dysfunction, observed in ME/CFS, cannot be explained by presence of circulating autoantibodies against the tested mitochondrial epitopes.
Introduction
Myalgic encephalomyelitis (ME), also called chronic fatigue syndrome (CFS), or systemic exertional intolerance disease (SEID), is a common debilitating disease of unknown etiology characterized by post-exertional malaise (PEM), cognitive disturbance, unrefreshing sleep, autonomous nerve dysfunction and other characteristic comorbidities (1, 2). The disease may affect 0.1–0.4% of the population according to the Canadian consensus criteria (3). The biology of ME/CFS is complex and diverse explanatory models for ME/CFS have been proposed include autoimmunity, chronic infection, energy metabolic defect, imbalance in autonomous nervous system and/or hormones, and psychosomatic dysfunction.
Accumulating evidence are pointing toward an autoimmune phenotype for ME/CFS. The presence of self-reacting antibodies in the circulation of patients include nuclear and membrane structures, neurotransmitters and their receptors, neo-autoantigens formed by oxidative or nitrosative damage, and autoantibodies targeted to mitochondrial components (Table 1). However, both the frequency and the titers of autoantibodies and their correlation to disease severity or symptoms has had limited reproducibility between different studies and patient cohorts. Still, a subset of ME/CFS patients presented amelioration of symptoms following antibody removal treatment (18). Specific changes in the proteome of CSF of ME/CFS patients involved the accumulation of complement components, which signify antibody activity (19). In a recent publication from our group, the serological profile of the same ME/CFS patient cohorts demonstrated evidence of minor alterations of antibody reactivities against the ubiquitous herpesviruses when compared to healthy controls (20). These alterations may indicate shortcomings in humoral responses in ME/CFS which are hallmarks of autoimmune diseases.
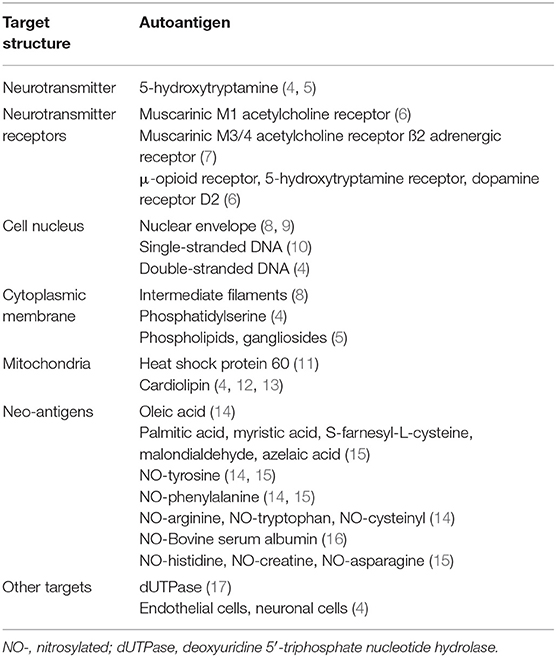
Table 1. Autoantibodies recorded in Myalgic Encephalomyelitis/Chronic Fatigue Syndrome patients.
Recent reports point toward a central metabolic defect in ME/CFS, which affects aerobic energy production via the tricarboxylic acid (TCA) cycle in mitochondria, leading to a diminished production of adenosine triphosphate (ATP) and excessive lactate generation upon exertion, possibly explaining PEM (21, 22). The transition between anaerobic and aerobic energy production is catalyzed by the pyruvate dehydrogenase complex (PDC). Autoantibodies specific for PDC is a hallmark of primary biliary cholangitis (PBC), a potential disease model of autoantibody-mediated energy blockade (23, 24). In analogy with PBC, in which energy production is inhibited by antibodies (25), circulating energy inhibitors have also been detected in ME/CFS (21), however, their molecular nature is unknown. It would be reasonable if these circulating inhibitors turned out to be immunoglobulins, presumably directed against mitochondrial antigens. We have therefore investigated the presence of anti-mitochondrial antibodies and anti-PDC reactive autoantibodies, in ME/CFS patients.
Methods
Participants
All ME/CFS patients included in this study were diagnosed according to the Canadian consensus criteria (3). ME/CFS patients reported impairment was assessed by the Fibro-fatigue scale (26). Blood samples were acquired from three ME/CFS cohorts. Cohort 1 (n = 74): 46 ME/CFS patients, 17 ME/CFS + fibromyalgia (FM) patients, and 11 FM patients. This cohort also included 29 multiple sclerosis (MS) patients. Cohort 2 (n = 61): 61 ME/CFS patients; Cohort 3 (n = 40): 18 ME/CFS patients, 19 ME/CFS/FM patients, 3 FM patients, and 15 age-matched healthy donors in cohort 3 (HD3). Samples from cohorts 1–3 originated from the Gottfries Clinic, Mölndal, Sweden. The characteristics of the patients are summarized in Table 2. Plasma samples from 15 PBC patients were collected at the blood bank of The Medical School in The University of Newcastle upon Tyne, UK. Additional controls included serum samples from 46 anonymous healthy blood donors from Uppsala Academic Hospital University, Sweden.

Table 2A. Characteristics of patient study cohorts 1 and 2.
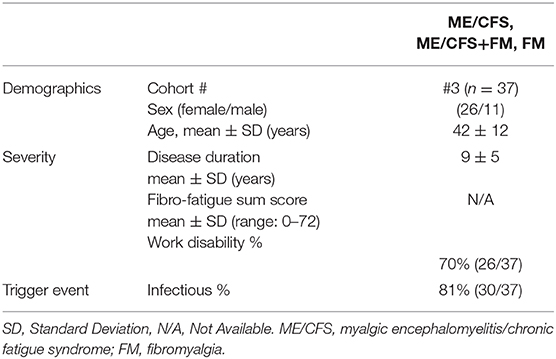
Table 2B. Characteristics of patient study cohort 3.
Ethics Statement
Informed consent for blood collection was obtained from all patients according to the Declaration of Helsinki, and ethical approval was granted by the ethical review committee at Medical Faculty, University of Gothenburg Dnr 029-13, Dnr 867-13, T 091-16, and Dnr 852-12, T 092-16 (CGG). Blood donor samples were collected anonymously according to ethical consent from the Uppsala Institutional Review Board (IRB) UPS_01_367, and Linköping Regional Office of Swedish Ethical Review Authority. The 15 PBC patient samples from Newcastle upon Tyne, were under REC number 12/NE/0095.
Detection of Anti-PDC Antibodies
Antibodies against human PDC (hPDC) were measured by in-house ELISA, as previously described (27). Briefly, wells of Immulon 4HBX microtiter plates (Dynex Technologies Inc., El Paso, TX) were coated with 2.5 μg/ml hPDC in 50 mM NaHCO3/Na2CO3 (pH 9.6). The plates were blocked with 5% (w/v) bovine serum albumin (BSA) in phosphate-buffered saline (PBS), and incubated with plasma diluted 1:500 in PBS/0.5% (w/v) BSA for 3 h. Specific antibody binding was detected with goat anti-human IgG, IgM, or IgA heavy chain specific peroxidase conjugates (Sigma, Poole, UK) and o-phenylenediamine dihydrochloride (OPD). Absorbance was recorded at 492 nm, and any values over 0.370 nm (mean OD value +3 SD) were regarded as positive for IgG anti-PDC, 0.211 nm for IgM and 0.0152 nm for IgA.
Validation of Anti-PDC Antibodies
Extracted human PDC was resolved with 10% SDS PAGE and immunoblotting was performed as previously described (24, 27). The membrane was blocked with 5% (w/v) skimmed milk powder and then probed with patient plasma from three ME/CFS and one ME/CFS/FM, all diluted 1:500 in 0.5% w/v of BSA in PBS–T. Bound antibodies were detected using goat anti-human IgG peroxidase-conjugated antibodies (Sigma, Poole, UK) and enhanced chemiluminescence (ECL; Amersham, Aylesbury, UK) according to the manufacturer's protocol.
Detection of Anti-mitochondrial Autoantibodies (AMA)
Plasma samples from 29 randomly selected ME/CFS patients were screened using Multi-spot slides, with fixed tissue sections (NOVA Lite® Rat Stomach, Liver, Kidney, San Diego, CA). All procedures were performed according to the manufacturer's instructions as part of a validated method used for diagnostic purposes in Linköping University Hospital, Sweden.
Detection of Anti-cardiolipin Autoantibodies (ACA)
IgG and IgM anti-cardiolipin antibodies were analyzed in the Clinical Immunology Laboratory, Linköping University Hospital, Sweden using the ELiAtex™ cardiolipin IgG and IgM fluoro-enzyme-immunoassay with the Phadia-250 instrument (Thermo-Fisher Scientific Phadia AB, Uppsala, Sweden). For IgA anti-cardiolipin antibodies, samples were examined with the Inova QUANTA Lite ACA IgA III ELISA (Inova, Altenhostrasse, Germany). Both assays were done according to manufacturer's instructions.
Statistical Analysis
For the comparison between multiple patient groups, we used one-way analysis of variance (ANOVA) using GraphPad Prism version 6.0 software (GraphPad Software, San Diego, CA, USA). Only statistically significant differences p < 0.05 were reported.
Results
Autoantibodies Against Mitochondrial Pyruvate Dehydrogenase Complex (PDC) Not Detected in ME/CFS
In this study, we analyzed whether dysfunctional energy generation from mitochondria in ME/CFS could be explained by the presence of reactive autoantibodies directed against the PDC enzyme, in analogy to what has been observed in PBC. ME/CFS, PBC, FM, MS and healthy blood donor controls were analyzed (Figure 1). PBC patient plasma samples were all positive for IgG, IgM, and IgA anti-PDC antibodies and hence presented with statistically significant differences (p < 0.0001). In repeated analyses, these samples remained positive down to dilutions of 1:105−1:106. In contrast to our hypothesis, ME/CFS samples were negative for autoantibodies against PDC, with the exception of three ME/CFS patients: #43 (A = 1.217 at 1:500); ME/CFS patient #69 (A = 0.406 at 1:500); ME/CFS patient #166 (A = 0.418 at 1:500); and #21, a ME/CFS patient with FM comorbidity (A =1.658 at 1:500) that was found weakly/intermediately positive. These plasma samples were tested additionally by immunoblot analysis for validation. Only sample from patient #21 (ME/CFS+FM) was positive, whereas the other samples were negative (Figure 2). Autoreactivity was identified against the major autoreactive epitopes within the PDC complex, dihydrolipoamide acetyltransferase (E2) and the E3-binding protein (E3BP) as previously described (24).
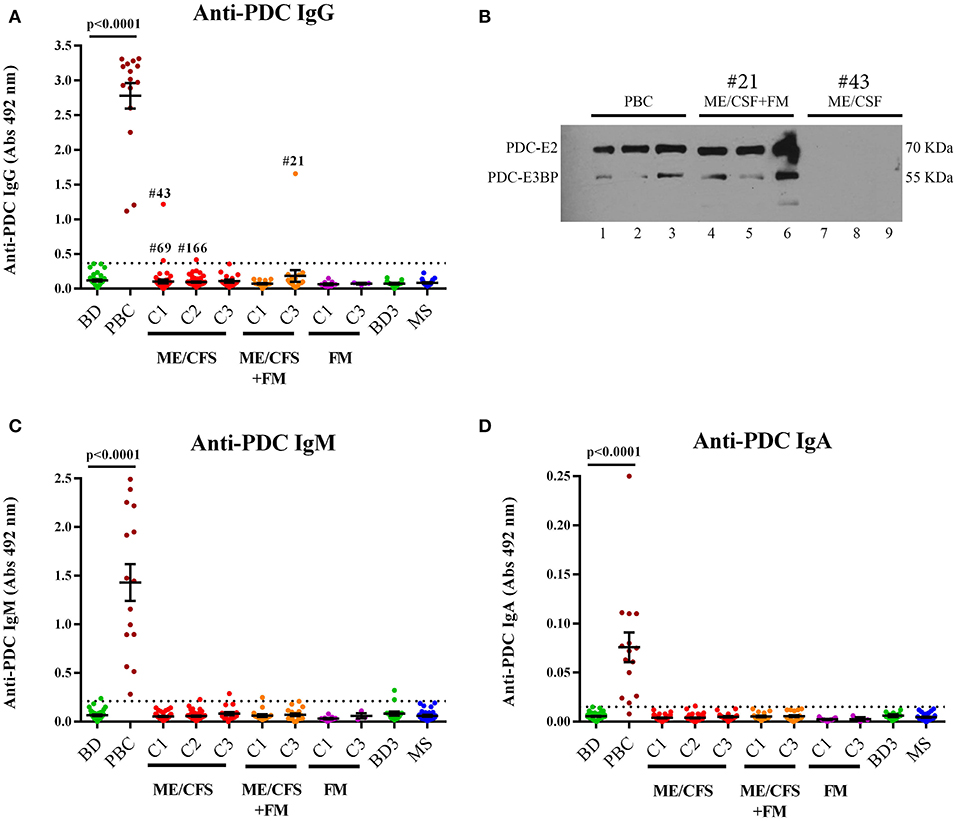
Figure 1. (A) Anti-pyruvate dehydrogenase complex (anti-PDC) IgG antibody levels in the plasma of healthy blood donors (BD, n = 44), primary biliary cholangitis patients (PBC, n = 15), myalgic encephalomyelitis/chronic fatigue syndrome (ME/CFS) patients (cohort 1: C1, n = 46, cohort 2: C2, n = 61 and cohort 3: C3, n = 18), myalgic encephalomyelitis/chronic fatigue syndrome with fibromyalgia (ME/CFS+FM) (cohort 1: C1, n = 17 and cohort 3: C3, n = 19), fibromyalgia (FM) patients (cohort 1: C1, n = 11 and cohort 3: C3, n = 3), age-matched healthy blood donors (BD3, n = 15) from cohort 3, and multiple sclerosis (MS) patients (cohort1: C1, n = 29). (B) Immunoblot analysis against human extracted pyruvate dehydrogenase of pooled primary biliary cholangitis (PBC) serum (lanes 1–3), plasma sample from patient #21 with myalgic encephalomyelitis/chronic fatigue syndrome with fibromyalgia (ME/CFS+FM patient (lanes: 4–6), and plasma sample from patient #43 with myalgic encephalomyelitis/chronic fatigue syndrome patient (lanes: 7–9). Samples were found positive for anti-PDC antibodies using the anti-PDC ELISA. Pooled PBC sample and patient #21 (ME/CFS+FM) were found positive for the major autoreactive proteins within the PDC complex, dihydrolipoamide acetyltransferase (E2) and the E3-binding protein (E3BP), whereas patient #43 (ME/CFS) was found negative. (C,D) Anti-PDC antibody levels of IgM and IgA subclass in the same samples as in panel (A). Dotted line represents cut-off levels for each Immunoglobulin subclass. Data are represented as individual points for each subject, overlaid by a horizontal mean group value ± SEM. Multiple group comparisons were analyzed by one-way ANOVA. Statistically significant differences are indicated (p < 0.0001).
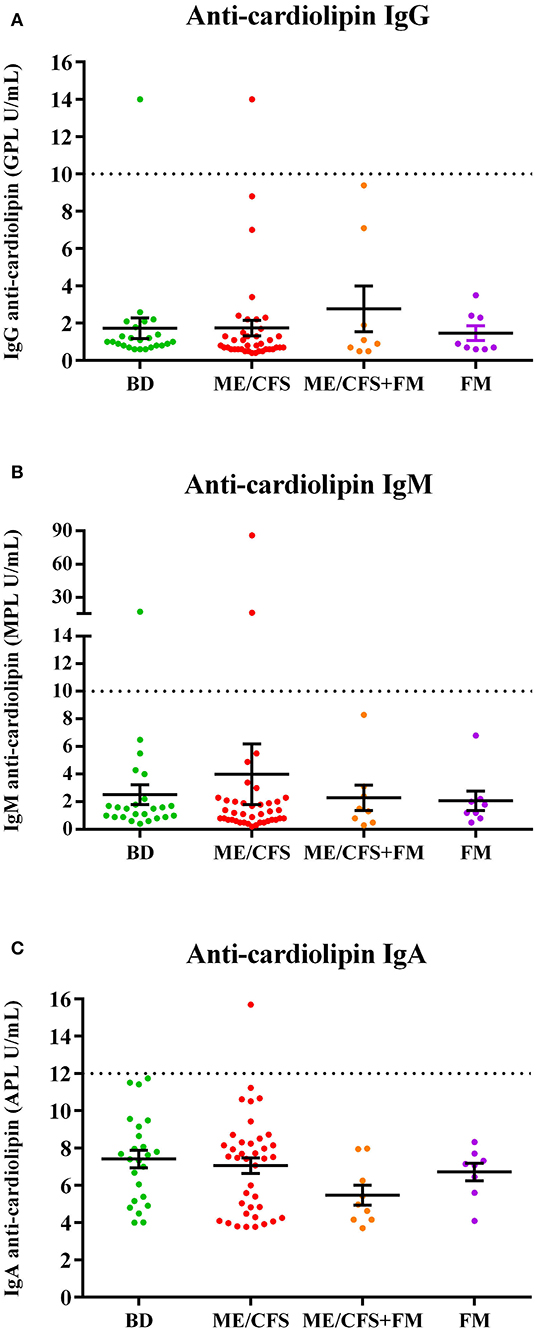
Figure 2. Anti-cardiolipin (ACA) antibody levels of IgG (A), IgM (B), and IgA (C) subclasses in the plasma of healthy blood donors and patients in cohort 1. For IgG and IgM the analysis included samples from healthy blood donors (BD, n = 24), myalgic encephalomyelitis/chronic fatigue syndrome (ME/CFS patients, n = 39), myalgic encephalomyelitis/chronic fatigue syndrome with fibromyalgia (ME/CFS+FM, n = 8) and fibromyalgia (FM, n = 8) patients. For IgA ACA analysis samples included BD (n = 24), ME/CFS patients (n = 39), ME/CSF+FM patients (n = 9), and FM (n = 8) patients. GPL, MPL, and APL correspond to IgG, IgM and IgA phospholipid units, respectively. Dotted lines represent cut-off levels for each subclass. Data are represented as individual points for each subject, overlaid by a horizontal mean group value ± SEM. For IgG and IgM ACA antibody levels, values < 10 U/mL were considered negative, values between 10 and 40 were considered as weak positive and values higher that 40 were considered positive. For IgA ACA, values < 12 U/mL were considered negative. No statistically significant differences were noted.
AMA and ACA Not Detected in ME/CFS Patients
The ME/CFS patient group did not exhibit AMAs, against inner and outer mitochondrial membrane, nor antibodies against other mitochondrial structures, nor other structures (nuclear, smooth muscle, gastric parietal cell). Anti-cardiolipin antibody (IgG, IgM, IgA) levels were not significantly different in plasma of ME/CFS or FM patients compared with blood donors (Figure 2).
Discussion
We conclude from the results presented in this study, that in contrast to our initial expectation, ME/CFS patients do not have autoantibodies to epitopes of mitochondrial components. This does not rule out that other important indirect or secondary mechanisms exist in blocking the complex mitochondrial pyruvate metabolism in ME/CFS.
An example of autoimmunity with autoreactive antibodies against a key metabolic factor is PBC. It was previously shown that anti-PDC antibodies in these patients are mainly directed against the inner lipoyl domain of the PDC-E2 component, which has an alpha-lipoic acid covalently bound to a specific lysine residue, which is an absolute requirement for its enzymatic activity. Lipoylation is a posttranslational modification, which also occurs in bacteria like E. coli or Novosphingobium sp. (28). Autoreactive responses in PBC have been suggested to arise after infection in the gut with these bacteria (29, 30) or beta-retroviruses (31), or exposure to environmental xenobiotics that mimic the native lipoic acid moiety (32). PBC patients have a PEM reminiscent of PEM in ME/CFS and FM patients (33). FM is a common comorbidity in both ME/CFS, occurring in ~30–70% of the patients, and autoimmunity (34–36). Metabolic disturbances in ME/CFS with reduced energy supply and increased lactate may account for most of the malaise in PEM as well as cognitive and physical disturbances (37). Notably, accumulation of lactate in blood and muscles after exercise, along with increased concentrations of lactate in cerebrospinal fluid (CSF) have been found in ME/CSF (38, 39). However, our present comparative analysis for AMA, anti-PDC, and anti-cardiolipin autoantibodies in the 3 cohorts did not yield a positive or disease-specific result.
A link between mitochondrial dysfunction and innate immune dysregulation is suggested which demonstrate that the energy producing organelles (mitochondria and peroxisomes) are coupled via mitochondrial antiviral signaling proteins (MAVS) to the inflammasome (40). Hypothetically, danger-associated molecular patterns (DAMPs), such as mitochondrial DNA (mtDNA), heat shock proteins (Hsps), and cardiolipins could be released from the mitochondria (41–43) in ME/CFS and act as autoantigens. We previously found that a subset of ME/CFS patients had higher levels of IgM antibodies against epitopes of both mitochondrial and bacterial Hsp-60 (despite the absence of an infectious pathogen) which potentially may lead to dysfunctional mitochondria (11). Our hypothesis on the presence of autoantibodies against cardiolipin in ME/CFS patients was based on previous publications (ref in Table 1), could not be confirmed here, possible explained by different inclusion and exclusion criteria of patients in previous studies that did not used Canadian criteria, but included leukemia/lymphoma and type 1 diabetes patients. Further studies are required to analyse unique epitope alterations such as oxidation epitopes of cardiolipin (42), length and 3D-structure, which each may signal differently in this complex immune-metabolic scenario.
The hypothesis of a direct blocking of PDC due to autoreactive antibodies is excluded based on our present findings, however, blocking could be secondary and a sign of compensatory efforts to balance some other abnormalities in ME/CFS, as suggested by Fluge et al. (21). Their data indicate a functional impairment of PDC leading to increased consumption of specifically ketogenic and anaplerotic amino acids that fuel alternative pathways for ATP production independently of PDC. The results were supported by increased mRNA expression of pyruvate dehydrogenase kinases that are inhibitory to PDC (21). Recent studies also show that many fatty acids may generate acetyl-CoA that fuel the TCA-cycle independently of PDC (44). Similar observations on altered energy metabolism may occur in different types of cellular stress such as starvation (45). Blocking of PDC could also be generated by other mechanisms including reduction-oxidation (redox) reactions known to modulate lipoic acid moiety in the PDC (46). Therefore, it would be of interest to investigate in future studies the PDC redox status in ME/CFS patients. Finally, multiple enzymes such as mitochondria pyruvate carrier, pyruvate carboxylases, PD-kinases, PD-phosphatases, in addition to PDC, modulate overall pyruvate carbon flux (47).
Data Availability Statement
The datasets generated for this study are available on request to the corresponding author.
Ethics Statement
The studies involving human participants were reviewed and approved by the ethical review committee at Medical Faculty, University of Gothenburg; Uppsala Institutional Review Board; Linköping Regional Office of Swedish Ethical Review Authority, Newcastle upon Tyne, under REC number 12/NE/0095; Regional ethic committee of Stockholm. The patients/participants provided their written informed consent to participate in this study.
Author Contributions
IN, JP, and EA designed and performed experiments, analysis, and authored the manuscript. MR and C-GG provided critical materials. CD performed experiments and analysis. AR conceived the design and execution of all experimental procedures and authored the manuscript. All authors critically reviewed the final manuscript.
Funding
This work was financed with grants from the Swedish ME Association (AR), Solve ME/CFS (AR), the Swedish Cancer Association (AR), and the Open Medicine Foundation (OMF) (AR).
Conflict of Interest
C-GG was employed by the Gottfries Clinic AB company.
The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Acknowledgments
The authors would like to thank ME/CFS patients for their interest in the study.
References
1. Blomberg J, Gottfries CG, Elfaitouri A, Rizwan M, Rosén A. Infection elicited autoimmunity and ME/CFS syndrome: an explanatory model. Front Immunol. (2018) 9:229. doi: 10.3389/fimmu.2018.00229
2. Mensah FKF, Bansal AS, Ford B, Cambridge G. Chronic fatigue syndrome and the immune system: where are we now? Neurophysiol Clin. (2017) 47:131–8. doi: 10.1016/j.neucli.2017.02.002
3. Carruthers BM, van de Sande MI, De Meirleir KL, Klimas NG, Broderick G, Mitchell T, et al. Myalgic encephalomyelitis: international consensus criteria. J Intern Med. (2011) 270:327–8. doi: 10.1111/j.1365-2796.2011.02428.x
4. Ortega-Hernandez OD, Cuccia M, Bozzini S, Bassi N, Moscavitch S, Diaz-Gallo LM, et al. Autoantibodies, polymorphisms in the serotonin pathway, and human leukocyte antigen class II alleles in chronic fatigue syndrome: are they associated with age at onset and specific symptoms? Ann N Y Acad Sci. (2009) 1173:589–99. doi: 10.1111/j.1749-6632.2009.04802.x
5. Klein R, Berg PA. High incidence of antibodies to 5-hydroxytryptamine, gangliosides and phospholipids in patients with chronic fatigue and fibromyalgia syndrome and their relatives: evidence for a clinical entity of both disorders. Eur J Med Res. (1995) 1:21–6.
6. Tanaka S, Kuratsune H, Hidaka Y, Hakariya Y, Tatsumi KI, Takano T, et al. Autoantibodies against muscarinic cholinergic receptor in chronic fatigue syndrome. Int J Mol Med. (2003) 12:225–30. doi: 10.3892/ijmm.12.2.225
7. Loebel M, Grabowski P, Heidecke H, Bauer S, Hanitsch LG, Wittke K, et al. Antibodies to beta adrenergic and muscarinic cholinergic receptors in patients with Chronic Fatigue Syndrome. Brain Behav Immun. (2016) 52:32–9. doi: 10.1016/j.bbi.2015.09.013
8. Konstantinov K, von Mikecz A, Buchwald D, Jones J, Gerace L, Tan EM. Autoantibodies to nuclear envelope antigens in chronic fatigue syndrome. J Clin Investig. (1996) 98:1888–96. doi: 10.1172/JCI118990
9. von Mikecz A, Konstantinov K, Buchwald DS, Gerace L, Tan EM. High frequency of autoantibodies to insoluble cellular antigens in patients with chronic fatigue syndrome. Arthritis Rheum. (1997) 40:295–305. doi: 10.1002/art.1780400215
10. Vernon SD, Reeves WC. Evaluation of autoantibodies to common and neuronal cell antigens in Chronic Fatigue Syndrome. J Autoimmune Dis. (2005) 2:5. doi: 10.1186/1740-2557-2-5
11. Elfaitouri A, Herrmann B, Bolin-Wiener A, Wang Y, Gottfries CG, Zachrisson O, et al. Epitopes of microbial and human heat shock protein 60 and their recognition in myalgic encephalomyelitis. PLoS ONE. (2013) 8:e81155. doi: 10.1371/journal.pone.0081155
12. Hokama Y, Campora CE, Hara C, Kuribayashi T, Le Huynh D, Yabusaki K. Anticardiolipin antibodies in the sera of patients with diagnosed chronic fatigue syndrome. J Clin Lab Anal. (2009) 23:210–2. doi: 10.1002/jcla.20325
13. Hokama Y, Empey-Campora C, Hara C, Higa N, Siu N, Lau R, et al. Acute phase phospholipids related to the cardiolipin of mitochondria in the sera of patients with chronic fatigue syndrome (CFS), chronic Ciguatera fish poisoning (CCFP), and other diseases attributed to chemicals, Gulf War, and marine toxins. J Clin Lab Anal. (2008) 22:99–105. doi: 10.1002/jcla.20217
14. Maes M, Mihaylova I, Leunis JC. Chronic fatigue syndrome is accompanied by an IgM-related immune response directed against neopitopes formed by oxidative or nitrosative damage to lipids and proteins. Neuro Endocrinol Lett. (2006) 27:615–21.
15. Maes M, Mihaylova I, Kubera M, Leunis JC, Twisk FN, Geffard M. IgM-mediated autoimmune responses directed against anchorage epitopes are greater in Myalgic Encephalomyelitis/Chronic Fatigue Syndrome (ME/CFS) than in major depression. Metab Brain Dis. (2012) 27:415–23. doi: 10.1007/s11011-012-9316-8
16. Maes M, Mihaylova I, Kubera M, Leunis JC. An IgM-mediated immune response directed against nitro-bovine serum albumin (nitro-BSA) in chronic fatigue syndrome (CFS) and major depression: evidence that nitrosative stress is another factor underpinning the comorbidity between major depression and CFS. Neuro Endocrinol Lett. (2008) 29:313–9.
17. Halpin P, Williams MV, Klimas NG, Fletcher MA, Barnes Z, Ariza ME. Myalgic encephalomyelitis/chronic fatigue syndrome and gulf war illness patients exhibit increased humoral responses to the herpesviruses-encoded dUTPase: Implications in disease pathophysiology. J Med Virol. (2017) 89:1636–45. doi: 10.1002/jmv.24810
18. Scheibenbogen C, Loebel M, Freitag H, Krueger A, Bauer S, Antelmann M, et al. Immunoadsorption to remove b2 adrenergic receptor antibodies in Chronic Fatigue Syndrome CFS/ME. PLoS ONE. (2018) 13:e0193672. doi: 10.1371/journal.pone.0193672
19. Schutzer SE, Angel TE, Liu T, Schepmoes AA, Clauss TR, Adkins JN, et al. Distinct cerebrospinal fluid proteomes differentiate post-treatment lyme disease from chronic fatigue syndrome. PLoS ONE. (2011) 6:e17287. doi: 10.1371/journal.pone.0017287
20. Blomberg J, Rizwan M, Böhlin-Wiener A, Elfaitouri A, Julin P, Zachrisson O, et al. Antibodies to human herpesviruses in myalgic encephalomyelitis/chronic fatigue syndrome patients. Front Immunol. (2019) 10:1946. doi: 10.3389/fimmu.2019.01946
21. Fluge O, Mella O, Bruland O, Risa K, Dyrstad SE, Alme K, et al. Metabolic profiling indicates impaired pyruvate dehydrogenase function in myalgic encephalopathy/chronic fatigue syndrome. JCI Insight. (2016) 1:e89376. doi: 10.1172/jci.insight.89376
22. Naviaux RK, Naviaux JC, Li K, Bright AT, Alaynick WA, Wang L, et al. Metabolic features of chronic fatigue syndrome. Proc Natl Acad Sci USA. (2016) 113:E5472–80. doi: 10.1073/pnas.1607571113
23. Purohit T, Cappell MS. Primary biliary cirrhosis: pathophysiology, clinical presentation and therapy. World J Hepatol. (2015) 7:926–41. doi: 10.4254/wjh.v7.i7.926
24. Palmer JM, Doshi M, Kirby JA, Yeaman SJ, Bassendine MF, Jones DE. Secretory autoantibodies in primary biliary cirrhosis (PBC). Clin Exp Immunol. (2000) 122:423–8. doi: 10.1046/j.1365-2249.2000.01403.x
25. Kadaja L, Kisand KE, Peet N, Braun U, Metskula K, Teesalu K, et al. IgG from patients with liver diseases inhibit mitochondrial respiration in permeabilized oxidative muscle cells: impaired function of intracellular energetic units? Mol Cell Biochem. (2004) 256–257:291–303. doi: 10.1023/B:MCBI.0000009876.23921.e6
26. Zachrisson O, Regland B, Jahreskog M, Kron M, Gottfries CG. A rating scale for fibromyalgia and chronic fatigue syndrome (the FibroFatigue scale). J Psychosom Res. (2002) 52:501–9. doi: 10.1016/S0022-3999(01)00315-4
27. Thomson RK, Davis Z, Palmer JM, Arthur MJ, Yeaman SJ, Chapman CJ, et al. Immunogenetic analysis of a panel of monoclonal IgG and IgM anti-PDC-E2/X antibodies derived from patients with primary biliary cirrhosis. J Hepatol. (1998) 28:582–94. doi: 10.1016/S0168-8278(98)80281-X
28. Smyk DS, Rigopoulou EI, Bogdanos DP. Potential roles for infectious agents in the pathophysiology of primary biliary cirrhosis: what's new? Curr Infect Dis Rep. (2013) 15:14–24. doi: 10.1007/s11908-012-0304-2
29. Wang JJ, Yang GX, Zhang WC, Lu L, Tsuneyama K, Kronenberg M, et al. Escherichia coli infection induces autoimmune cholangitis and anti-mitochondrial antibodies in non-obese diabetic (NOD).B6 (Idd10/Idd18) mice. Clin Exp Immunol. (2014) 175:192–201. doi: 10.1111/cei.12224
30. Tanaka A, Leung PSC, Gershwin ME. Pathogen infections and primary biliary cholangitis. Clin Exp Immunol. (2019) 195:25–34. doi: 10.1111/cei.13198
31. Xu L, Sakalian M, Shen Z, Loss G, Neuberger J, Mason A. Cloning the human betaretrovirus proviral genome from patients with primary biliary cirrhosis. Hepatology. (2004) 39:151–6. doi: 10.1002/hep.20024
32. Tanaka T, Zhang W, Sun Y, Shuai Z, Chida AS, Kenny TP, et al. Autoreactive monoclonal antibodies from patients with primary biliary cholangitis recognize environmental xenobiotics. Hepatology. (2017) 66:885–95. doi: 10.1002/hep.29245
33. Newton JL, Davidson A, Kerr S, Bhala N, Pairman J, Burt J, et al. Autonomic dysfunction in primary biliary cirrhosis correlates with fatigue severity. Eur J Gastroenterol Hepatol. (2007) 19:125–32. doi: 10.1097/01.meg.0000252629.96043.67
34. Sotzny F, Blanco J, Capelli E, Castro-Marrero J, Steiner S, Murovska M, et al. Myalgic Encephalomyelitis/Chronic Fatigue Syndrome - Evidence for an autoimmune disease. Autoimmun Rev. (2018) 17:601–9. doi: 10.1016/j.autrev.2018.01.009
35. Torrente-Segarra V, Salman-Monte TC, Rua-Figueroa I, Perez-Vicente S, Lopez-Longo FJ, Galindo-Izquierdo M, et al. Fibromyalgia prevalence and related factors in a large registry of patients with systemic lupus erythematosus. Clin Exp Rheumatol. (2016) 34(2 Suppl 96):40–7.
36. Bazzichi L, Rossi A, Zirafa C, Monzani F, Tognini S, Dardano A, et al. Thyroid autoimmunity may represent a predisposition for the development of fibromyalgia? Rheumatol Int. (2012) 32:335–41. doi: 10.1007/s00296-010-1620-1
37. Keech A, Sandler CX, Vollmer-Conna U, Cvejic E, Lloyd AR, Barry BK. Capturing the post-exertional exacerbation of fatigue following physical and cognitive challenge in patients with chronic fatigue syndrome. J Psychosom Res. (2015) 79:537–49. doi: 10.1016/j.jpsychores.2015.08.008
38. Shungu DC, Weiduschat N, Murrough JW, Mao X, Pillemer S, Dyke JP, et al. Increased ventricular lactate in chronic fatigue syndrome. III. Relationships to cortical glutathione and clinical symptoms implicate oxidative stress in disorder pathophysiology. NMR Biomed. (2012) 25:1073–87. doi: 10.1002/nbm.2772
39. Lien K, Johansen B, Veierod MB, Haslestad AS, Bohn SK, Melsom MN, et al. Abnormal blood lactate accumulation during repeated exercise testing in myalgic encephalomyelitis/chronic fatigue syndrome. Physiol Rep. (2019) 7:e14138. doi: 10.14814/phy2.14138
40. Weinberg SE, Sena LA, Chandel NS. Mitochondria in the regulation of innate and adaptive immunity. Immunity. (2015) 42:406–17. doi: 10.1016/j.immuni.2015.02.002
41. Morris G, Berk M, Galecki P, Walder K, Maes M. The neuro-immune pathophysiology of central and peripheral fatigue in systemic immune-inflammatory and neuro-immune diseases. Mol Neurobiol. (2016) 53:1195–219. doi: 10.1007/s12035-015-9090-9
42. Tyurina YY, Shrivastava I, Tyurin VA, Mao G, Dar HH, Watkins S, et al. “Only a life lived for others is worth living”: redox signaling by oxygenated phospholipids in cell fate decisions. Antioxid Redox Signal. (2018) 29:1333–58. doi: 10.1089/ars.2017.7124
43. Ingelsson B, Söderberg D, Strid T, Söderberg A, Bergh AC, Loitto V, et al. Lymphocytes eject interferogenic mitochondrial DNA webs in response to CpG and non-CpG oligodeoxynucleotides of class C. Proc Natl Acad Sci USA. (2018) 115:E478–87. doi: 10.1073/pnas.1711950115
44. Germain A, Barupal DK, Levine SM, Hanson MR. Comprehensive circulatory metabolomics in ME/CFS reveals disrupted metabolism of acyl lipids and steroids. Metabolites. (2020) 10:34. doi: 10.3390/metabo10010034
45. Zhang S, Hulver MW, McMillan RP, Cline MA, Gilbert ER. The pivotal role of pyruvate dehydrogenase kinases in metabolic flexibility. Nutr Metab. (2014) 11:10. doi: 10.1186/1743-7075-11-10
46. Solmonson A, DeBerardinis RJ. Lipoic acid metabolism and mitochondrial redox regulation. J Biol Chem. (2018) 293:7522–30. doi: 10.1074/jbc.TM117.000259
Keywords: myalgic encephalomyelitis/chronic fatigue syndrome, anti-pyruvate dehydrogenase complex antibodies, PDC, anti-mitochondrial autoantibodies, AMA
Citation: Nilsson I, Palmer J, Apostolou E, Gottfries C-G, Rizwan M, Dahle C and Rosén A (2020) Metabolic Dysfunction in Myalgic Encephalomyelitis/Chronic Fatigue Syndrome Not Due to Anti-mitochondrial Antibodies. Front. Med. 7:108. doi: 10.3389/fmed.2020.00108
Received: 18 October 2019; Accepted: 10 March 2020;
Published: 31 March 2020.
Edited by:
Paul Robert Fisher, La Trobe University, AustraliaReviewed by:
Geraldine Cambridge, University College London, United KingdomØystein Fluge, Haukeland University Hospital, Norway
Copyright © 2020 Nilsson, Palmer, Apostolou, Gottfries, Rizwan, Dahle and Rosén. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Anders Rosén, YW5kZXJzLnJvc2VuQGxpdS5zZQ==