 Graziella Orrù
Graziella Orrù Angelo Gemignani1
Angelo Gemignani1 Ciro Conversano
Ciro Conversano
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
BRIEF RESEARCH REPORT article
Front. Med. , 13 January 2020
Sec. Rheumatology
Volume 6 - 2019 | https://doi.org/10.3389/fmed.2019.00319
Here, we report an investigation on the accuracy of the Toronto Alexithymia Scale, a measure to assess alexithymia, a multidimensional construct often associate to fibromyalgia. Two groups of participants, patients with fibromyalgia (n = 38), healthy controls (n = 38) were administered the Toronto Alexithymia Scale and background tests. Machine learning models achieved an overall accuracy higher than 80% in detecting both patients with fibromyalgia and healthy controls. The parameter which alone has demonstrated maximum efficiency in classifying the single subject within the two groups has been the item 3 of the alexithymia scale. The analysis of the most informative features, based on all scales administered, revealed that item 3 and 13 of the alexithymia questionnaire and the visual analog scale scores were the most informative attributes in correctly classifying participants (accuracy above 85%). An additional analyses using only the alexithymia scale subset of items and the visual analog scale scores has shown that the predictors which efficiently classified patients with fibromyalgia and controls were the item 3 and 7 (accuracy = 85.53%). Our findings suggest that machine learning models analysis based on the Toronto Alexithymia Scale subset of items scores accurately distinguish patients with fibromyalgia from healthy controls.
Fibromyalgia syndrome (FMS) has widely been defined as a chronic condition characterized by aching, pain or stiffness in the muscles or joints, and the presence of muscles tenderness (1). The symptoms of fibromyalgia can vary and are similar to those of several other conditions. The literature has suggested that along with the physical symptoms, FMS can be manifest with features belonging to the psychological domains such as depression, anxiety, sleep disorders, fatigue, pain, alexithymia, and functional difficulty of daily living activities (2, 3). In regard to the relationship between depression and FMS, a recent research (4) suggested a shared pathophysiology between the two and demonstrated a bidirectional temporal association which means that the first disease occurring may increase the risk to develop the other. Moreover, a recent study found that pain severity, pain catastrophizing, and fear of movement are influenced by depression and anxiety levels in FMS patients, while fatigue and sleep disturbance may be associated only with depression. Furthermore, both depression and anxiety did not have an amplifying influence on one another when related to somatic and psychological variables (5).
While several psychological domains in FMS patients have been extensively studied, others have been poorly investigated. Among the psychological factors, alexithymia is a personality construct characterized by the “absence of words for emotion” which has been minimally explored in FM but is worth examining, as it can negatively impact the perception of emotional sensations. A recent critical review (6), investigating the presence of alexithymia in patients with FMS, highlighted the high prevalence of alexithymia in FM patients. Although the influence of the alexithymic aspect on patients with FMS is not yet clear, it is possible to mention some of the most reliable hypotheses. Alexithymia and FMS share several factors, including a close link with trauma and dissociation as a defense mechanism. In fact, several authors have confirmed the role of traumatic experiences on the onset and the presence of fibromyalgia as well as in individuals with alexithymia (7, 8). Individuals with alexithymia seem to confer much more weight to the physical sensation of arousal instead of interpreting it, which remains suspended somehow. This factor could cause, in FM patients, a considerable distress, the inability to define and integrate emotions, leading to negative consequences regarding social integration and self-acceptance (9).
To date it is possible to affirm that there is no univocal relationship between the two aspects, but that alexithymia leads to an altered interpretation of some emotions and a worsening of the quality of life. Furthermore, a few factors such as pain perception, presence of anxiety, high level of catastrophization, and distress in patients with FMS, should bring the clinicians and health experts back to the importance of the patients' emotional health (10–12). Moreover, alexithymia seems to be associated with an increased affective pain and hypochondriacal illness behavior in FMS patients, with a mediating effect of psychological distress and illness behavior itself (13). Additionally, some researches highlight that not knowing how to reduce the impact of negative feelings—which is typical in individuals with alexithymia—may increase negative affect and chronic sympathetic hyperarousal impairing consequently the immune system (6, 13).
In order to plan and monitor treatments, an increasing number of studies have tried to identify the individuals' features and experience related to the illness across a variety of long-term chronic conditions such as osteoporosis (14), diabetes (15), chronic pain (16), dementia (17), and FMS (18) using comprehensive relevant questionnaires or outcomes measures provided by the medico-clinical research (19).
In the context of FMS, psychological domains that may negatively influence the quality of life of the individuals affected have been poorly investigated, especially in those with a subthreshold clinical manifestation. Due to subthreshold symptoms and/or because of the similarity of symptoms to those of several other conditions, the objective is to identify whether that individual can be accurately identified based on the results of the relevant tests and questionnaires administered. Clarifying the role of specific psychological features in patients with FMS can thus allow better understanding of the disease etiology, the development of patient-tailored treatments, in which both physical and psychological symptoms have to be considered.
Over the past few years, there has been growing interest within the clinical setting in the use of analytical methods in order to efficiently distinguishing patients from healthy individuals on the sole basis of the scores results, enabling to make inferences at both group and individual level. One such method is supervised machine learning (ML), an area of artificial intelligence concerned with the development of algorithms and techniques able to automatically extract information from the available data. In recent years, it has been shown that psychometric testing may be augmented using ML techniques (20) in different fields application, amongst others in neuroimaging (21), malingering (22, 23), genetics (24), and clinical medicine (25). As far as we know, this is the first time that such methods have been applied to fibromyalgia and related psychological domains of interest. ML models have shown promising advantages in solving classification problems. In our case, the issue we intend to address using ML models is the following: Which are the predictors that best distinguish between patients with FMS and healthy controls? In order to guarantee that the reported results are replicable we also evaluated such models using 10-fold cross-validation. Using 10-fold cross-validation the reported results do not suffer from overfitting which yields to overly optimistic results that are not confirmed out of sample. The goal of cross-validation is to test the model's ability to predict new data that was not used in estimating it. The data set is split into 10 folds. In the first iteration, the first fold is used to test the model and the rest are used to train the model. In the second iteration, the second fold is used as the testing set while the rest serve as the training set. This process is repeated until each fold of the 10 folds have been used as the testing set. The average errors an unbiased estimate of the classification accuracy of the model under investigation (26).
Seventy-six Italian speaking subjects (15 men and 61 women; mean age: 49.71 ± 11.25, range 20–73) were recruited for the present study. The clinical sample consisted of two groups, patients with a diagnosis of FMS (n = 38; duration of illness in years: 9.02 ± 6.15, range 1–28), made by an expert rheumatologist, meeting the ACR criteria (27) and healthy controls (HC) (n = 38). HC individuals were usually the patients relatives with no history of chronic pain.
The absence of neurological/psychiatric disorders was confirmed for both samples through anamnesis and clinical interview made by a psychiatrist.
The exclusion criteria for FMS and HC group were the following: (1) age ≤ 18, (2) education level below 5 years; (3) poor knowledge of the Italian Language; (4) presence of neurologic or psychiatric disorders.
Socio-demographic data sheet. The data required were the following: age, gender, years of education, marital status. Additional questions about the participants' current mental-health status were asked.
Self-report questionnaire measures, with established norms, were used. All subjects in the FMS and HC group were assessed using the following questionnaires:
Toronto Alexithymia Scale [TAS-20; (28)]. In order to evaluate the presence of alexithymia, a multidimensional construct often associated to FMS (29), the Italian version of the TAS-20 has been used. The TAS-20 individuals items are reported.
Visual Analog Scale [VAS; (30)] and the Italian adaptation of the McGill Pain Questionnaire (31), named “Questionario Italiano sul Dolore” [QUID; (32)] were used to assess the presence, level and type of pain. QUID questionnaire has been administered to evaluate different dimensions of the pain experience: sensory (QUID-S), affective (QUID-A), evaluative (QUID-E), miscellaneous (QUID-M) components and number of words chosen to describe the pain experience (QUID-NWC).
The Italian version of the Hospital Anxiety and Depression Scale [HADS; (33, 34)] was used in order to evaluate symptoms of psychological distress.
FMS patients were recruited at the University of Pisa Hospital (Rheumatology Unit). The HC group was recruited from patients' partners or relatives that accompanied them to visit. The study was approved by Hospital of Pisa Ethics Committee and was conducted in accordance with the Declaration of Helsinki. All the participants gave their written informed consent before to participate in the study.
Data analysis has been performed using SPSS and Weka 3.8 (35).
t-test has been performed and based on the t values and sample size of the two groups (FMS, n = 38; HC, n = 38), the effects sizes (d) have been derived through Borenstein's formula (36). The suggestions of Cohen (37) for interpreting the magnitude of effect sizes were the following intervals: 0.0–0.1 (no effect), 0.2–0.4 (small effect), 0.5–0.7 (intermediate effect), 0.8–≥1 (large effect).
In order to evaluate the effectiveness of the TAS-20, the predictors used in developing the machine learning (ML) models were the following: age, education, gender, TAS-20 subset of items, VAS, HADS, and QUID components. The k-fold cross validation technique was used. Specifically, the k = 10 has been used, where the value for k is fixed to 10, a value that has been found through experimentation to have a low bias. In fact, this technique is commonly used in the application of ML techniques in order to compare and select a specific model for a given predictive modeling problem and generally the estimates have a lower bias than other methods.
As a first step we run the classifiers including all the predictors. A second step included a preliminary selection of most informative attributes (38). Such feature selection procedure consists in excluding the predictors which do not contribute to the discrimination between the FMS and the HC groups. We also identified the most discriminative predictor using the OneR algorithm (39). Based on the most informative attributes, the best rule that correctly classify the subject in the two groups was obtained by J48 pruned three algorithm (40).
In order to identify the most efficient items of the TAS-20 scale, we isolated the most efficient subset of items of the same scale through the algorithm developed by Hall (38).
Means and standard deviations for age, gender, education, and tests scores are reported in Table 1. t-test has been performed and based on the t values and sample size of the two groups, the effects sizes (d) have been derived through Borenstein's formula. All questionnaire measures considered have shown effect sizes from small to large according to Cohen's interpretation (37) and are shown in Table 2.
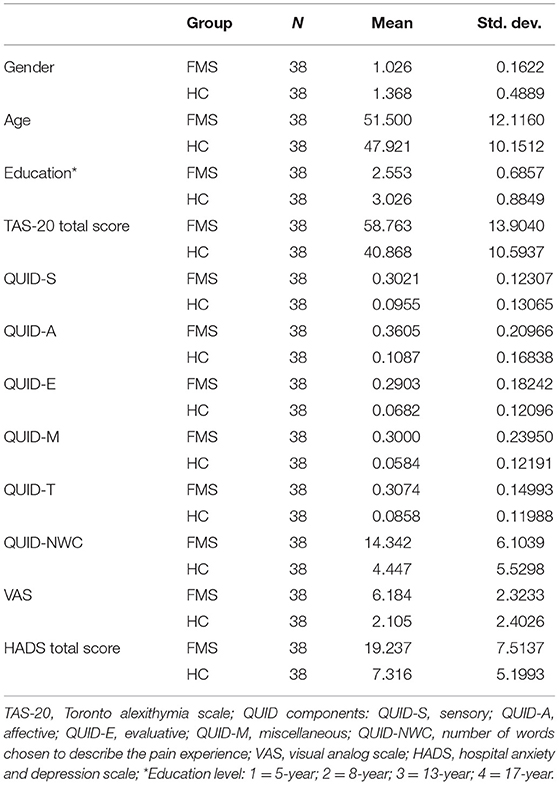
Table 1. Demographic characteristics and performance on the administered tests for each group of participants (FMS and HC groups).

Table 2. t-test and effect sizes (d).
In applying TAS-20, HADS, VAS, QUID scales in a psychological-clinical setting, the most interesting aspect is to identify which are the main features which enable to characterize patients with fibromyalgia (group A) from healthy controls (group B). In order to pursue this aim, we applied ML algorithms. In the classification process, the parameter which alone has demonstrated maximum efficiency, amongst all domains and subdomains considered, in classifying the single subject within the two groups has been the item three of the TAS-20 (item 3), where the cut-off has been identified through oneR, which yielded an accuracy of 84.21% and the rule was the following:
if the TAS-20 (item 3) score is < 3.5, then the subject is classified as a control subject;
and
if the TAS-20 (item 3) score is ≥ 3.5, then the subject is classified as a FMS patient.
The reported decision rule is not the best classifier, but it gives a better understanding of the principle, which results in high accuracy in classifying FMS (31/38; accuracy = 81%) and HC subjects (33/38; accuracy = 87%), AUC = 0.84 (d = 1.41) and F1 = 0.84.
In Table 3 are displayed the accuracies demonstrated by 5 different classifiers: Naïve Bayes, Logistic Regression, Simple Logistics, Support Vector Machine, Random Forest (using 10-fold cross-validation and 5-fold cross-validation). Classifiers were run with default parameters of Weka and therefore without any parameter tuning.
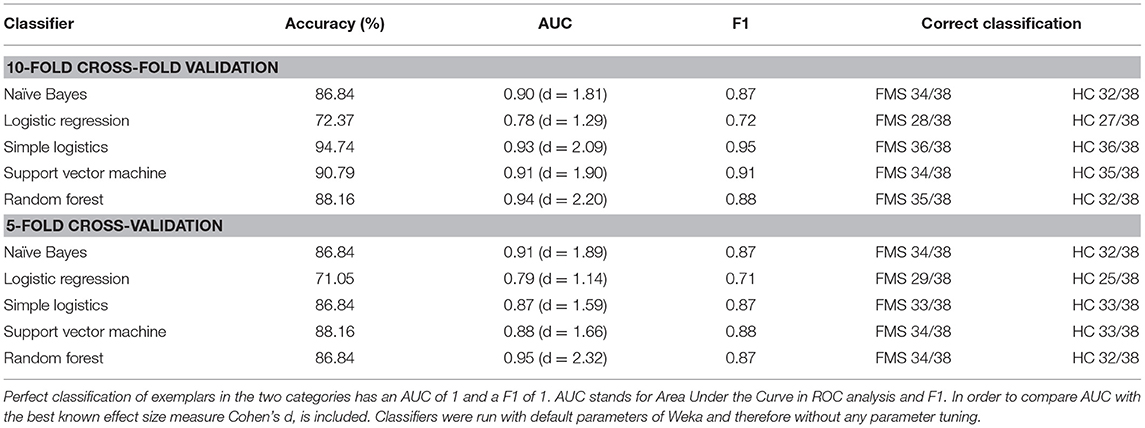
Table 3. Accuracies as measured by % correct, AUC, F1, and correct classification obtained by five different ML classifiers (using 10-fold cross-validation and 5-fold cross-validation).
In order to identify the most informative features based on the domains and subdomains administered, we run the classifiers using as input the best informative attributes.
In this dataset, classification accuracy was increased by a preliminary selection of the most informative input features (38). In Table 4 are displayed the accuracies achieved by 5 different classifiers with the preliminary best attributes selection.
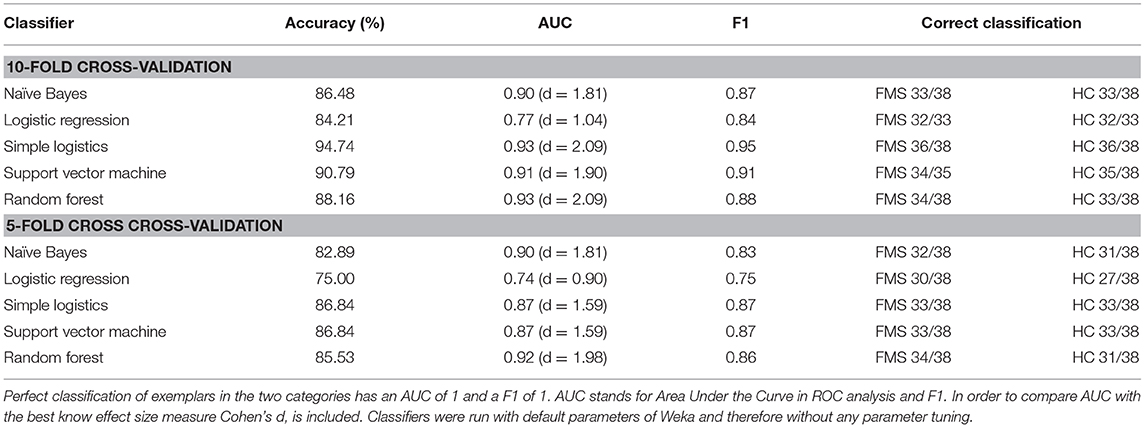
Table 4. Accuracies as measured by % correct, AUC, and F1 obtained by five different ML classifiers (using 10-fold cross-validation and 5-fold cross-validation) with a preliminary best attributes selection.
In order to have insight of the best rule, based on the attributes selected classifier, J48 pruned three algorithm (using 10-fold cross validation), that correctly classify the subject in the two groups yielding an overall accuracy of 85.53%, the rule was the following:
if TAS-20 (item 3) score is ≤ 3:
and VAS score ≤ 5, then the subject is classified as a control subject;
and VAS score >5, and TAS-20 (item 13) score is ≤ 1, then the subject is classified as a FMS patient;
and VAS score >5, and TAS-20 (item 13) score is >1, then the subject is classified as a control subject.
and
if TAS-20 (item 3) score is > 3:
and the gender is =F, then the subject is classified as a FMS patient;
and the gender is =M, then the subject is classified as control subject.
Note that this is a rule which has different separated nested single and composed rules. The reported decision rule results in high accuracy in classifying FMS (33/38; accuracy = 87%) and HC subjects (32/38; accuracy = 84%), AUC = 0.82 (d = 1.29) and F1 = 0.85.
When considering the previous tests and subscales scores, the single most efficient rule was obtained by J48 classifier (using 10-fold cross validation) that correctly classify the subjects in the two groups (FMS and HC) yielding an overall accuracy of 85.53%, where the rule highlighted the most sensitive scales were TAS-20 and VAS. In order to predict which of the TAS-20 subscales and cut-offs and VAS scale cut-off may be used as the single best predictor, we have considered the following subscales and features: TAS-20 (1–20 items), VAS total score, gender, and age. For this analysis, we have removed the gender, given that the sample was unbalance for variable (61 females, 15 males). The single most efficient rule was obtained by J48 algorithm, that correctly classifies the subjects in the two groups, yielded an overall accuracy of 88.16% (AUC = 0.88; d = 1.66; F1 = 0.88) and was the following:
if TAS-20 (item 3) score is ≤ 3:
and VAS score ≤ 5, then the subject is classified as a control subject;
and VAS score >5, then the subject is classified as a FMS patient;
and
if TAS-20 (item 3) score is > 3:
and TAS-20 (item 7) is ≤ 1, then the subject is classified as a control subject;
and TAS-20 (item 7) is >1, then the subject is classified as a FMS patient.
In order to identify the most efficient items of the TAS-20 scale, we isolated the most efficient subset of items of the same scale through the algorithm developed by Hall (38), which identified those features highly correlated with the group and lower correlated among themselves. The TAS-20 subset items which better correlate with Fibromyalgia through attributes selection (10-fold cross-validation, stratified) were the following items: 1, 3, 7, 13, 14, and 15.
As far as we know, this is the first time that ML methods have been applied to fibromyalgia and related psychological domains. ML models have shown promising advantages in solving classification problems. The issue we intended to address using ML models was the following: which are the predictors that best distinguish between patients with FMS and healthy controls? Currently, clinical and research efforts have led to increasingly sophisticated methods to characterize and detect subthreshold alexithymia in patient with fibromyalgia, nevertheless there are still significant theoretical and practical challenges. Conventional statistical analysis doesn't allow to identify decision roles with a powerful translational effect in the clinical setting. The employment of the ML techniques allow to identify the best principles compare to the inferential statistic, which are both diagnostic rules and the accuracy. Models easily interpretable as those based on decision principles have allowed to identify decisional roles with a slightly reduction of accuracy. These decisional principles use the tests scores to detect the best predictors and rules useful by clinicians in the clinical practice.
Our study support the hypothesis that machine learning increases diagnosticity in psychometric evaluation of alexithymia in fibromyalgic patients.
The traditional statistical analysis has shown that all variables and scales considered have significant effect, ranging from small effect sizes to large effect, according to Cohen's interpretation (37). On the contrary classifications based on ML techniques reached higher accuracies, in the range of 84.21–88.16% with opaque classifiers and were able to (i) correctly classifies the subjects in the two groups (FMS and HC); (ii) to identified the subset of items which better correlate with the FMS group.
Our findings suggest that machine learning models analysis based on the TAS-20 subset of items scores accurately distinguish patients with fibromyalgia from healthy controls. The single most efficient rule, using only TAS subscales and VAS score as predictors of two classes, was obtained by J48 algorithm, that correctly classifies the subjects in the two groups, yielded an overall accuracy of 88.16% (AUC = 0.88; d = 1.66; F1 = 0.88).
The present research found that the vast majority of individual TAS-20 items (i.e., item 1, 3, 7, 13, 14, 15) that better correlated with fibromyalgia fell into the “Difficulty Identifying Feelings” feelings subscale of the alexithymia construct. These results may highlight the presence of a greater difficulty in identifying and expressing emotions and externally oriented thinking in patients with FMS compared to general population. Alexithymia as an emotional dysregulation trait, could play an important role in FM syndrome where individuals are less capable of adequately identifying physical sensations (i.e., somatic manifestations of emotions) leading them to misinterpret their emotional arousal as signs of disease (41, 42). This could amplify the perception of disease, bringing patients to seek medical care for symptoms for which there is no medical explanation.
Future replications in medico-clinical settings using participants with fibromyalgia are needed in order to corroborate our results.
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation, to any qualified researcher.
The studies involving human participants were reviewed and approved by the Hospital of Pisa Ethics Committee and was conducted in accordance with the Declaration of Helsinki. All participants gave their written informed consent before participating in the study. The patients/participants provided their written informed consent to participate in this study.
CC and LB conceived the assessment. RC contributed to the data acquisition. GO contributed to the data analysis and data interpretation. GO, CC, LB, and AG drafted the manuscript. RC implemented the introduction associated with fibromyalgia and alexhitymia. All authors revised the manuscript and approved the final version to be published.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
We thank Simona Lemmetti, Laura Marchi, and Francesca Marzetti, who contributed to healthy and fibromyalgic patients data acquisition.
2. Gerdle B, Björk J, Cöster L, Henriksson KG, Henriksson C, Bengtsson A. Prevalence of widespread pain and associations with work status: a population study. BMC Musculoskelet Disord. (2008) 9:102. doi: 10.1186/1471-2474-9-102
3. Jahan F, Nanji K, Qidwai W, Qasim R. Fibromyalgia syndrome: an overview of pathophysiology, diagnosis and management. Oman Med J. (2012) 27:192. doi: 10.5001/omj.2012.44
4. Chang MH, Hsu JW, Huang KL, Su TP, Bai YM, Li CT, et al. Bidirectional association between depression and fibromyalgia syndrome: a nationwide longitudinal study. J Pain. (2015) 16:895–902. doi: 10.1016/j.jpain.2015.06.004
5. Hadlandsmyth K, Dailey DL, Rakel BA, Zimmerman MB, Vance CG, Merriwether EN, et al. Somatic symptom presentations in women with fibromyalgia are differentially associated with elevated depression and anxiety. J Health Psychol. (2017) 1359105317736577. doi: 10.1177/1359105317736577
6. Di Tella M, Castelli L. Alexithymia and fibromyalgia: clinical evidence. Front Psychol. (2013) 4:909. doi: 10.3389/fpsyg.2013.00909
7. Waller E, Scheidt CE, Endorf K, Hartmann A, Zimmermann P. Unresolved trauma in fibromyalgia: a cross-sectional study. J Health Psychol. (2016) 21:2457–65. doi: 10.1177/1359105315580460
8. Al-Allaf AW, Dunbar KL, Hallum NS, Nosratzadeh B, Templeton KD, Pullar T. A case–control study examining the role of physical trauma in the onset of fibromyalgia syndrome. Rheumatology. (2002) 41:450–3. doi: 10.1093/rheumatology/41.4.450
9. Taylor GJ, Bagby RM, Parker JD. Disorders of Affect Regulation: Alexithymia in Medical and Psychiatric Illness Cambridge: Cambridge University Press (1999).
10. Di Tella M, Enrici I, Castelli L, Colonna F, Fusaro E, Ghiggia A, et al. Alexithymia, not fibromyalgia, predicts the attribution of pain to anger-related facial expressions. J Affect Disord. (2018) 227:272–9. doi: 10.1016/j.jad.2017.10.048
11. Di Tella M, Ghiggia A, Tesio V, Romeo A, Colonna F, Fusaro E, et al. Pain experience in Fibromyalgia syndrome: the role of alexithymia and psychological distress. J Affect Disord. (2017) 208:87–93. doi: 10.1016/j.jad.2016.08.080
12. Romagnolli L, Coria VR, Júnior SHN, Sartori JET, de Souza Romanelli A, Carvalho LGGS, et al. Alexithymia and fibromyalgia: a systematic review. Rev Med. (2016) 95:12–7. doi: 10.11606/issn.1679-9836.v95i1p12-17
13. Huber A, Suman AL, Biasi G, Carli G. Alexithymia in fibromyalgia syndrome: associations with ongoing pain, experimental pain sensitivity and illness behavior. J Psychosom Res. (2009) 66:425–33. doi: 10.1016/j.jpsychores.2008.11.009
14. Catalano A, Martino G, Bellone F, Gaudio A, Lasco C, Langher V, et al. Anxiety levels predict fracture risk in postmenopausal women assessed for osteoporosis. Menopause. (2018) 25:1110–5. doi: 10.1097/GME.0000000000001123
15. Settineri S, Frisone F, Merlo EM, Geraci D, Martino G. Compliance, adherence, concordance, empowerment, and self-management: five words to manifest a relational maladjustment in diabetes. J Multidiscip Healthc. (2019) 12:299. doi: 10.2147/JMDH.S193752
16. Catalano A, Martino G, Morabito N, Scarcella C, Gaudio A, Basile G, et al. Pain in osteoporosis: from pathophysiology to therapeutic approach. Drugs Aging. (2017) 34:755–65. doi: 10.1007/s40266-017-0492-4
17. Orru G, Sampietro S, Catanzaro S, Girardi A, Najjar M, Giantin V, et al. Serial position effect in a free recall task: differences between probable dementia of Alzheimer type (PDAT), vascular (VaD) and mixed etiology dementia (MED). Arch Gerontol Geriatr. (2009) 49:207–10. doi: 10.1016/j.archger.2009.09.030
18. Lee JW, Lee KE, Park DJ, Kim SH, Nah SS, Lee JH, et al. Determinants of quality of life in patients with fibromyalgia: a structural equation modeling approach. PLoS ONE. (2017) 12:e0171186. doi: 10.1371/journal.pone.0171186
19. Coin A, Najjar M, Catanzaro S, Orru G, Sampietro S, Sergi G, et al. A retrospective pilot study on the development of cognitive, behavioral and functional disorders in a sample of patients with early dementia of Alzheimer type. Arch Gerontol Geriatr. (2009) 49:35–8. doi: 10.1016/j.archger.2009.09.010
20. James G, Witten D, Hastie T, Tibshirani R. An Introduction to Statistical Learning. Vol. 112. New York, NY: Springer. (2013). 18 p. doi: 10.1007/978-1-4614-7138-7
21. Orru G, Pettersson-Yeo W, Marquand AF, Sartori G, Mechelli A. Using support vector machine to identify imaging biomarkers of neurological and psychiatric disease: a critical review. Neurosci Biobehav Rev. (2012) 36:1140–52. doi: 10.1016/j.neubiorev.2012.01.004
22. Mazza C, Monaro M, Orrù G, Burla F, Colasanti M, Ferracuti S, et al. Introducing machine learning to detect personality faking-good: a new model based on MMPI-2-RF scales and reaction times. Front Psychiatry. (2019) 10:389. doi: 10.3389/fpsyt.2019.00389
23. Pace G, Orrù G, Monaro M, Gnoato F, Vitaliani R, Gemignani A, et al. Malingering detection of cognitive impairment with the B test is boosted using machine learning. Front Psychol. (2019) 10:1650. doi: 10.3389/fpsyg.2019.01650
24. Libbrecht MW, Noble WS. Machine learning applications in genetics and genomics. Nat Rev Genet. (2015) 16:321. doi: 10.1038/nrg3920
25. Obermeyer Z, Emanuel EJ. Predicting the future—big data, machine learning, and clinical medicine. New Engl J Med. (2016) 375:1216. doi: 10.1056/NEJMp1606181
26. Cawley GC, Talbot NL. On over-fitting in model selection and subsequent selection bias in performance evaluation. J Mach Learn Res. (2010) 11:2079–107.
27. Wolfe F, Clauw DJ, Fitzcharles MA, Goldenberg DL, Häuser W, Katz RS, et al. Fibromyalgia criteria and severity scales for clinical and epidemiological studies: a modification of the ACR preliminary diagnostic criteria for fibromyalgia. J Rheumatol. (2011) 38:1113–22. doi: 10.3899/jrheum.100594
28. Bressi C, Taylor G, Parker J, Bressi S, Brambilla V, Aguglia E, et al. Cross validation of the factor structure of the 20-item Toronto Alexithymia Scale: an Italian multicenter study. J Psychosom Res. (1996) 41:551–9. doi: 10.1016/S0022-3999(96)00228-0
29. Marchi L, Marzetti F, Orrù G, Lemmetti S, Miccoli M, Ciacchini R, et al. Alexithymia and psychological distress in patients with fibromyalgia and rheumatic disease. Front Psychol. (2019) 10:1735. doi: 10.3389/fpsyg.2019.01735
30. McCormack HM, David JDL, Sheather S. Clinical applications of visual analogue scales: a critical review. Psychol Med. (1988) 18:1007–19. doi: 10.1017/S0033291700009934
31. Melzack R. The McGill pain questionnaire: major properties and scoring methods. Pain. (1975) 1:277–99. doi: 10.1016/0304-3959(75)90044-5
32. De Benedittis G, Massei R, Nobili R, Pieri A, Corli O. Il questionario italiano del dolore (QUID). Algos. (1988) 5:50.
33. Costantini M, Musso M, Viterbori P, Bonci F, Del Mastro L, Garrone O, et al. Detecting psychological distress in cancer patients: validity of the Italian version of the Hospital Anxiety and Depression Scale. Support Care Cancer. (1999) 7:121–7. doi: 10.1007/s005200050241
34. Zigmond AS, Snaith RP. The hospital anxiety and depression scale. Acta Psychiatr Scand. (1983) 67:361–70. doi: 10.1111/j.1600-0447.1983.tb09716.x
35. Hall M, Frank E, Holmes G, Pfahringer B, Reutemann P, Witten IH. The WEKA data mining software: an update. ACM SIGKDD Explor Newslett. (2009) 11:10–8. doi: 10.1145/1656274.1656278
36. Borenstein M, Cooper H, Hedges L, Valentine J. Effect sizes for continuous data. In: Cooper H, Hedges LV, Valentine JC, editors. The Handbook of Research Synthesis and Meta-Analysis. Vol. 2. Evanston, IL: Russell Sage Foundation; Northwestern University (2009). p. 221–35.
37. Cohen J. Statistical Power Analysis for the Behavioural Sciences, xxi (New Jersey, NJ: Lawrence Erbaum Associates) (1998).
38. Hall MA. Correlation-based feature subset selection for machine learning (PhD Thesis). University of Waikato, Hamilton, New Zealand (1998).
39. Holte RC. Very simple classification rules perform well on most commonly used datasets. Mach Learn. (1993) 11:63–90. doi: 10.1023/A:1022631118932
41. Lumley MA, Stettner L, Wehmer F. How are alexithymia and physical illness linked? A review and critique of pathways. J Psychosom Res. (1996) 41:505–18. doi: 10.1016/S0022-3999(96)00222-X
Keywords: alexithymia, chronic conditions, fibromyalgia, machine learning, experiment
Citation: Orrù G, Gemignani A, Ciacchini R, Bazzichi L and Conversano C (2020) Machine Learning Increases Diagnosticity in Psychometric Evaluation of Alexithymia in Fibromyalgia. Front. Med. 6:319. doi: 10.3389/fmed.2019.00319
Received: 21 August 2019; Accepted: 16 December 2019;
Published: 13 January 2020.
Edited by:
Ying Ying Leung, Duke-NUS Medical School, SingaporeReviewed by:
Claire Williams, Swansea University, United KingdomCopyright © 2020 Orrù, Gemignani, Ciacchini, Bazzichi and Conversano. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Graziella Orrù, Z3JhemllbGxhLm9ycnVAdW5pcGkuaXQ=
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.