 Jesica Mazza-Stalder1,2*
Jesica Mazza-Stalder1,2* Emilie Chevallier1
Emilie Chevallier1 Onya Opota3
Onya Opota3 Ana Carreira1
Ana Carreira1 Katia Jaton3
Katia Jaton3 Eric Masserey4
Eric Masserey4 Jean Pierre Zellweger5
Jean Pierre Zellweger5 Laurent Pierre Nicod1
Laurent Pierre Nicod1- 1Pulmonary Division, Lausanne University Hospital, University of Lausanne, Lausanne, Switzerland
- 2Vaud Lung Association, Lausanne, Switzerland
- 3Institute of Microbiology, Lausanne University Hospital, University of Lausanne, Lausanne, Switzerland
- 4Public Health Department, Lausanne, Switzerland
- 5Swiss Lung Association, TB Competence Center, Bern, Switzerland
Setting: Studies performed locally in Switzerland in the late eighties reported unsatisfactory treatment outcomes. Better outcomes were observed since the introduction of directly observed therapy (DOT) in the late nineties and improvement in social support in recent years.
Design: retrospective study of treatment outcomes for all tuberculosis (TB) patients notified in Vaud County (VD), Switzerland, between, 1st of January 2010 and 31st of December of 2014.
Results: 375 patients were notified in VD during the study period. The global outcome was successful in 90.1% of patients (338/375). In 183 culture and PCR positive pulmonary TB, the documented cure rate was 57.9% (106/183), and the treatment completion was 59/183 (32.2%), i.e., a treatment success of 90.2%. DOT was applied globally in 234/375 (62.4%) and in 64/67 of the asylum seekers (AS) (95.5%) followed at the dispensary. Treatment outcomes were successful in 60/67 (89.6%) AS.
Discussion: Improvements in tuberculosis outcomes resulted not only from the introduction of DOT in VD in the nineties but also from a change in the management, with increased attention to the social problems faced by the migrants.
Conclusion: A combined medical and social approach of TB care in VD improved treatment outcomes.
Introduction
In Switzerland in 2017, 554 cases of TB were notified to the Swiss Federal Office of Public Health (SFOPH), resulting in a notification rate of 6.5 cases per 100,000 population (1); this rate is fairly stable. Of these TB patients ~23%, are from Swiss origin and around 77% are from foreign-origin, asylum seekers (AS) account for 34% of the foreign-born patients. Among others, the efficient management of TB, as detailed in the END TB strategy of the WHO, implies rapid diagnosis, high cure rate, and avoidance of failure, relapses, and interruptions before the scheduled end of treatment (2, 3). To guarantee that TB cases are rapidly diagnosed, access to health care must be universally offered, and avoid stigmatization (4). Adherence is essential for treatment completion, TB prevention and care, and thus one of the major determinants of treatment outcomes (5). In Switzerland, studies performed in the late eighties described unsatisfactory treatment outcomes with a success rate in VD County not exceeding 70% in patients with complete documentation (63% if patients without documentation are included) (6). A countrywide survey revealed better results but confirmed that the success rate among some subgroups of foreign-born patients, for instance undocumented migrants, was below the expected range (7). Local studies demonstrated that the provision of directly observed therapy (DOT) and a better training of the health care workers caring for TB patients had an important impact on the cure rate. Since then, VD County invested more resources in the management of TB. Our aim is to present the integrated medical and social approach implemented in VD County for the management of TB, and the current outcomes.
Methods
Description of the Cantonal Tuberculosis Health Care System
VD County has a population of 794,000 inhabitants with 33% of foreign-born residents and notifies around 65 cases of TB per year. TB patients are mostly followed by specialists at the TB clinic (TB dispensary or DAT) of the University Hospital of Lausanne. TB notification to the cantonal health authority is mandatory in Switzerland. The physician in charge of the patient declares the new TB cases to the Cantonal health officer who transfers the information to the SFOPH. Diagnostic laboratories, independently, also notify to the cantonal health authority all new strains of M. tuberculosis identified. The TB nurses from the Lung association (a Non Governmental Organisation caring for patients with chronic respiratory diseases) carry out contact investigations if ordered by the cantonal health officer. A medical advisor (a lung specialist) works at both the Lung association and the TB dispensary (DAT) and is available for questions regarding TB diagnosis, treatment, follow up, and contact tracing. Notification of the issue of treatment is requested by SFOPH since 2016 for all TB patients.
Study Population, Data Collection, and Ethics Approval
All TB patients notified in VD County between, 1st of January 2010 and 31st of December of 2014 were eligible for inclusion in our study. Patient's data were obtained using the VD Lung Association records and the electronic medical records at the DAT. A common excel table was elaborated to analyze the data. End of treatment notification results forms for pulmonary culture positive patient were obtained, missing information was obtained directly from medical doctors in charge of the patients (mostly lung or infectious disease specialists) or from the final reports on the electronic medical records of the Hospital. We collected data on age, nationality, type of TB (pulmonary [PTB] or extra-pulmonary [EPTB]), new or retreatment cases, legal resident status, tuberculosis resistance pattern, and follow-up 2 years after the end of treatment. Authorization was obtained from the Ethics Committee of VD County (CER-VD 2017-02300) to review the clinical records and publish the analyzed data. Written informed consent was not required. All patient identifiable information was anonymized.
Outcomes
Treatment outcomes were defined according to the WHO 2013 revised definitions (8). Successful outcomes included cure (documented with bacteriological conversion in culture positive pulmonary TB) and treatment completion (treatment completed without bacteriological confirmation). Unsatisfactory outcomes included treatment failure, lost to follow up and deaths (deaths due to TB or not due to TB). Potentially unsatisfactory outcomes included “transferred out” cases for whom the treatment outcome was unknown.
Microbiology
Acid fast bacilli detection was achieved through a fluorescent auramine-thiazine red staining according to international guidelines (9). Detection of M. tuberculosis complex was achieved either using a real-time PCR targeting the IS6110 on the molecular diagnostic platform of our laboratory of microbiology (10) or using the Xpert MTB/RIF (11). Mycobacterial culture and drug susceptibility test for first-line drugs were achieved in Mycobacteria Growth Indicator Tube. Drug sensitivity testing for second-line anti-TB drugs for MDR- and XDR-TB was performed at the National Reference Center for Tuberculosis (Zurich, Switzerland).
Treatment Administration
Whenever possible, and at least for all patients recently arrived in Switzerland and during the intensive phase, the treatment was administered under DOT, supervised by nurses, be it by a daily visit to the DAT or to a pharmacy close to the living place or in the social environment of the patient. For well-integrated patients with stable living place and no risk of unexpected moving out of the region, the treatment during the continuation phase may have been under self-administration or by collecting the treatment in the pharmacy once a week (with a pill organizer).
Social Support
Every patient with TB diagnosed in the County received a visit from a social worker during the isolation in hospital or within the first 2 weeks of treatment if the patient was at home. Enablers to adherence such as psychosocial, social or financial support were deployed when appropriate as suggested by European standards of tuberculosis care (12–14). Housing closer to the hospital was whenever possible obtained thanks to the networking between the social services and the different structures that provide housing for migrants (15). Interventions to assist and motivate the patients such as providing extra food vouchers, clothes or assistance to travel, were offered, when necessary. Missed appointments were re-scheduled systematically to avoid interruptions while on treatment as proposed by others (16). In case of drug dependency, methadone programs were combined together with TB treatment and DOT (17). Patients missing one DOT appointment received a telephone call or a reminder letter in order to re-establish contact with the TB clinic. To exchange information on DOT, contact tracing, social and financial enablers to improve treatment adherence, we organized monthly meetings with all the different actors of TB care. Enablers and facilitators of treatment adherence are listed in Table 1.
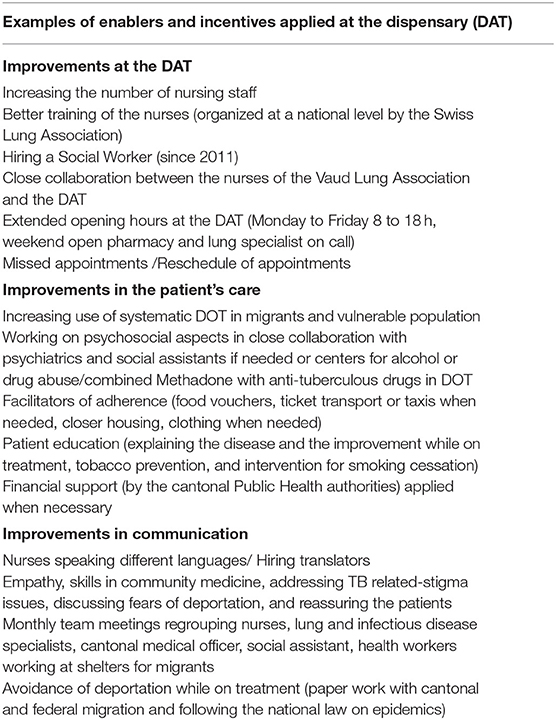
Table 1. Social enablers applied at the DAT to facilitate adherence.
Results
Between January 2010 and December 2014, 375 patients were notified in VD, with a male predominance of 62.1%. The mean age was 38 years (range 1–98) for the whole group and 67 years (3–98) in Swiss patients. There were 288 foreign-born patients (77%) mainly Africans (26.4%), Western Europeans (16.2%), Eastern Europeans (15.7%), and 87 Swiss patients. TB was diagnosed for the first time in 269 patients (72%), 44 patients (12%) had been treated previously and no information on previous treatment was available for 62 patients (17%). Pulmonary tuberculosis (PTB) alone affected 222 patients (59.2%), extra-pulmonary-TB (EPTB) was diagnosed in 103 patients (27. 4%), and both PTB and EPTB was diagnosed in 50 patients (13.4%). Detailed patient's characteristics is reported in Table 2 and sites of disease (PTB and EPTB) in Table 3.
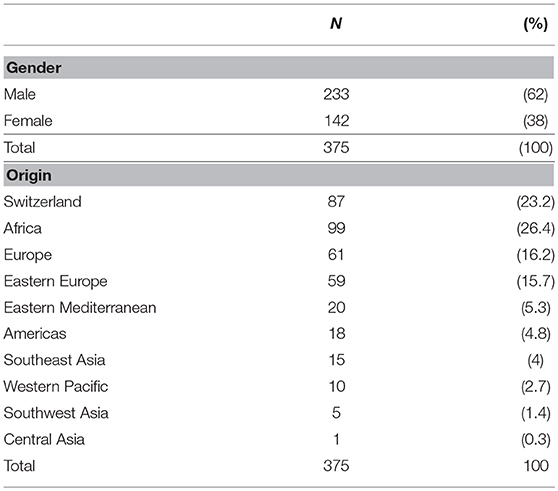
Table 2. Patient's demographics.
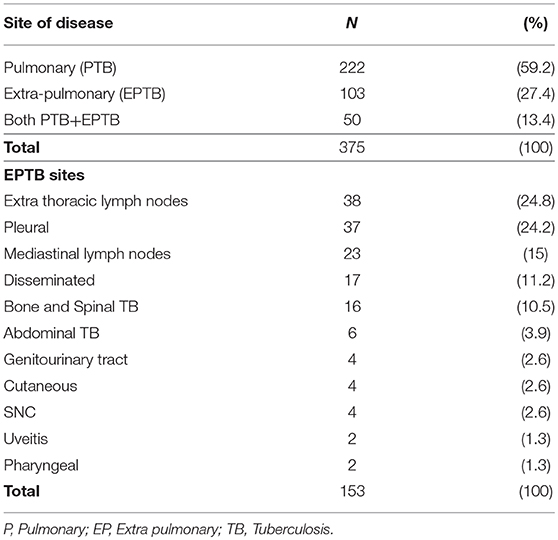
Table 3. Sites of disease.
Microbiological Findings
Cultures were performed in 362 patients (96.5%), not done in 11 patients (3%), and information was missing for 2 patients (0.5%). Among all patients (PTB+ EPTB) culture was positive in 268/375 (71.5%). In patients with PTB only the culture and/or PCR was positive in 183/222 (82.4%) and for EPTB only patients we obtained 80/103 (77.6%) positive samples. We excluded from the analysis the culture positive among the group of PTB+EPTB (n = 41) because we couldn't differentiate the site from which the culture was positive. Among all the TB strains, 265 were M. tuberculosis (98.9%) and 3 were M. bovis (1.1%). Complete microbiological data is reported in Table 4.
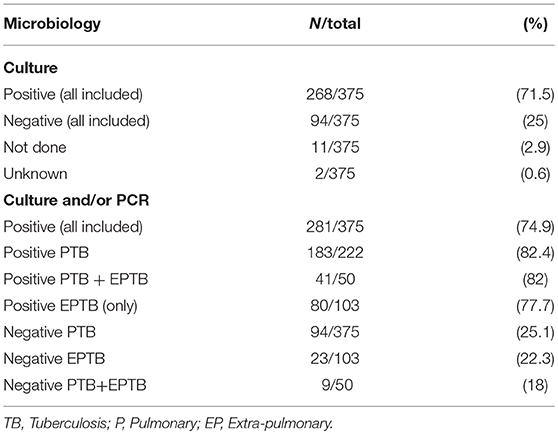
Table 4. Microbiological findings.
Treatment Outcomes
Globally, treatment was successfully completed in 338 patients (90.1%). Among 183 patients with culture or PCR positive PTB (excluding PTB+EPTB), including 10 MDR-TB, the documented cure rate was 106 (57.9%) and the treatment completion was 59 (32.2%), i.e., a global treatment success of 90.2% (n = 165). Among 50 patients with PTB+EPTB tuberculosis, the outcome was successful in 44 (88%). Among 103 patients with EPTB, the treatment completion was 95 (92.2%) (Figure 1).
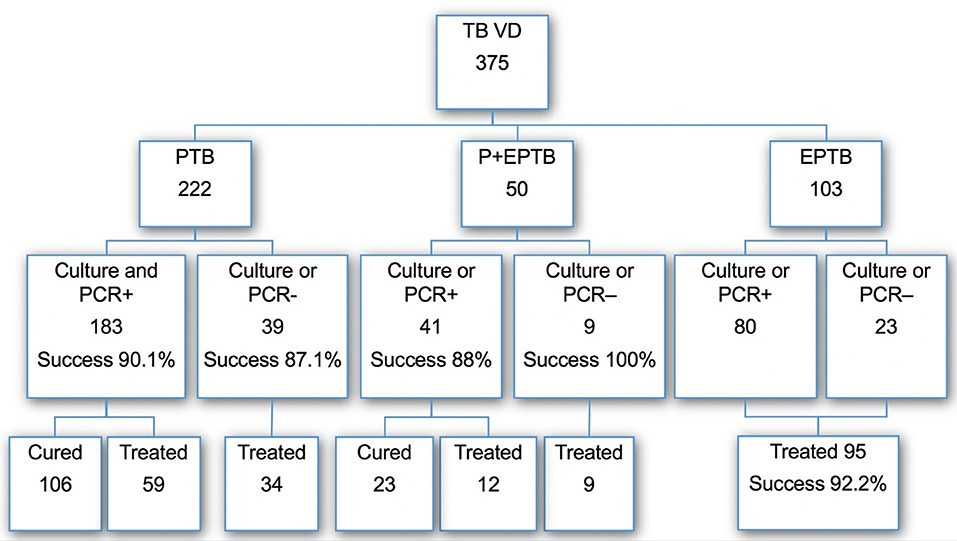
Figure 1. Distribution of TB cases, bacteriological results, and outcome of treatment in each category.
Overall (PTB+EPTB) treatment success among all AS was 79/89 (87.6%). Most AS in VD County were treated at the DAT 67/89 (75.2%) 95.5% of them on DOT (64/67) with a treatment success of 60/67 (89.6%). DOT was applied in 234/375 (62.4%) of our entire study population. We observed no treatment failure. However, 19 patients had unsatisfactory outcomes (5.1%) and 18 potentially unsatisfactory outcomes (4.8%). Among these, we counted 7 persons lost to follow up (1.8%), 12 deaths (3.2%), and 18 transfers while on treatment (4.8%) (Table 5). Within the lost to follow up we counted 7 patients that were part of a very mobile population including 5 AS (2 Georgians, 3 Africans) and 2 foreign-born Europeans (Romanians). Among the 12 that died, 6 died from TB, and 6 died due to comorbidities. Among them 10 patients were Swiss (mean age 69 (49–89), the other two were foreign-born (mean age 52 (23–80). The 23-year-old patient that died while on treatment was an XDR-TB patient who died for causes other than TB. In two elderly Swiss patients (mean age 85) TB was not suspected before death and was diagnosed and notified only after an autopsy. Transmission of TB to health care workers occurred from these 2 undiagnosed patients, one to a nurse and one to a pathologist. Treatment outcomes in DOT vs non DOT is shown in Table 6. Outcomes by categories are shown in Table 7.
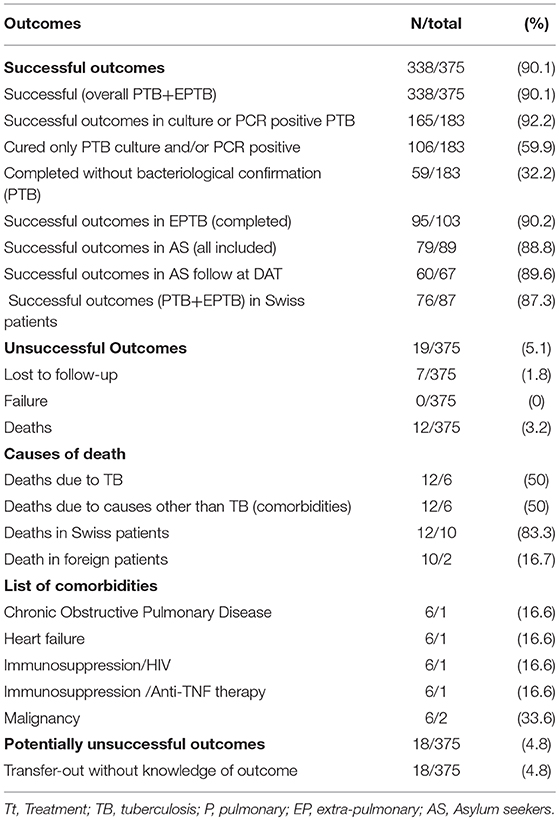
Table 5. Treatment outcomes.
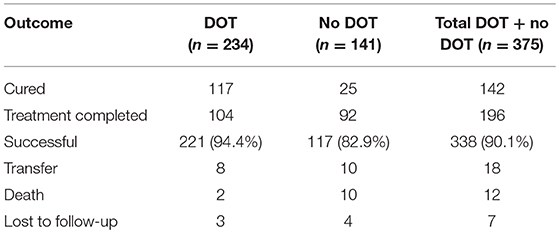
Table 6. Outcomes DOT vs. no DOT.

Table 7. Outcomes by categories.
Follow-Up Visits After Treatment
We followed 178 patients for up to 2 years, 84.2% of these patients were followed at the DAT or at the university hospital in other units (pediatrics and infectious diseases). Relapses were observed in 2 patients, both during the first year after the end of treatment. No relapse was observed after the first year.
Discussion
This retrospective study assessed TB treatment outcomes among patients in VD County during the period 2010–2014, and showed a global success rate of 90.1%. In culture positive pulmonary patients, the cure rate was similar (90.2%). Our success rate is comparable to studies performed at our institution after the implementation of DOT in the late nineties (88.9%) and with publications from St. Gallen in eastern Switzerland (87.5%) (18, 19). Our results are much superior to the historical results of 70% of treatment outcomes previously published by our own institution by Coulon et al. (6). In this study, and other local studies (20) treatment interruptions were more common among migrants and vulnerable populations because of change in place of living, deportation out of the country or disappearance in illegality for migrants not granted refugee status, and because of a high rate of non-adherence despite good access to health care in Switzerland. Adherence is one of the major determinants of treatment success (5). Among the measures considered for improving the adherence to TB therapy and the cure rate, the DOT is considered as one of the most crucial, since the seminal publication by Weis demonstrating that DOT contributed to the decrease in relapse and acquisition of drug resistance (21). Further studies supported the role of DOT as a method for improving the success rate of TB treatment (22). Recently, several other studies and analysis have questioned this dogma and demonstrated that DOT may not be the only element of success in TB treatment, but that the whole organization of patient care is contributing to the success (23, 24). The experience in our institution seems to confirm this, as the improvement in the cure rate resulted not only from the introduction of DOT in Lausanne in the nineties but also from a change in the management, with better training of specialized nurses, improvements in communication by hiring translators, re-organization of the appointment schedules, and above all increasing the attention to the social problems faced by the migrants and vulnerable populations (19). Indeed, since the nineties, a reinforcement of the existing personnel at the TB clinic was assured in VD County with extended opening hours as recommended in treatment guidelines (14, 25) and the social aspects were better considered with the inclusion of a social worker in the staff. Since most of the treatment interruptions in the late eighties occurred among AS followed outside the TB clinic by general practitioners lacking the necessary structure to take care of difficult social situations, in later years, we tried to follow this particularly vulnerable population at the DAT. We found that 75.2% of the AS were followed at the DAT and a DOT strategy was applied in 95.5% of them. Among the entire study population DOT was applied in 62.4%. As other programs showed before, we found that regulatory interventions (search for missing patient by police order) were rarely needed and were only applied in case of disappearance of infectious patients (26). Furthermore, thanks to an agreement between the SFOPH and the State Secretariat for Migration, migrants with TB, even those who are not granted asylum status, are no longer deported from the country during the treatment against their will, thus avoiding disappearance in illegality and treatment interruptions.
Like other groups we observed diagnostics delay among elderly people. Most of the deaths were among Swiss elderly patients. Atypical forms of Tb presentation among older patients and lack of suspicion of TB by doctors in elderly patients are well known (27). Diagnostic TB delays has been confirmed by a recent study conducted in Switzerland (28). In our study 2 very old Swiss patients (mean age 85) living in nursing homes were only diagnosed after death (autopsy). This finding underlines, as described by others, a real underappreciated problem with undiagnosed TB cases among older people with potential transmission in the community and particularly to health care workers (29).
Relapses were rare in our study group with only 2 patients in the year following the end of treatment.
This retrospective study has limitations, as we could not analyze prospectively if the improvements of outcomes and adherence were due to the health care and social interventions deployed among the most vulnerable populations. Another limitation of this study is that we described an observational cohort from a single center in comparison with a historical cohort only but without a control group, and that the role of each different components that helped improving the tuberculosis care (DOT vs. social support) could not be assessed properly in a prospective way. The strengths are the relatively high number of patients included in the analysis, the quality control of the daily work in the center and the good treatment outcomes obtained.
In summary, this study shows an improvement in treatment outcomes in VD County with a global success rate of 90.1% overpassing the expectations of 85% requested by the WHO. The patient-centered approach of TB care in VD County provides social protection with a high-quality standard of TB care and a scale-up compared to previous published outcomes.
Ethics Statement
Commission cantonale d'Ethique sur la Recherche sur l'ê tre humain. CER-VD Project Number 2017-02300.
Author Contributions
JM-S: design of the study, data collection and analysis, manuscript redaction. EC: data collection, manuscript revision. OO and JZ: data analysis and manuscript revision. KJ, EM, and LN: manuscript revision. All authors listed have made a substantial, direct and intellectual contribution to the work, and approved it for publication.
Conflict of Interest Statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Acknowledgments
We thank particularly the nurses of the Lung Association of VD County, the nurses and social worker of the DAT and the members of the Laboratory of Molecular Diagnostic and Tuberculosis of the Lausanne University Hospital.
References
1. Tuberculosis in Switzerland-Revised Edition. (2019). Available online at: https://www.tbinfo.ch/fileadmin/user_upload/1wissenszentrum/Publikationen/Handbuch_Tuberkulose/Handbuch_TB_FR_29_03_19.pdf
2. Lonnroth K, Migliori GB, Abubakar I, D'Ambrosio L, de Vries G, Diel R, et al. Towards tuberculosis elimination: an action framework for low-incidence countries. Eur Respir J. (2015) 45:928–52. doi: 10.1183/09031936.00214014
3. Uplekar M, Weil D, Lonnroth K, Jaramillo E, Lienhardt C, Dias HM, et al. WHO's new end TB strategy. Lancet. (2015) 385:1799–801. doi: 10.1016/S0140-6736(15)60570-0
4. Lonnroth K, Mor Z, Erkens C, Bruchfeld J, Nathavitharana RR, van der Werf MJ, Lange C, Tuberculosis in migrants in low-incidence countries: epidemiology and intervention entry points. Int J Tuberc Lung Dis. (2017) 21:624–37. doi: 10.5588/ijtld.16.0845
5. Sumartojo E, When tuberculosis treatment fails. A social behavioral account of patient adherence. Am Rev Respir Dis. (1993) 147:1311–20. doi: 10.1164/ajrccm/147.5.1311
6. Zellweger JP, Coulon P, Outcome of patients treated for tuberculosis in Vaud County Switzerland. Int J Tuberc Lung Dis. (1998) 2:372–7.
7. Helbling P, Medinger C, Altpeter E, Raeber PA, Beeli D, Zellweger JP. Outcome of treatment of pulmonary tuberculosis in Switzerland in 1996. Swiss Med Wkly. (2002) 132:517–22. Available online at: https://smw.ch_2002_10045
8. World Health Organization. Definitions and Reporting Framework for Tuberculosis-−2013 Revision, Geneva (2013).
9. International Union Against Tuberculosis and Lung Disease. International Union Against Tuberculosis and Lung Disease. Technical guide: Sputum examination for tuberculosis by direct microscopy in low-income countries (2000). Available online at: https://www.medbox.org/laboratory-technologies/technical-guide-sputum-examination-for-tuberculosis-by-direct-microscopy-in-low-income-countries/preview?q=
10. Greub G, Sahli R, Brouillet R, Jaton K. Ten years of R&D and full automation in molecular diagnosis. Future Microbiol. (2016) 11:403–25. doi: 10.2217/fmb.15.152
11. Opota O, Senn L, Prod'hom G, Mazza-Stalder J, Tissot F, Greub G, et al. Added value of molecular assay Xpert MTB/RIF compared to sputum smear microscopy to assess the risk of tuberculosis transmission in a low-prevalence country. Clin Microbiol Infect. (2016) 22:613–9. doi: 10.1016/j.cmi.2016.04.010
12. Volmink J, Matchaba P, Garner P. Directly observed therapy and treatment adherence. Lancet. (2000) 355:1345–50. doi: 10.1016/S0140-6736(00)02124-3
13. Munro SA, Lewin SA, Smith HJ, Engel ME, Fretheim A, Volmink J. Patient adherence to tuberculosis treatment: a systematic review of qualitative research. PLoS Med. (2007) 4: e238. doi: 10.1371/journal.pmed.0040238
14. Migliori GB, Zellweger JP, Abubakar I, Ibraim E, Caminero JA, De Vries G, et al. European union standards for tuberculosis care. Eur Respir J. (2012) 39:807–19. doi: 10.1183/09031936.00203811
15. Nahid P, Dorman SE, Alipanah N, Barry PM, Brozek JL, Cattamanchi A, et al. Official American thoracic society/centers for disease control and prevention/infectious diseases society of America clinical practice guidelines: treatment of drug-susceptible tuberculosis. Clin Infect Dis. (2016) 63:e147–95. doi: 10.1093/cid/ciw376
16. Lutge EE, Wiysonge CS, Knight SE, Volmink J. Material incentives and enablers in the management of tuberculosis. Cochrane Database Syst Rev. (2012) 1:CD007952. doi: 10.1002/14651858.CD007952.pub2
17. Morozova O, Dvoryak S, Altice FL. Methadone treatment improves tuberculosis treatment among hospitalized opioid dependent patients in Ukraine. Int J Drug Policy. (2013) 24:e91–8. doi: 10.1016/j.drugpo.2013.09.001
18. Guglielmi S, Barben J, Horn L, Schoch OD. Administrative monitoring of tuberculosis treatment in Switzerland. Int J Tuberc Lung Dis. (2006) 10:1236–40.
19. Deruaz J, Zellweger JP. Directly observed therapy for tuberculosis in a low prevalence region: first experience at the Tuberculosis Dispensary in Lausanne. Swiss Med Wkly. (2004) 134:552–8. doi: 10.4414/smw.2004.10643
20. Rose N, Shang H, Pfyffer GE, Brandli O. [Tuberculosis therapy in canton Zurich 1991–1993: what are the causes for recurrence and therapy failure?]. Schweiz Med Wochenschr. (1996) 126:2059–67.
21. Weis SE, Slocum PC, Blais FX, King B, Nunn M, Matney B, et al. The effect of directly observed therapy on the rates of drug resistance and relapse in tuberculosis. N Engl J Med. (1994) 330:1179–84. doi: 10.1056/NEJM199404283301702
22. Moonan PK, Quitugua TN, Pogoda JM, Woo G, Drewyer G, Sahbazian B, et al. Does directly observed therapy (DOT) reduce drug resistant tuberculosis? BMC Public Health. (2011) 11:19. doi: 10.1186/1471-2458-11-19
23. Volmink J, Garner P. Directly observed therapy for treating tuberculosis. Cochr Database Systemat Rev. (2007) 4:CD003343. doi: 10.1002/14651858.CD003343.pub3
24. Pasipanodya JG, Gumbo T. A meta-analysis of self-administered vs. directly observed therapy effect on microbiologic failure, relapse, and acquired drug resistance in tuberculosis patients. Clin Infect Dis. (2013) 57:21–31. doi: 10.1093/cid/cit167
25. Garner P, Smith H, Munro S, Volmink J. Promoting adherence to tuberculosis treatment. Bull World Health Organ. (2007) 85:404–6. doi: 10.2471/BLT.06.035568
26. Gasner MR, Maw KL, Feldman GE, Fujiwara PI, Frieden TR. The use of legal action in New York City to ensure treatment of tuberculosis. N Engl J Med. (1999) 340:359–66. doi: 10.1056/NEJM199902043400506
27. Rajagopalan S. Tuberculosis and aging: a global health problem. Clin Infect Dis. (2001) 33:1034–9. doi: 10.1086/322671
28. Christian Auer SK, Zuske M, Schindler C, Wyss K, Blum J, Bosch-Capblanch X, et al. Health-seeking behaviour and treatment delay in patients with pulmonary tuberculosis in Switzerland: some slip through the net. Swiss Med Wkly. (2018) 148:w14659. doi: 10.4414/smw.2018.14659
Keywords: tuberculosis outcomes, treatment adherence, tuberculosis in Switzerland, directly-observed therapy, tuberculosis social approach
Citation: Mazza-Stalder J, Chevallier E, Opota O, Carreira A, Jaton K, Masserey E, Zellweger JP and Nicod LP (2019) Improvement in Tuberculosis Outcomes With a Combined Medical and Social Approach. Front. Med. 6:135. doi: 10.3389/fmed.2019.00135
Received: 06 December 2018; Accepted: 30 May 2019;
Published: 21 June 2019.
Edited by:
Konrad E. Bloch, University Hospital Zürich, SwitzerlandReviewed by:
Otto Dagobert Schoch, Kantonsspital St. Gallen, SwitzerlandCarolin Steinack, University Hospital Zürich, Switzerland
Copyright © 2019 Mazza-Stalder, Chevallier, Opota, Carreira, Jaton, Masserey, Zellweger and Nicod. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Jesica Mazza-Stalder, amVzaWNhLm1henphLXN0YWxkZXJAY2h1di5jaA==