 Coralie Zumelzu1
Coralie Zumelzu1 Marina Alexandre1
Marina Alexandre1 Christelle Le Roux1Patricia Weber1Alexis Guyot1Annie Levy2Françoise Aucouturier3Sabine Mignot-Grootenboer4Frédéric Caux1Eve Maubec1
Christelle Le Roux1Patricia Weber1Alexis Guyot1Annie Levy2Françoise Aucouturier3Sabine Mignot-Grootenboer4Frédéric Caux1Eve Maubec1 Catherine Prost-Squarcioni1,2,5*
Catherine Prost-Squarcioni1,2,5*- 1Department of Dermatology and Referral Center for Auto-Immune Bullous Diseases MALIBUL, Avicenne Hospital, AP-HP, University Paris 13, Bobigny, France
- 2Department of Pathology, Avicenne Hospital, AP-HP, University Paris 13, Bobigny, France
- 3Department of Immunology and Referral Center for Auto-Immune Bullous Diseases MALIBUL, Saint-Louis Hospital, AP-HP, Paris, France
- 4Department of Immunology and Referral Center for Auto-Immune Bullous Diseases MALIBUL, Bichat Hospital, AP-HP, Paris, France
- 5Department of Histology, UFR Léonard de Vinci, University Paris 13, Bobigny, France
An 83-year-old patient developed erosions and a blister of the gingival mucous membrane, 6 months after discontinuation of the anti-programmed death-1 (anti PD-1) pembrolizumab therapy administered for 10 months for a metastatic melanoma. A diagnosis of mild mucous membrane pemphigoid (MMP) was made. Complete remission of MMP was rapidly obtained with minimal therapy (doxycycline). MMP remained in complete remission after a 3-month follow-up since discontinuation of the doxycycline therapy and no evidence of relapse of the melanoma was observed after a 14-month follow-up since discontinuation of the pembrolizumab therapy. The widespread use of anti PD-1 and anti-programmed death-ligand-1 (PD-L1) in several malignancies reveals new adverse events. MMP describes a group of chronic, inflammatory, mucous membrane-predominant, subepithelial auto-immune blistering diseases. It is clinically distinct from bullous pemphigoid another autoimmune blistering disease but shares some immunological similarities with it. Twenty-nine cases of bullous pemphigoid associated with anti PD-1/PD-L1 have been reported in the literature and one of MMP. Here, we described the case of a MMP developed after pembrolizumab and discussed the accountability of anti PD-1/PD-L1 in our case and the previous reported bullous pemphigoid and MMP cases using the Begaud system scoring.
Background
Immune checkpoint inhibitors against programmed death-1 (anti PD-1) and programmed death-ligand 1 (anti-PD-L1) agents have revolutionized the treatment of metastatic melanoma and have shown encouraging promise in advanced solid tumors and hematological malignancies. However, these agents are associated with immune-related adverse events (IrAEs) that affect mainly the skin, hormone glands, liver and gastrointestinal tracts.
Indeed, up to 20% of treated patients may develop dermatological IrAEs. They are predominantly non-specific rashes and pruritus (1). Toxicities on buccal mucous membrane (MM) have also been described, including xerostomia, lichenoid reactions, and dysgeusia (2). Since 2015, an association between a treatment with anti PD-1/PD-L1 and bullous pemphigoid (BP) has been reported in 29 cases. One mucous membrane pemphigoid (MMP) case, an autoimmune bullous disease (AIBD) similar to BP, has also been described after pembrolizumab therapy.
Here, we report a second case of MMP that occurred 16 months after initiation of pembrolizumab therapy for a metastatic melanoma, discuss the association between MMP and melanoma, and review the literature on BP and MMP associated with anti PD-1/PD-L1.
Case Presentation
In 2014, an 83-year-old woman with no history of known autoimmune disease was diagnosed as having a right leg superficial spreading melanoma, initially T2b N0 M0. Eight months later, she developed iterative local and in transit cutaneous metastases on the same leg and she underwent four times surgical excision.
In 2016, at the fourth recurrence, surgery was not chosen. Baseline full-body computed tomography revealed no other metastasis (T2 N0 M1a). Mutation tested on a tumor sample excluded the presence of any BRAF mutation. Administration of pembrolizumab therapy was started at 2 mg/kg every 3 weeks, resulting in complete remission (CR) within 3 months (cycle 4). In March 2017, after 14 cycles, she remained in CR, and the pembrolizumab therapy was stopped at her request.
In October 2017, 6 months after pembrolizumab discontinuation, she complained of oral pain and was referred to our hospital. Clinical examination revealed gingivitis with one tense blister, a large pseudomembrane-covered erosion with a tweezers sign, an atrophy and pseudo lichenoid lesions. Other MM and skin were not involved. Gingival biopsy showed a subepithelial cleavage with the overlying intact epithelium (Figure 1A). A moderate perivascular infiltration consisting of lymphocytes and histiocytes was observed, with no lichenoid infiltrates. Direct immunofluorescence (DIF) microscopy revealed linear IgG (++) and C3 (++) immune deposits along the basement membrane zone (BMZ) (Figure 1B). Standard indirect immunofluorescence (IIF) microscopy on rat esophagus failed to detect circulating anti-BMZ antibodies. A diagnosis of mild MMP was made. Further immunological investigations demonstrated that the immune deposits identified using direct immunoelectron microscopy (IEM) were strictly localized in the lamina densa (Figure 2), a site consistent with autoantibodies against the laminin 332 or the C-terminal extremity of BP180 antigen (BP180). IIF on salt-split skin, immunoblot using amniotic extracts, and enzyme-linked immunosorbent assays (ELISAs) with BP180-NC16A epitope and BP230 antigen (BP230) had negative results.
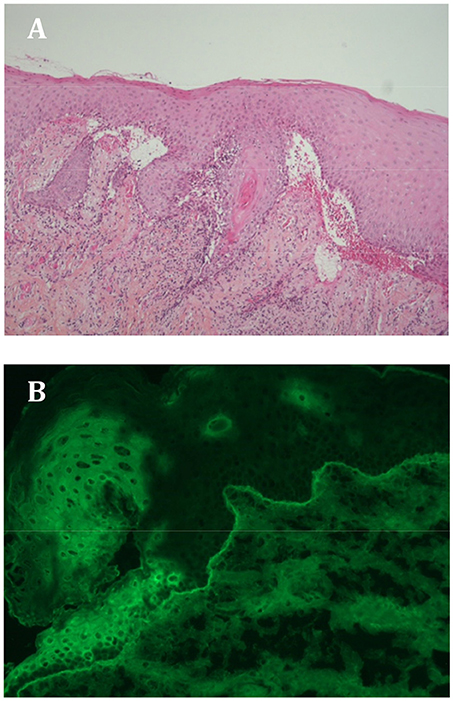
Figure 1. (A) Histological examination of a gingival biopsy showing subepithelial cleavage with overlying intact epithelium. A moderate perivascular infiltration can be observed consisting of lymphocytes and histiocytes, and no lichenoid infiltrate. (B) Direct immunofluorescence microscopic image showing linear IgG (++) and C3 (++) immune deposits along the basement membrane zone on the gingival biopsy.
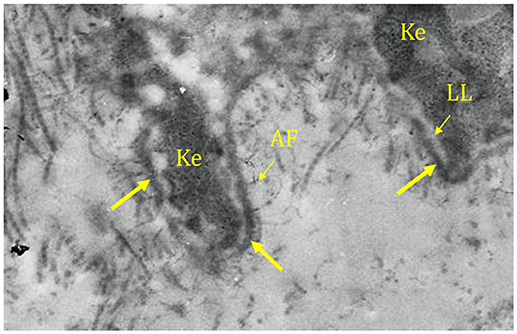
Figure 2. Direct immunoelectron microscopy showing immune deposits (arrow) strictly localized in the lamina densa. Ke, keratinocyte; LL, lamina lucida; AF, anchoring fibril.
Doxycycline therapy (100 mg/day) and mouth washes with corticosteroid (betamethasone 2 mg) three times daily were initiated, which led to the control of the MMP within 2 weeks and CR under this minimal therapy in 6 weeks. After 3 months of treatment with doxycycline therapy, the patient decided on her own to discontinue it, and no MMP relapse had occurred 3 months later. No clinical or radiological evidence of relapse of the melanoma was observed on computed tomography imaging after a 14-month follow-up since discontinuation of the pembrolizumab therapy.
Discussion
Our case raises the question of an association between MMP and melanoma, or between MMP/BP and pembrolizumab administration.
MMP encompasses a group of AIBDs clinically defined by the predominance of MM lesions over skin lesions (3, 4), and healing of its lesions leads to characteristic cicatricial scarring. The buccal involvement is the most frequent, followed in order of decreasing frequency by ocular, nasal, nasopharyngeal, anogenital, skin, laryngeal, and oesophageal involvements. The ocular, laryngeal, and oesophageal involvements can cause severe impairment or even death.
Our patient had a typical MMP, except the age at MMP onset, in a mild form because of the purely buccal involvement. Thus she was considered as a “low-risk patient” with few tendencies of scarring and required minimal therapy with doxycycline and topical steroids (3). Her MMP was controlled in 2 weeks, in CR on minimal therapy in 6 weeks, and in CR off treatment in 3 months. She developed mild cicatricial lesions of her gingival MM and did not relapse during follow-up. Rapid clinical improvement after only a short course of treatment is unusual in MMP.
MMP results from the activity of autoantibodies directed against BMZ antigens. The main autoantibody target is BP180, with the sera of most MMP patients reacting with its C-terminal domain (BP180-C term), combined or not with reactivity against the BP180-NC16A epitope and BP230 (5, 6). Other target antigens associated with a clinical MMP phenotype have been characterized molecularly, including the following: laminin 332, both α6β4-integrin subunits, and type VII collagen (7), respectively defining laminin 332-MMP, α6β4-integrin MMP, and MM epidermolysis bullosa acquisita. Autoreactive T lymphocytes are thought to also play a key role in the pathogenesis of MMP, particularly in the fibrosing process (8–15).
Our patient had a linear deposition of IgG/C3 along the epithelial BMZ on DIF microscopy and on the lamina densa on direct IEM, a location consistent with targeting of the C-terminal extremity of BP180 or laminin 332 by autoantibodies (16, 17). No circulating antibodies against BMZ antigens were detected by serological studies, notably BP180-NC16A ELISA, as in 49% of MMP in a recent series (18).
An association between laminin 332-MMP and malignancy was first reported in 1998 but is currently controversial. On one hand, 21 cases of laminin 332-MMP have been reported in association with cancer, including 15 reviewed by Sadler in 2007 (19) and six case reports after 2007 (20–25). An increased risk of solid cancers as compared with the general population was reported by two authors (26, 27), higher in the first year following the laminin 332-MMP diagnosis. On the other hand, no significant correlation was found between laminin 332 reactivity and the proportion of patients with an associated internal cancer in three recent serological studies of MMP (28–30).
Anyway, no association between laminin 332-MMP and melanoma has been reported (31).
In our patient, who had a possible laminin 332-MMP, a link between MMP and melanoma seems unlikely, as the first incidence occurred 3 years after the second and the latter was in CR.
We examined the intrinsic accountability of pembrolizumab therapy on MMP induction in our patient with metastatic melanoma because of its extrinsic accountability based on the following reports: (i) MMP and BP have immunological similarities (7); (ii) intrinsic accountability of anti PD-1/PD-L1 treatments on BP induction: 27 BP have been reported as case reports or short series (32–49) and two BPs listed as adverse drug reaction in two large trials with anti PD-1 (50, 51); (iii) recently, one pembrolizumab-associated MMP case report (52), and (iv) some of the anti PD-1/PD-L1-associated BPs had atypical clinical phenotypes (33–35, 42, 47).
Although the clinical characteristics of MMP differ from those of BP typified by the absence of MM lesions, absence of predominant head-and-neck involvement, absence of scars, and older age at onset (>70 years) (53), MMP and BP share physiopathological features; BP result from the activity of autoantibodies directed against BP230 and BP180, such as most MMPs. However, the sera of most patients with BP react with the BP180-NC16A epitope, contrary to those of patients with MMP.
The melanoma treatment has been revolutionized by innovative immunomodulation drugs that break tolerance. The main treatment targets for melanoma are cytotoxic T-lymphocyte antigen-4 and PD-1. Ipilimumab, a monoclonal antibody against cytotoxic T-lymphocyte antigen-4, was the first drug to demonstrate a benefit in overall survival in a randomized controlled phase 3 study of patients with advanced melanoma (54) and to be approved by the Food and Drug Administration (FDA) and European Medicines Agency (EMA). The anti-PD-1s and anti-PD-L1s are remarkably more effective in terms of response and overall survival rates than ipilimumab. The response rate with anti-PD-1 reaches 40% in melanoma, and the 5-year overall survival rate for naive patients is close to 40% (55). Moreover, anti-PD-1s are less toxic in terms of IrAEs. In 2014, the FDA approved the anti-PD-1 antibodies pembrolizumab and nivolumab for advanced melanoma and, in 2015, the combination of ipilimumab and nivolumab.
PD-1 is a negative co-stimulatory receptor, which downregulates excessive immune responses by binding to its ligands, PD-L1 and PD-L2. This receptor is expressed mainly on activated T cells. In tumor tissue, binding of PD-1 inhibits effector T-cell function, which leads to exhausted T cells and suppression of the antitumor immune response (56). Pembrolizumab and nivolumab on one hand and atezolizumab and durvalumab on the other hand are selective humanized monoclonal antibodies that bind respectively to PD-1 and PD-L1 and thus block the interaction between PD-1 and its ligands, which leads to stimulatory effects on T cells.
B cells also express PD-1, and inhibition of PD-1 expression can directly activate B cells in a T-cell-independent manner (57). Lastly, it appears that anti PD-1 reduce regulatory T-cell activity (58), resulting in decreased tolerance and development of autoimmunity. All these mechanisms can be involved in the induction of MMP as soon as B and T cells played a central role in the MMP pathogenesis.
The potential drug induction of AIBD has been known for decades (18, 59–66). Recently, between 2015 and 2018, 18 case reports or small series described 27 patients who developed BP while receiving anti PD-1/PD-L1 therapy, including three with negative DIF (35, 37) or without DIF confirmation (47) but with typical clinical presentations (Tables 1, 2). Fourteen patients received anti PD-1 nivolumab therapy (patients 2, 4, 7, 9, 10, 13, 15, 18, 20, 22, 23, and 25–27) (33, 35, 38, 42, 44, 46, 47, 49), 11 received anti PD-1 pembrolizumab therapy (patients 1, 5, 6, 8, 11, 12, 14,16, 19, 21, and 24) (32, 34–37, 39, 40, 43, 45, 48), one received anti-PD-L1 durvalumab therapy (patient 3) (33), and one received anti-PD-L1 atezolizumab therapy (patient 17) (41). Six of the 27 patients received ipilimumab therapy before anti PD-1, one received an association of ipilimumab and nivolumab therapy, and one received ipilimumab therapy after treatment with nivolumab. Two additional BP cases within a large series were simply mentioned, without any clinical description (50, 51). Recently, one MMP case treated with pembrolizumab therapy for a metastatic Merkel cell carcinoma has also been reported (53). Notably, the outcomes of the patients with melanoma were better [only 5 (33%) out of 15 cases in which the information were available, had a progressive disease] than reported in general anti-PD-1 treatment of melanoma (55). Other studies reported that objective response rate was significantly higher in patients with melanoma who experienced nivolumab-related adverse events (67).
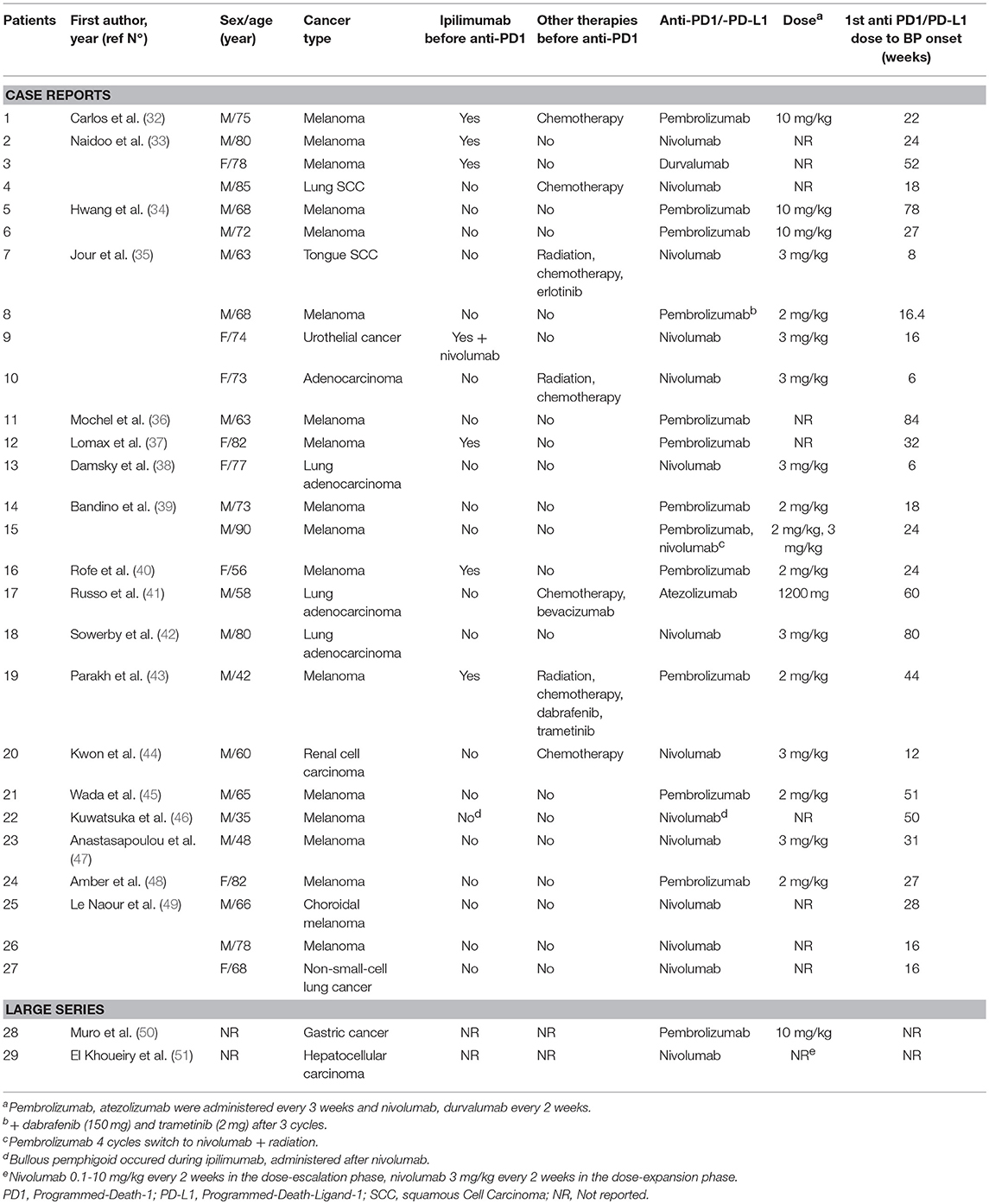
Table 1. Case reports of anti-PD1/PD-L1-treated bullous pemphigoid patients.
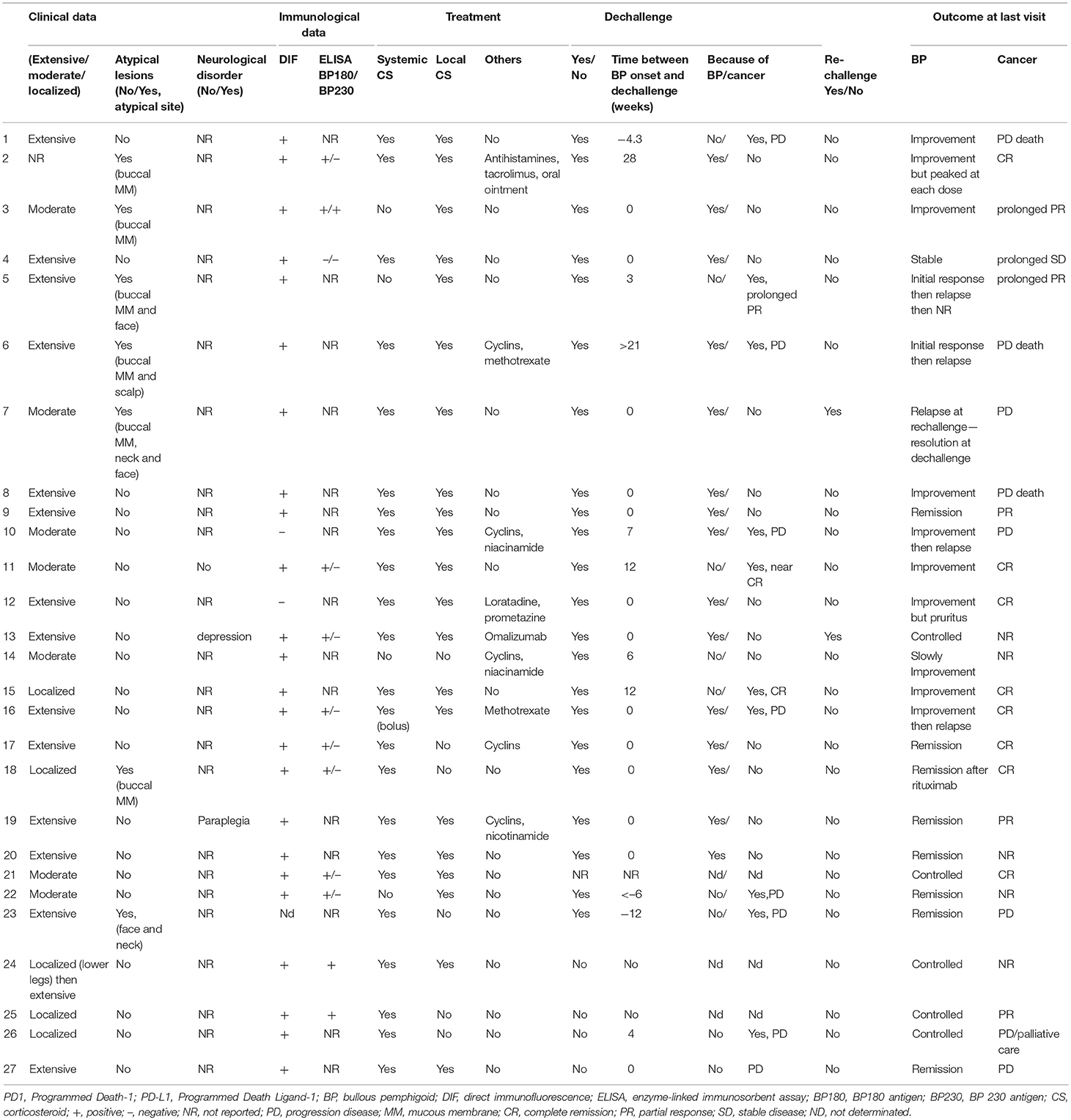
Table 2. Clinical, immunological, and evolutive data in 27 of the 29 anti-PD1/PD-L1-treated BP patients reported in the literature.
The overall characteristics of these patients with anti PD-1/PD-L1-associated BPs were as follows: eight women and 19 men (female-to-male sex ratio, 0.4), median age of 68 years (35–90 years) at the time of BP diagnosis, and a median interval of 24 (6–84) weeks between starting anti PD-1/PD-L1 therapy (challenge) and BP onset. This time was significantly shorter (median, 16 weeks; range, 6–80 weeks) with nivolumab than with pembrolizumab (median, 27 weeks; range, 16–84 weeks) (Wilcoxon rank sum test with continuity correction: p = 0.023).
Pruritus was a prominent feature of most cases (68). Administration of anti PD-1/PD-L1 agents was discontinued (dechallenge) in 21 of the 27 patients (patients 1–14, 16–20, 22, 23, and 27) because of the evolution of BP and/or cancer and continued in five patients (no dechallenge, patients 1, 15, and 24–26). This information is unknown in one patient (patient 21). BP treatment with systemic steroids was required in all but four patients (patients 3, 5, 14, and 22). AntiPD-1/PD-L1 was reintroduced in two patients (rechallenge; patients 7 and 13). The reasons of the dechallenge, and the outcome after dechallenge or rechallenge are detailed in Table 2.
The comparison with the “usual” BPs (7, 69) highlights particularities in these anti PD-1/PD-L1-associated BPs as follows: a predominance of males (female-to-male sex ratio, 0.4 vs. 1.5), younger age [mean, 69 years; median, 68 years (range, 35–90 years) vs. mean, 83 years], no evidence of neurological disorders, more extensive diseases (52 vs. 41%), and no circulating autoantibodies against BP230 except in one patient (8 vs. 60–70%), while 91% of the tested sera had circulating autoantibodies against BP180-NC16A (vs. 80–90%). Moreover, seven cases had atypical clinical phenotypes, as head and neck involvement or mucosal lesions (33–35, 42, 47), raising doubts about the diagnosis of BP (53).
The patient with pembrolizumab-associated MMP reported by Haug et al. was a 62-year-old man who developed a pure buccal MMP after 13 weeks of pembrolizumab therapy. He had circulating autoantibodies targeting the C-terminal extremity of BP180. Pembrolizumab was discontinued at the time of MMP onset, and he was successfully treated with doxycycline and topical steroid, as in our case.
In our patient, MMP developed after 14 cycles and 24 weeks of pembrolizumab discontinuation, that is, 66 weeks after starting the treatment. Overall, IrAE induced by anti PD-1/PD-L1 agents usually appeared between 1 week and several months after starting immunotherapy (2). Among the 27 cases of anti PD-1/PD-L1-associated BPs, four had a long delay (>60 weeks) between starting anti PD-1/PD-L1 therapy and onset of BP (patients 5, 11, 17, and 18) (34, 36, 41, 42). Similarly to our patient, three patients developed a BP 4, 12, and 12 weeks after discontinuation of the anti PD-1 therapy (patients 1, 22, and 23, respectively) (32, 46, 47). This could be explained by the durable activity of anti PD-1/PD-L1 on immunity (70, 71).
Lastly, we assessed the intrinsic accountability score of anti PD-1/PD-L1 in AIBD induction for our patient with MMP, and a posteriori for the 27 BPs and MMP cases that have been reported using the Begaud scoring system (terms in bold type), updated in 2011 (72). The present challenge was the treatment of a malignancy by using an anti PD-1/PD-L1. Patients with a malignancy who started treatment with anti PD-1/PD-L1 before MMP/BP onset may have a suggestive or compatible challenge. The dechallenge was the discontinuation of the treatment. Outcome after dechallenge or no dechallenge may be suggestive (if BP is controlled with dechallenge or worsened without dechallenge), conversely non-suggestive (if BP worsened after dechallenge or controlled unless without dechallenge), and inconclusive (without details on BP evolution or continued treatment).
The rechallenge was the reintroduction of the treatment. It may be positive (R+) or negative (R–) or not done (R0). The chronological scoring (combining status of challenge, dechallenge, and rechallenge) may be C1, doubtful; C2, plausible; and C3, likely. The symptomatological scoring may be S1, doubtful; S2, plausible; and S3, likely. Lastly, the intrinsic accountability scoring [combining chronological (C) and symptomatological (S) scores] may be I1 (C1S1), I2 (C1S2 or C2S1), I3 (C2S2), I4 (C1S3 or C3S1), I5 (C2S3 or C3S2), or I6 (C3S3) (see detailed results in Supplementary Data, Table S1).
The Begaud system scoring indicates that the possibility of anti PD-1/PD-L1 as a BP triggering factor is mostly low: only 10 (four with pembrolizumab, five with nivolumab, and one with durvalumab) of the 27 patients with BP were given high accountability scores [I5 for three patients (patients 2, 6, and 7), I4 for five (patients 8, 9, 14, 20, and 27), I3 for two (patients 3 and 5)], while 17 (seven with pembrolizumab, nine with nivolumab, and one with atezolizumab) had low accountability [I2 for six (patients 10, 12, 17, 18, 19, and 23) and I1 for 11 (patients 1, 4, 11, 13, 15, 16, 21, 22, and 24–26)]. One patient with BP had a positive rechallenge, and another had a negative rechallenge.
The Begaud system scoring indicates that the intrinsic accountability score was I4 for the MMP case that was reported but I1 for our patient with MMP.
In all the MMP/BP patients, the low score was essentially due to the long time between anti PD-1 introduction and AIBD onset (compatible challenge) and/or a non-suggestive dechallenge. Indeed, it could be the consequence of long delay of action of anti PD-1/PD-L1. A non-suggestive dechallenge may not be an argument against the accountability of a long-acting drug, and at the end, the Begaud scoring system may not be suitable for assessing the accountability of drugs with prolonged therapeutic effect.
In our patient, the eventuality of a rechallenge did not occur because the melanoma and MMP remained in CR. As an anti PD-1-induced MMP is possible, a rechallenge would theoretically expose her to a risk of MMP relapse in a potentially more serious form. Indeed, MMP can involve ocular, nasopharyngeal, laryngeal, esophageal, genital, or anal MM, sites that have a high likelihood of scarring, which is associated with loss of function. On the other hand and contrary to literatures on adverse drug reactions, a negative rechallenge with anti PD-1 has already been reported (38, 73).
In conclusion, we report the case of a patient who developed a mild MMP, possibly induced by anti PD-1 rather than by melanoma. We cannot also exclude that the MMP could be triggered by aging, malignancy, and pembrolizumab acting in concert or developed quite independently. MMP was rapidly controlled by a minimal treatment, raising the question of reintroduction of anti PD-1 if the melanoma relapses. With the increasing use of immunotherapies for various malignancies, clinicians should be alert for this new anti PD-1-induced IrAE, which is related to BP but potentially more severe. Long-term clinical follow-up is warranted owing to delayed adverse events, even after discontinuation of anti PD-1 inhibitors. Lastly the Begaud system scoring applied to our patient and previous reported cases with anti-PD-1/PD-L1 related BP/MMP indicates a low intrinsic accountability score in most of the patients suggesting it may not be suitable for assessing the accountability of drugs with prolonged therapeutic effect. Development of another specific assessment might be necessary.
Ethics Statement
A written consent has been obtained from the patient.
Author Contributions
CZ and CP-S conceived and designed the study. CZ, MA, CL, PW, AG, and EM collected clinical data. AL and CP-S conducted the histological studies and FA and SM-G the immunological ones. CZ wrote the first draft of the manuscript. CP-S rewrote sections of the manuscript. EM and FC corrected the final version. All authors contributed to manuscript revision, and read and approved the submitted version.
Conflict of Interest Statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Acknowledgments
We thank physicians who referred the patient to our department of oncodermatology and Referral Center for autoimmune bullous diseases and the Center's physicians who assured multidisciplinary patient management (Drs. Francis Pascal, Isaac Soued); Mrs. Nicole Lièvre and Mr. Michel Heller for their technical assistance.
Supplementary Material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fmed.2018.00268/full#supplementary-material
Abbreviations
AIBD, autoimmune bullous disease; anti PD-1, anti-Programmed-Death-1; anti-PD-L1, anti-Programmed-Death-ligand-1; BMZ, basement membrane zone; BP, bullous pemphigoid; BP180, BP180 antigen; BP230, BP230 antigen; CR, complete remission; DIF, direct immunofluorescence; ELISA, enzyme-linked immunosorbent assay; FDA, Food and Drug Administration; IEM, immunoelectron microscopy; IIF, indirect immunofluorescence; IrAEs, immune-related adverse events; MM, mucous membrane(s); MMP, mucous membrane pemphigoid.
References
1. Curry JL, Tetzlaff MT, Nagarajan P, Drucker C, Diab A, Hymes SR, et al. Diverse types of dermatologic toxicities from immune checkpoint blockade therapy. J Cutan Pathol. (2017) 44:158–76. doi: 10.1111/cup.12858
2. Sibaud V. Dermatologic reactions to immune checkpoint inhibitors : skin toxicities and immunotherapy. Am J Clin Dermatol. (2018) 19:345–61. doi: 10.1007/s40257-017-0336-3
3. Chan LS, Ahmed AR, Anhalt GJ, Bernauer W, Cooper KD, Elder MJ, et al. The first international consensus on Mucous membrane pemphigoid: definition, diagnostic criteria, pathogenic factors, medical treatment, and prognostic indicators. Arch Dermatol. (2002) 138:370–9. doi: 10.1001/archderm.138.3.370
4. Murrell DF, Marinovic B, Caux F, Prost C, Ahmed R, Wozniak K, et al. Definitions and outcome measures for Mucous membrane pemphigoid: recommendations of an international panel of experts. J Am Acad Dermatol. (2015) 72:168–74. doi: 10.1016/j.jaad.2014.08.024
5. Murakami H, Nishioka S, Setterfield J, Bhogal BS, Black MM, Zillikens D, et al. Analysis of antigens targeted by circulating IgG and IgA autoantibodies in 50 patients with cicatricial pemphigoid. J Dermatol Sci. (1998) 17:39–44. doi: 10.1016/S0923-1811(97)00067-4
6. Balding SD, Prost C, Diaz LA, Bernard P, Bedane C, Aberdam D, et al. Cicatricial pemphigoid autoantibodies react with multiple sites on the BP180 extracellular domain. J Invest Dermatol. (1996) 106:141–6. doi: 10.1111/1523-1747.ep12329728
7. Schmidt E, Zillikens D. Pemphigoid diseases. Lancet (2013) 381:320–32. doi: 10.1016/S0140-6736(12)61140-4
8. Sacks EH, Jakobiec FA, Wieczorek R, Donnenfeld E, Perry H, Knowles DM Jr. Immunophenotypic analysis of the inflammatory infiltrate in ocular cicatricial pemphigoid. Further evidence for a T cell-mediated disease. Ophthalmology (1989) 96:236–43. doi: 10.1016/S0161-6420(89)32922-8
9. Rice BA, Foster CS. Immunopathology of cicatricial pemphigoid affecting the conjunctiva. Ophthalmology (1990) 97:1476–83. doi: 10.1016/S0161-6420(90)32402-8
10. Bernauer W, Wright P, Dart JK, Leonard JN, Lightman S. The conjunctiva in acute and chronic Mucous membrane pemphigoid. An immunohistochemical analysis. Ophthalmology (1993) 100:339–46. doi: 10.1016/S0161-6420(93)31644-1
11. Lambiase A, Micera A, Mantelli F, Moretti C, Di Zazzo A, Perrella E, et al. T-helper 17 lymphocytes in ocular cicatricial pemphigoid. Mol Vis. (2009) 15:1449–55.
12. Suelves AM, Zhao TZ, Siddique SS, Foster CS. Profile of local interleukin expression in a cohort of ocular cicatricial pemphigoid patients. Invest Ophthalmol Vis Sci. (2012) 53:8112–7. doi: 10.1167/iovs.11-9322
13. Saw VP, Offiah I, Dart RJ, Galatowicz G, Dart JK, Daniels JT, et al. Conjunctival interleukin-13 expression in Mucous membrane pemphigoid and functional effects of interleukin-13 on conjunctival fibroblasts in vitro. Am J Pathol. (2009) 175:2406–15. doi: 10.2353/ajpath.2009.090579
14. Torchia D, Caproni M, Volpi W, Fabbri P. Naturally occurring regulatory T cells in Mucous membrane pemphigoid lesions. Acta Dermatovenerol Alp Pannonica Adriat. (2009) 18:3–6.
15. Black AP, Seneviratne SL, Jones L, King AS, Winsey S, Arsecularatne G, et al. Rapid effector function of circulating NC16A-specific T cells in individuals with Mucous membrane pemphigoid. Br J Dermatol. (2004) 151:1160–4. doi: 10.1111/j.1365-2133.2004.06219.x
16. Bédane C, McMillan JR, Balding SD, Bernard P, Prost C, Bonnetblanc JM, et al. Bullous pemphigoid and cicatricial pemphigoid autoantibodies react with ultrastructurally separable epitopes on the BP180 ectodomain: evidence that BP180 spans the lamina lucida. J Invest Dermatol. (1997) 108:901–7. doi: 10.1111/1523-1747.ep12292701
17. Prost-Squarcioni C. Part II: Diagnostic tests - Ch 19. Electron microscopy and immunoelectron microscopy. In: Murrell Dedee editor. Blistering Diseases- Clinical Features, Pathogenesis, Treatment. New York, NY: Springer (2015) p. 213–37.
18. Gaudin O, Seta V, Alexandre M, Bohelay G, Aucouturier F, Mignot-Grootenboer S, et al. Gliptin accountability in Mucous membrane pemphigoid induction in 24 Out of 313 patients. Front Immunol. (2018) 9:1030. doi: 10.3389/fimmu.2018.01030
19. Sadler E, Lazarova Z, Sarasombath P, Yancey KB. A widening perspective regarding the relationship between anti-epiligrin cicatricial pemphigoid and cancer. J Dermatol Sci. (2007) 47:1–7. doi: 10.1016/j.jdermsci.2007.02.012
20. Fukushima S, Egawa K, Nishi H, Wakasugi S, Ishii N, Hashimoto T, et al. Two cases of anti-epiligrin cicatricial pemphigoid with and without associated malignancy. Acta Derm Venereol. (2008) 88:484–7. doi: 10.2340/00015555-0506
21. Takahara M, Tsuji G, Ishii N, Dainichi T, Hashimoto T, Kohno K, et al. Mucous membrane pemphigoid with antibodies to the beta(3) subunit of Laminin 332 in a patient with acute myeloblastic leukemia and graft-versus-host disease. Dermatology (2009) 219:361–4. doi: 10.1159/000243807
22. Dainichi T, Hirakawa Y, Ishii N, Ohyama B, Kohda F, Takahara M, et al. Mucous membrane pemphigoid with autoantibodies to all the laminin 332 subunits and fatal outcome resulting from liver cirrhosis and hepatocellular carcinoma. J Am Acad Dermatol. (2011) 64:1199–200. doi: 10.1016/j.jaad.2009.09.013
23. Young AL, Bailey EE, Colaço SM, Engler DE, Grossman ME. Anti-laminin-332 Mucous membrane pemphigoid associated with recurrent metastatic prostate carcinoma: hypothesis for a paraneoplastic phenomenon. Eur J Dermatol. (2011) 21:401–4. doi: 10.1684/ejd.2011.1360
24. Yamada H, Nobeyama Y, Matsuo K, Ishiji T, Takeuchi T, Fukuda S, et al. A case of paraneoplastic pemphigus associated with triple malignancies in combination with antilaminin-332 Mucous membrane pemphigoid. Br J Dermatol. (2012) 166:230–1. doi: 10.1111/j.1365-2133.2011.10520.x
25. Fukuchi O, Suko A, Matsuzaki H, Baba H, Yoshida H, Takeuchi T, et al. Anti-laminin-332 Mucous membrane pemphigoid with autoantibodies to α3, β3 and γ2 subunits of laminin-332 as well as to BP230 and periplakin associated with adenocarcinoma from an unknown primary site. J Dermatol. (2013) 40:61–2. doi: 10.1111/j.1346-8138.2012.01645.x
26. Egan CA, Lazarova Z, Darling TN, Yee C, Coté T, Yancey KB. Anti-epiligrin cicatricial pemphigoid and relative risk for cancer. Lancet (2001) 357:1850–1. doi: 10.1016/S0140-6736(00)04971-0
27. Matsushima S, Horiguchi Y, Honda T, Fujii S, Okano T, Tanabe M, et al. A case of anti-epiligrin cicatricial pemphigoid associated with lung carcinoma and severe laryngeal stenosis: review of Japanese cases and evaluation of risk for internal malignancy. J Dermatol. (2004) 31:10–5. doi: 10.1111/j.1346-8138.2004.tb00497.x
28. Bernard P, Antonicelli F, Bedane C, Joly P, Le Roux-Villet C, Duvert-Lehembre S, et al. Prevalence and clinical significance of anti-laminin 332 autoantibodies detected by a novel enzyme-linked immunosorbent assay in Mucous membrane pemphigoid. JAMA Dermatol. (2013) 149:533–40. doi: 10.1001/jamadermatol.2013.1434
29. Hayakawa T, Furumura M, Fukano H, Li X, Ishii N, Hamada T, et al. Diagnosis of oral Mucous membrane pemphigoid by means of combined serologic testing. Oral Surg Oral Med Oral Pathol Oral Radiol. (2014) 117:483–96. doi: 10.1016/j.oooo.2013.12.402
30. Cozzani E, Di Zenzo G, Calabresi V, Carrozzo M, Burlando M, Longanesi L, et al. Autoantibody profile of a cohort of 78 Italian patients with Mucous membrane pemphigoid: correlation between reactivity profile and clinical involvement. Acta Derm Venereol. (2016) 96:768–73. doi: 10.2340/00015555-2311
31. Kartan S, Shi VY, Clark AK, Chan LS. Paraneoplastic pemphigus and autoimmune blistering diseases associated with neoplasm: characteristics, diagnosis, associated neoplasms, proposed pathogenesis, treatment. Am J Clin Dermatol. (2017) 18:105–26. doi: 10.1007/s40257-016-0235-z
32. Carlos G, Anforth R, Chou S, Clements A, Fernandez-Peñas P. A case of bullous pemphigoid in a patient with metastatic melanoma treated with pembrolizumab. Melanoma Res. (2015) 25:265–8. doi: 10.1097/CMR.0000000000000155
33. Naidoo J, Schindler K, Querfeld C, Busam K, Cunningham J, Page DB, et al. Autoimmune bullous skin disorders with immune checkpoint inhibitors targeting PD-1 and PD-L1. Cancer Immunol Res. (2016) 4:383–9. doi: 10.1158/2326-6066.CIR-15-0123
34. Hwang SJ, Carlos G, Chou S, Wakade D, Carlino MS, Fernandez-Penas P. Bullous pemphigoid, an autoantibody-mediated disease, is a novel immune-related adverse event in patients treated with anti-programmed cell death 1 antibodies. Melanoma Res. (2016) 26:413–6. doi: 10.1097/CMR.0000000000000260
35. Jour G, Glitza IC, Ellis RM, Torres-Cabala CA, Tetzlaff MT, et al. Autoimmune dermatologic toxicities from immune checkpoint blockade with anti-PD-1 antibody therapy: a report on bullous skin eruptions. J Cutan Pathol. (2016) 43:688–96. doi: 10.1111/cup.12717
36. Mochel MC, Ming ME, Imadojemu S, Gangadhar TC, Schuchter LM, Elenitsas R, et al. Cutaneous autoimmune effects in the setting of therapeutic immune checkpoint inhibition for metastatic melanoma. J Cutan Pathol. (2016) 43:787–91. doi: 10.1111/cup.12735
37. Lomax AJ, Ge L, Anand S, McNeil C, Lowe P. Bullous pemphigoid-like reaction in a patient with metastatic melanoma receiving pembrolizumab and previously treated with ipilimumab. Australas J Dermatol. (2016) 57:333–5. doi: 10.1111/ajd.12484
38. Damsky W, Kole L, Tomayko MM. Development of bullous pemphigoid during nivolumab therapy. JAAD Case Rep. (2016) 2:442–4. doi: 10.1016/j.jdcr.2016.05.009
39. Bandino JP, Perry DM, Clarke CE, Marchell RM, Elston DM. Two cases of anti-programmed cell death 1-associated bullous pemphigoid-like disease and eruptive keratoacanthomas featuring combined histopathology. J Eur Acad Dermatol Venereol. (2017) 31:e378–80. doi: 10.1111/jdv.14179
40. Rofe O, Bar-Sela G, Keidar Z, Sezin T, Sadik CD, Bergman R. Severe bullous pemphigoid associated with pembrolizumabtherapy for metastatic melanoma with complete regression. Clin Exp Dermatol. (2017) 42:309–12. doi: 10.1111/ced.13042
41. Russo I, Sacco G, Frega S, Polo V, Pasello G, Alaibac M. Immunotherapy-related skin toxicity: bullous pemphigoid in a lung adenocarcinoma patient treated with the anti-PDL1 antibody atezolizumab. Eur J Dermatol. (2017) 27:205–8. doi: 10.1684/ejd.2016.2959
42. Sowerby L, Dewan AK, Granter S, Gandhi L, LeBoeuf NR. Rituximab treatment of nivolumab-induced bullous pemphigoid. JAMA Dermatol. (2017) 153:603–5. doi: 10.1001/jamadermatol.2017.0091
43. Parakh S, Nguyen R, Opie JM, Andrews MC. Late presentation of generalised bullous pemphigoid-like reaction in a patient treated with pembrolizumab for metastatic melanoma. Australas J Dermatol. (2017) 58:e109–12. doi: 10.1111/ajd.12488
44. Kwon CW, Land AS, Smoller BR, Scott G, Beck LA, Mercurio MG. Bullous pemphigoid associated with nivolumab, a programmed cell death 1 protein inhibitor. J Eur Acad Dermatol Venereol. (2017) 31:e349–50. doi: 10.1111/jdv.14143
45. Wada N, Uchi H, Furue M. Bullous pemphigoid induced by pembrolizumab in a patient with advanced melanoma expressing collagen XVII. J Dermatol. (2017) 44:e240–1. doi: 10.1111/1346-8138.13940
46. Kuwatsuka Y, Iwanaga A, Kuwatsuka S, Okubo Y, Murayama N, Ishii N, et al. Bullous pemphigoid induced by ipilimumab in a patient with metastatic malignant melanoma after unsuccessful treatment with nivolumab. J Dermatol. (2018) 45:e21–2. doi: 10.1111/1346-8138.14043
47. Anastasopoulou A, Papaxoinis G, Diamantopoulos P, Christofidou E, Benopoulou O, Stratigos A. Bullous pemphigoid-like skin lesions and overt eosinophilia in a patient with melanoma treated with nivolumab: case report and review of the literature. J Immunother. (2018) 41:164–7. doi: 10.1097/CJI.0000000000000210
48. Amber KT, Valdebran M, Lu Y, De Feraudy S, Linden KG. Localized pretibial bullous pemphigoid arising in a patient on pembrolizumab for metastatic melanoma. J Dtsch Dermatol Ges. (2018) 16:196–8. doi: 10.1111/ddg.13411
49. Le Naour S, Peuvrel L, Saint-Jean M, Dreno B, Quereux G. Three new cases of bullous pemphigoid during anti-PD-1 antibody therapy. J Eur Acad Dermatol Venereol. (2018) 32:e104–6. doi: 10.1111/jdv.14579
50. Muro K, Chung HC, Shankaran V, Geva R, Catenacci D, Gupta S, et al. Pembrolizumab for patients with PD-L1-positive advanced gastric cancer (KEYNOTE-012): a multicentre, open-label, phase 1b trial. Lancet Oncol. (2016) 17:717–26. doi: 10.1016/S1470-2045(16)00175-3
51. El-Khoueiry AB, Sangro B, Yau T, Crocenzi TS, Kudo M, Hsu C, et al. Nivolumab in patients with advanced hepatocellular carcinoma (CheckMate 040): an open-label, non-comparative, phase 1/2 dose escalation and expansion trial. Lancet (2017) 389:2492–502. doi: 10.1016/S0140-6736(17)31046-2
52. Haug V, Behle V, Benoit S, Kneitz H, Schilling B, Goebeler M, et al. Pembrolizumab-associated Mucous membrane pemphigoid in a Merkel cell carcinoma patient. Br J Dermatol. (2018). doi: 10.1111/bjd.16780. [Epub ahead of print].
53. Vaillant L, Bernard P, Joly P, Prost C, Labeille B, Bedane C, et al. Evaluation of clinical criteria for diagnosis of bullous pemphigoid. French bullous study group. Arch Dermatol. (1998) 134:1075–80. doi: 10.1001/archderm.134.9.1075
54. Hodi FS, O'Day SJ, McDermott DF, Weber RW, Sosman JA, Haanen JB, et al. Improved survival with ipilimumab in patients with metastatic melanoma. N Engl J Med. (2010) 363:711–23. doi: 10.1056/NEJMoa1003466
55. Robert C, Schachter J, Long GV, Arance A, Grob JJ, Mortier L, et l; KEYNOTE-006 investigators. pembrolizumab versus Ipilimumab in advanced melanoma. N Engl J Med. (2015) 26:2521–32. doi: 10.1056/NEJMoa1503093
56. Zitvogel L, Kroemer G. Targeting PD-1/PD-L1 interactions for cancer immunotherapy. Oncoimmunology (2012) 1:1223–5. doi: 10.4161/onci.21335
57. Thibult ML, Mamessier E, Gertner-Dardenne J, Pastor S, Just-Landi S, Xerri L, et al. PD-1 is a novel regulator of human B-cell activation. Int Immunol. (2013) 25:129–37. doi: 10.1093/intimm/dxs098
58. Wang W, Lau R, Yu D, Zhu W, Korman A, Weber J. PD1 blockade reverses the suppression of melanoma antigen-specific CTL by CD4+ CD25(Hi) regulatory T cells. Int Immunol. (2009) 21:1065–77. doi: 10.1093/intimm/dxp072
59. Bastuji-Garin S, Joly P, Picard-Dahan C, Bernard P, Vaillant L, Pauwels C, et al. Drugs associated with bullous pemphigoid. A case-control study. Arch Dermatol. (1996) 132:272–6. doi: 10.1001/archderm.1996.03890270044006
60. Bastuji-Garin S, Joly P, Lemordant P, Sparsa A, Bedane C, Delaporte E, et al. Risk factors for bullous pemphigoid in the elderly: a prospective case-control study. J Invest Dermatol. (2011) 131:637–43. doi: 10.1038/jid.2010.301
61. Stavropoulos PG, Soura E, Antoniou C. Drug-induced pemphigoid: a review of the literature. J Eur Acad Dermatol Venereol. (2014) 28:1133–40. doi: 10.1111/jdv.12366
62. García M, Aranburu MA, Palacios-Zabalza I, Lertxundi U, Aguirre C. Dipeptidyl peptidase-IV inhibitors induced bullous pemphigoid: a case report and analysis of cases reported in the European pharmacovigilance database. J Clin Pharm Ther. (2016) 41:368–70. doi: 10.1111/jcpt.12397
63. Benzaquen M, Borradori L, Berbis P, Cazzaniga S, Valero R, Richard MA, et al. Dipeptidyl peptidase-IV inhibitors, a risk factor for bullous pemphigoid. Retrospective multicenter case–control study in France and Switzerland. J Am Acad Dermatol. (2017) 78:1090–6. doi: 10.1016/j.jaad.2017.12.038
64. Béné J, Moulis G, Bennani I, Auffret M, Coupe P, Babai S, et al. Bullous pemphigoid and dipeptidyl peptidase IV-inhibitors: a case/non-case study in the French pharmacovigilance database. Br J Dermatol. (2016) 175:296–301. doi: 10.1111/bjd.14601
65. Varpuluoma O, Försti AK, Jokelainen K, Turpeinen M, Timonen M, Huilaja L, et al. Vildagliptin significantly increases the risk of bullous pemphigoid: a Finnish Nationwide Registry Study. J Invest Dermatol. (2018) 138:1659–61 doi: 10.1016/j.jid.2018.01.027
66. Vassileva S. Drug-induced pemphigoid: bullous and cicatricial. Clin Dermatol. (1998) 16:379–87. doi: 10.1016/S0738-081X(98)00008-X
67. Weber JS, Hodi FS, Wolchok JD, Topalian SL, Schadendorf D, Larkin J, et al. Safety profile of nivolumab monotherapy: a pooled analysis of patients with advanced melanoma.J Clin Oncol. (2017) 35:785–92. doi: 10.1200/JCO.2015.66.1389
68. Lopez AT, Khanna T, Antonov N, Audrey-Bayan C, Geskin L. A review of bullous pemphigoid associated with PD-1 and PD-L1 inhibitors. Int J Dermatol. (2018) 57:664–9. doi: 10.1111/ijd.13984
69. Joly P, Baricault S, Sparsa A, Bernard P, Bédane C, Duvert-Lehembre S, et al. Incidence and mortality of bullous pemphigoid in France. J Invest Dermatol. (2012) 132:1998–2004. doi: 10.1038/jid.2012.35
70. Topalian SL, Sznol M, McDermott DF, Kluger HM, Carvajal RD, Sharfman WH, et al. Survival, durable tumor remission, and long-term safety in patients with advanced melanoma receiving nivolumab. J Clin Oncol. (2014) 32:1020–30. doi: 10.1200/JCO.2013.53.0105
71. Robert C, Ribas A, Hamid O, Daud A, Wolchok JD, Joshua AM, et al. Durable complete response after discontinuation of pembrolizumab in patients with metastatic melanoma. J Clin Oncol. (2017) 36:1668–74. doi: 10.1200/JCO.2017.75.6270
72. Miremont-Salamé G, Théophile H, Haramburu F, Bégaud B. Causality assessment in pharmacovigilance: the French method and its successive updates. Thérapie (2016) 71:179–86. doi: 10.1016/j.therap.2016.02.010
Keywords: mucous membrane pemphigoid, bullous pemphigoid, melanoma, anti-programmed-death-1/death-ligand-1, immune checkpoints inhibitors, pembrolizumab, drug accountability study, adverse drug reaction
Citation: Zumelzu C, Alexandre M, Le Roux C, Weber P, Guyot A, Levy A, Aucouturier F, Mignot-Grootenboer S, Caux F, Maubec E and Prost-Squarcioni C (2018) Mucous Membrane Pemphigoid, Bullous Pemphigoid, and Anti-programmed Death-1/ Programmed Death-Ligand 1: A Case Report of an Elderly Woman With Mucous Membrane Pemphigoid Developing After Pembrolizumab Therapy for Metastatic Melanoma and Review of the Literature. Front. Med. 5:268. doi: 10.3389/fmed.2018.00268
Received: 23 June 2018; Accepted: 03 September 2018;
Published: 27 September 2018.
Edited by:
Cristina Has, Albert-Ludwigs-Universität Freiburg, GermanyReviewed by:
Marian Dmochowski, Poznan University of Medical Sciences, PolandHiroshi Koga, Kurume University School of Medicine, Japan
Copyright © 2018 Zumelzu, Alexandre, Le Roux, Weber, Guyot, Levy, Aucouturier, Mignot-Grootenboer, Caux, Maubec and Prost-Squarcioni. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Catherine Prost-Squarcioni, Y2F0aGVyaW5lLnByb3N0QGFwaHAuZnI=