
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
SYSTEMATIC REVIEW article
Front. Immunol. , 15 October 2020
Sec. Alloimmunity and Transplantation
Volume 11 - 2020 | https://doi.org/10.3389/fimmu.2020.567715
 Omid Rezahosseini1
Omid Rezahosseini1 Dina Leth Møller1
Dina Leth Møller1 Andreas Dehlbæk Knudsen1,2
Andreas Dehlbæk Knudsen1,2 Søren Schwartz Sørensen3,4
Søren Schwartz Sørensen3,4 Michael Perch4,5Finn Gustafsson2,4
Michael Perch4,5Finn Gustafsson2,4 Allan Rasmussen6
Allan Rasmussen6 Sisse Rye Ostrowski7
Sisse Rye Ostrowski7 Susanne Dam Nielsen1,4*
Susanne Dam Nielsen1,4*Background: Defining the optimal dosage of the immunosuppressive or duration of anti-infective agents is a challenge in solid organ transplant (SOT) recipients. We aimed to systematically review the literature regarding the use of T cell mediated immune functional assays (IFAs) for adjustment of the immunosuppressive or anti-infective agents in SOT recipients.
Methods: We systematically searched PubMed, Scopus, EMBASE, Web of Science (WOS), Cochrane Central Register of Controlled Trials (CENTRAL), and ClinicalTrials.gov to find human interventional studies or study protocols that used either in-house or commercially available IFAs for adjustment of the immunosuppressive or anti-infective agents in SOT recipients.
Results: We included six clinical trials and six study protocols. Four out of the six clinical trials used interferon-γ release assays for cytomegalovirus (IGRA-CMV), and five out of the six registered study protocols planned to use IGRA-CMV for adjustment of anti-CMV antiviral (Valganciclovir) prophylaxis or preemptive therapy in SOT recipients. Primary or secondary anti-CMV prophylaxes were discontinued in SOT recipients who had positive IGRA-CMV results without an increase in the rate of CMV infection or reactivation. Among other IFAs, one clinical trial used interferon-γ release assays for tuberculosis (IGRA-TB), and one study used ImmuKnow for adjustment of the duration and dosage of isoniazid and tacrolimus, respectively.
Conclusion: Our systematic review supports a promising role for the IGRA-CMVs for adjustment of the duration of anti-CMV antiviral prophylaxis in SOT recipients. There are limited data to support the use of IFAs other than IGRA-CMVs for adjustment of immunosuppressive or anti-infective agents. Further multicenter randomized clinical trials using IFAs other than IGRA-CMVs may help in personalized immunosuppressive or prophylactic anti-infective therapy in SOT recipients.
Solid-organ transplantation (SOT) is a life-saving treatment option for patients with terminal organ failure (1). To avoid rejection of the transplanted organ, SOT recipients receive life-long immunosuppressive therapy (1). Immunosuppressive therapy, however, is a double-edged sword; over-immunosuppression may precipitate cancers and infections, while under-immunosuppression increases the risk of graft rejection (2, 3). Consequently, monitoring of the immunosuppressive drug-level is part of the standard of care in SOT recipients. However, infection rates may differ in SOT recipients who receive the same immunosuppression regimen, and with equal trough level of the immunosuppressive agents (4). Moreover, SOT recipients usually receive a combination of immunosuppressive agents with different mechanisms of action (5, 6), and therapeutic drug monitoring of individual drugs may not accurately reflect the immune status. To prevent infections, SOT recipients may need prophylactic anti-infective agents for cytomegalovirus (CMV) disease, tuberculosis, pneumocystis pneumonia (PCP), and some other infective agents but there is no accurate measure to guide optimal duration of the prophylactic anti-infective agents in SOT recipients (7, 8). Thus, more precise tools to monitor the function of the immune system in SOT recipients and to guide the dosing of immunosuppressants and anti-infective agents are needed.
Immune functional assays (IFAs) are assays that use a stimulant to trigger the immune cells and afterward record the functional immune response (4, 9–11) As such, IFAs may be used to monitor the immune function and could be used in approaches toward personalized treatment with immunosuppressive and anti-infective agents. Several standardized (commercially available) and in-house IFAs have been introduced. A common feature of these IFAs is that mainly test T cell function (11–14). We aimed to systematically review the literature regarding the use of T cell mediated IFAs for adjustment of the immunosuppressive or anti-infective agents in SOT recipients.
Several commercially available in vitro IFAs are routinely used in research and clinical practice (9, 10). Assays such as ImmunKnow®, QuantiFERON®-TB Gold, T-SPOT®.TB, QuantiFERON®-CMV, T-Track® CMV, and T-SPOT®.CMV, are examples of commercially available IFAs (9–11). Below we summarize the mechanism of action of the mentioned commercially available in vitro IFAs used in solid organ transplantation.
Most of the cell functions are dependent on the production of adenosine triphosphate (ATP) and intracellular synthesis of ATP is a marker of cell activity (15). ImmunKnow® (Cylex, Columbia, USA) uses this principle to measure the activity of CD4+ T lymphocytes (10). In ImmuneKnow®, phytohemagglutinin (PHA) is used to stimulate lymphocytes, and the concentration of ATP is measured using the bioluminescence method (Figure 1) and reported in nanograms per milliliter (ng/ml) (10). According to the recommendations by manufacturer, ATP levels equal to or lower than 225 ng/mL are interpreted as a low immune cell response, while ATP levels equal to or higher than 525 ng/mL are interpreted as a high immune cell response (10).
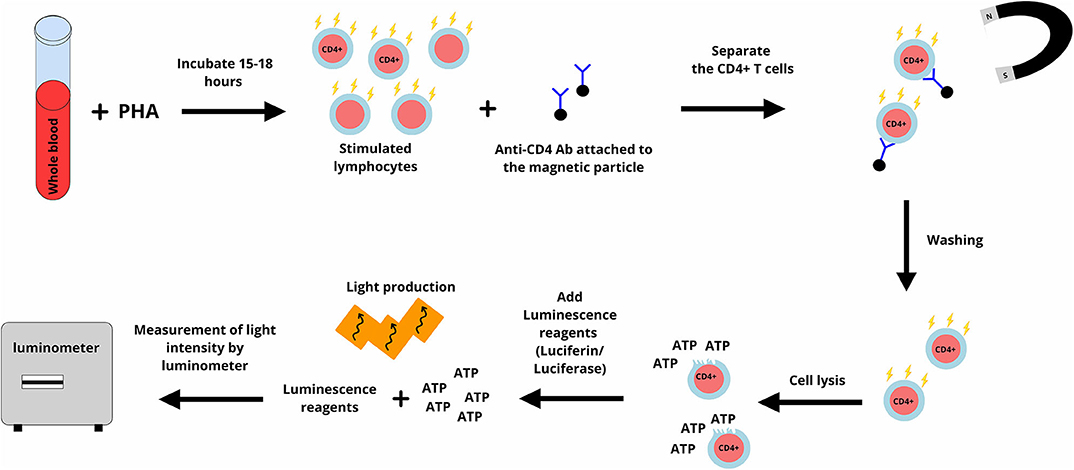
Figure 1. In ImmuKnow assay, a sample of whole blood is incubated with phytohemagglutinin (PHA) for 15–18 h. PHA stimulates lymphocytes and lymphocytes including CD4+ T lymphocytes produce adenosine triphosphate (ATP). Anti-CD4 antibodies attached to magnetic particles are added and attach to CD4+ T lymphocytes. CD4+ T lymphocytes are purified and after washing, are lysed. A luminescence reagent (a mixture of luciferin and luciferase) is added. ATP activates luciferase and this enzyme cut luciferin which results in light production. The produced light is measured using the bioluminescence method and reported in nanograms per milliliter (ng/ml). The figure designed by authors using Gravit Designer.
T-lymphocytes are the main target of most immunosuppressive agents, including cyclosporine and tacrolimus (5). Therefore, the ImmunKnow® assay is relevant as an IFA to monitor the immune system in SOT recipients. Immunosuppressive agents are present both in plasma and inside the red blood cells, ImmunKnow® is performed on a sample of whole blood to ensure that lymphocytes are tested in the presence of immunosuppressive drugs. Moreover, pre-purification of lymphocytes is not necessary to perform the ImmunKnow® assay and this decreases the iatrogenic stimulation of lymphocytes (10). Using whole blood is one of the advantages of this assay (16). However, PHA is not a specific stimulator of CD4+ T lymphocytes, and all types of living cells produce ATP. Furthermore, the requirement for purification and lysis of CD4+ T lymphocytes after stimulation are among the disadvantages of ImmunKnow®. This assay was approved by U.S. Food and Drug Administration (FDA) (17).
The interferon-gamma release assay for tuberculosis (IGRA-TB) is an in vitro assay that measures the production of IFN-γ following stimulation of T lymphocytes with Mycobacterium tuberculosis (M. tuberculosis) specific antigens (Figure 2). The antigens used are highly specific for M. tuberculosis and are not found in most of the non-tuberculous mycobacterium, including Bacillus Calmette-Guérin (BCG) (18). Currently, there are two commercially available IGRA-TB, the QuantiFERON®-TB Gold (Qiagen, Hilden, Germany) and T-SPOT®.TB assay (Oxford Immunotec, Abingdon, UK) (11, 18–20).
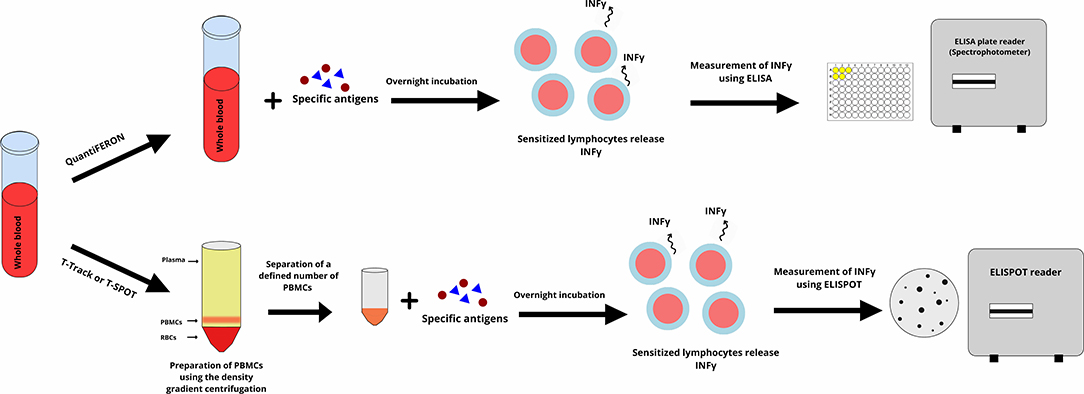
Figure 2. The Interferon-Gamma Release Assays (IGRAs) is performed according to two different methods. In the QuantiFERON, whole blood is incubated with specific antigens overnight (16–24 h). Antigens stimulate lymphocytes and sensitized lymphocytes release interferon-gamma. The interferon-gamma is measured using an enzyme linked immunosorbent assay (ELISA) and is reported as international units (IU) per milliliter. In the T-Track or T.SPOT assay peripheral blood mononuclear cell (PBMC) purified from whole blood are incubated with specific antigens overnight, and sensitized PBMCs release interferon-gamma. The interferon-gamma is measured using an enzyme-linked immunosorbent spot (ELISPOT) and is reported as the number of the formed spots on the ELISPOT's plate. The figure designed by authors using Gravit Designer.
In the QuantiFERON®-TB Gold In-Tube, whole blood is incubated with the M. tuberculosis specific antigens (early secreted antigenic target 6 (ESAT-6), culture filtrate protein 10 (CFP-10), and TB 7.7. The IFN-γ in the supernatant is measured using an enzyme-linked immunosorbent assay (ELISA) technique (Figure 2) and reported as international units (IU) per milliliter (18, 21). QuantiFERON®-TB Gold Plus is a new generation of QuantiFERON®-TB Gold that uses a peptide cocktail that mimick the ESAT-6 and CFP-10 antigens and stimulate CD4+ T lymphocytes, plus an additional set of peptides that stimulate CD8+ T lymphocytes (19).
In T-SPOT®.TB assay, peripheral blood mononuclear cells (PBMCs) are separated from a sample of whole blood using the Ficoll method (density gradient centrifugation), and a defined number of PBMCs are incubated with ESAT-6 and CFP 10 resulting in release of IFN-γ from sensitized T lymphocytes (20, 22). T-SPOT®.TB is an enzyme-linked immunosorbent spot (ELISPOT) assay with pre-coated plates with anti-IFN-γ antibodies (Figure 2) (11, 18). The use of highly M. tuberculosis specific antigens is one of the advantages of the QuantiFERON®-TB Gold and T-SPOT®.TB assays. This decreases the risk of false-positive results in individuals who have received the BCG vaccine or who are infected with other strains of mycobacteria. IGRAs, however, have a high number of indeterminate results and poor reproducibility mainly in immunocompromised patients (23–26). In comparison with QuantiFERON®-TB Gold, the T-SPOT®.TB assay is more laborious, takes more time, and needs specific laboratory equipment for purification of PBMCs (27, 28). Both assays approved by FDA and QuantiFERON®-TB Gold has the Conformitè Europëenne Mark (CE Mark) for commercial use in Europe (19, 20).
The principal of the IGRA-CMV is similar to the IGRA-TB (Figure 2), however, CMV specific antigens are used in IGRA-CMV (29). Three commercially available IGRA-CMV are available. QuantiFERON®-CMV (Qiagen, Hilden, Germany), T-Track® CMV assay (Lophius, Regensburg, Germany), and T-SPOT®.CMV (Oxford Immunotec, Abingdon, UK) (29–31).
The QuantiFERON®-CMV assay monitors the immune response to the cytomegalovirus (CMV). QuantiFERON®-CMV uses human leukocyte antigen (HLA) class I specific synthetic CMV epitopes to stimulate CMV-specific CD8+ T lymphocytes. These epitopes are peptide sequences of pp65, pp50, immediate-early 1 (IE-1), and the glycoprotein gB antigens (Figure 2) (29).
T-Track® CMV assay stimulates PBMCs with recombinant pp65 and IE-1 antigens that are called T-activated® proteins. These T-activated® proteins have been processed and can stimulate CD4+ T lymphocytes, CD8+ T lymphocytes, and natural killer cells (Figure 2) (30). In terms of principal, T-SPOT®.CMV is similar to T-Track CMV and uses pp65 and IE-1 CMV antigens as the stimulator (31).
When comparing QuantiFERON®-CMV, T-Track® CMV, and T-SPOT®.CMV, the QuantiFERON®-CMV is easier to perform as it does not need laboratory instruments for purification of PBMCs (Figure 2) (31). However, the ELISPOT based assays are more sensitive than ELISA based assays for the detection of cytokines including IFN-γ in the supernatant (32). QuantiFERON®-CMV, T-Track® CMV, and T-SPOT®.CMV are not FDA approved, however are CE Marked for commercial use in Europe (31, 33, 34).
We used the preferred reporting items for systematic reviews and meta-analyses (PRISMA) statement (35). The clinical question was designed according to the PICOS process and keywords selected to cover the clinical question (36). We searched PubMed, Scopus, EMBASE, Web of Science (WOS), Cochrane Central Register of Controlled Trials (CENTRAL), and ClinicalTrials.gov from 1 January 1970 to 15 May 2020. In a complementary search, we did a manual search in google using the mentioned keyword combinations. We also studied the reference list of eligible studies for any additional relevant papers.
Two independent investigators searched the mentioned databases using the same search terms and screened the retrieved papers by title and abstract. Potentially relevant papers were read in full-text and included if inclusion criteria were fulfilled.
The study protocol of this systematic review was registered on the international prospective register of systematic reviews (PROSPERO) with registration number of CRD42020182068.
We included studies on human recipients of solid organs of any type and any age group. The studies should use at least one of the commercially available or in-house IFAs for adjustment of dosage or duration of immunosuppressive and/or prophylactic anti-infective agents. We included interventional studies including randomized or non-randomized clinical trials. In regard to the type of articles only original articles, brief reports, research correspondence, or study protocols in English were included. We excluded studies that did not full-fill the inclusion criteria. We also excluded review articles, case reports, and conference proceedings.
We used the following MeSH terms in PubMed from 1 January 1970 to 15 May 2020 and found 75 hits.
(((((((“Interferon-gamma Release Tests” [Mesh]) OR “Enzyme-Linked Immunospot Assay” [Mesh]) OR “Phytohemagglutinins” [Mesh]) OR “Lipopolysaccharides” [Mesh]) OR “Mitogens” [Mesh])) AND (((“Antibiotic Prophylaxis” [Mesh]) OR “Immunosuppressive Agents” [Mesh]) OR “Anti-Infective Agents” [Mesh])) AND “Organ Transplantation”[Mesh].
Using the free-text terms in the same time-period, we found 797 hits in PubMed.
(((((((((((IGRA) OR QuantiFERON) OR ImmuKnow) OR T-Track) OR T.SPOT) OR TruCulture)) OR ((ELISpot) OR FluoroSpot))) OR ((((phytohaemagglutinin) OR lipopolysaccharides) OR proliferation assay) OR in-house assay))) AND ((((prophylaxis*) OR antibiotic) OR antiviral) OR immunosuppress*)) AND organ transplant*.
We used the same combination of the free-text terms to search Scopus, EMBASE, WOS, CENTRAL, and CinicalTrials.gov.
The selected papers were studied in full text by the same two investigators who did the search process (OR and DLM). We used the Cochrane risk of bias tools for randomized (RoB 2.0) and non-randomized (ROBINS-I) clinical trials (37, 38). We also used the online version of robvis (visualization tool) to draw the traffic light plots and weighted bar plots. Risk of bias tools use standard signaling questions and elicit aspects of a clinical trial that are related to the risk of bias. According to an algorithm and based on the answers to the signaling question, the risk of bias is evaluated (37, 38). Using traffic light plots and weighted bar plots, the judgment for risk of bias in randomized clinical trials is shown as either low, some concerns, or high, and the judgment for non-randomized clinical trials is shown as low, moderate, or high (37, 38).
The included studies were not homogenous, hence we could not perform a meta-analysis and only used narrative data synthesis for the results.
Out of 915 published papers and registered study protocol, six papers and six study protocols met our inclusion criteria and were selected for data extraction (Figure 3). The summary of the included papers and study protocols are shown in Tables 1, 2, respectively.
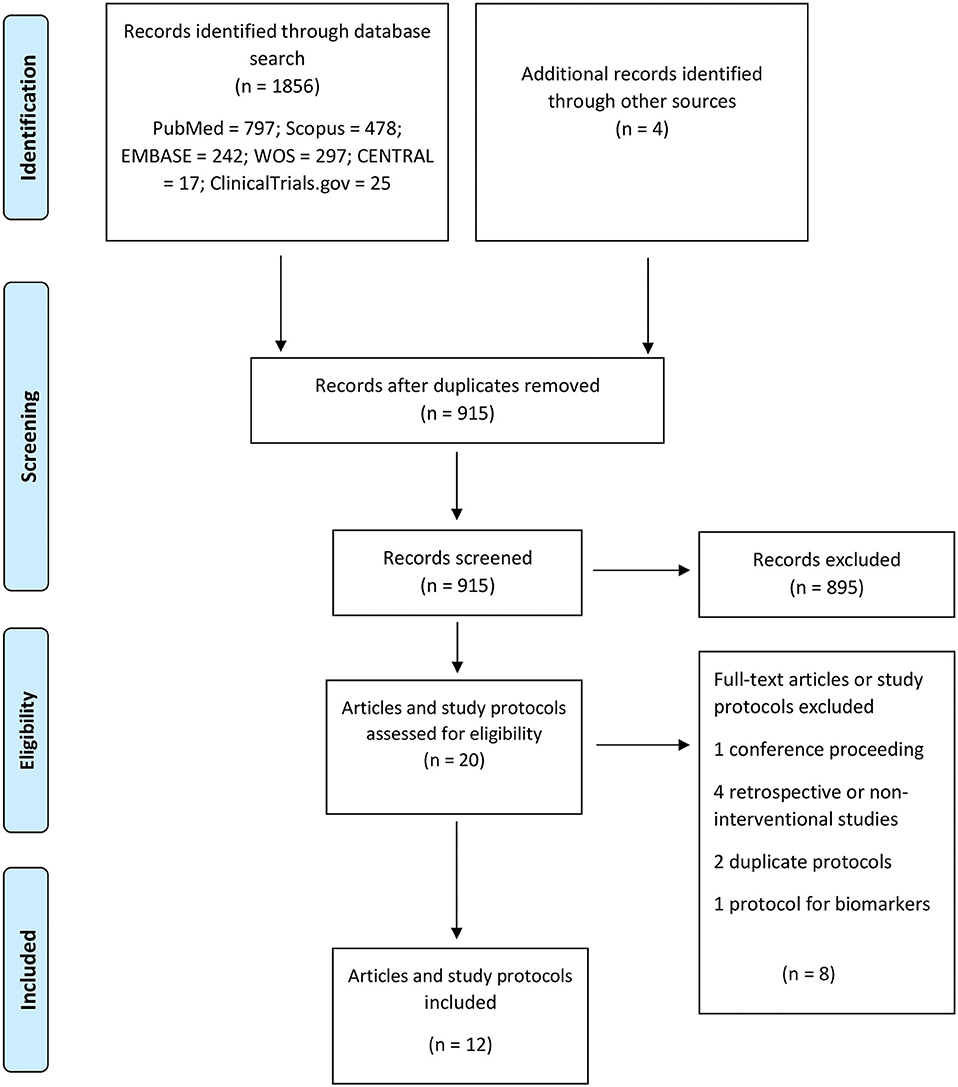
Figure 3. PRISMA flow diagram for the included studies.
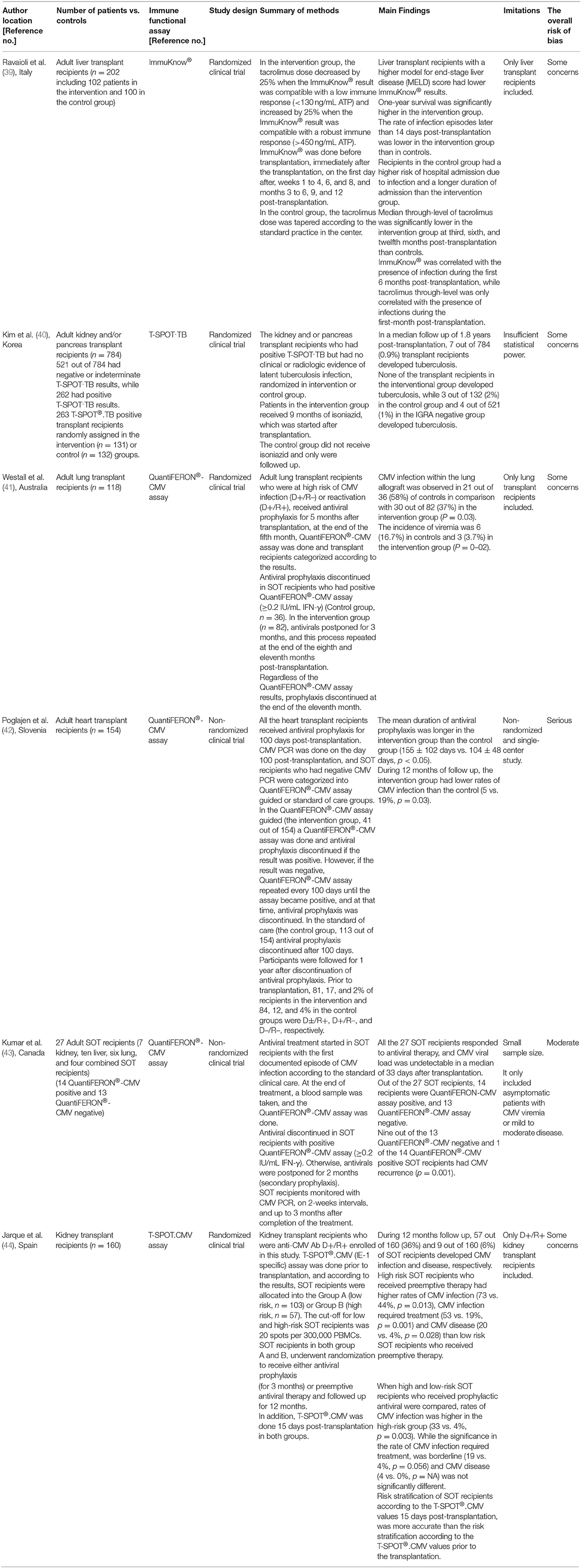
Table 1. Summary of the published interventional studies.
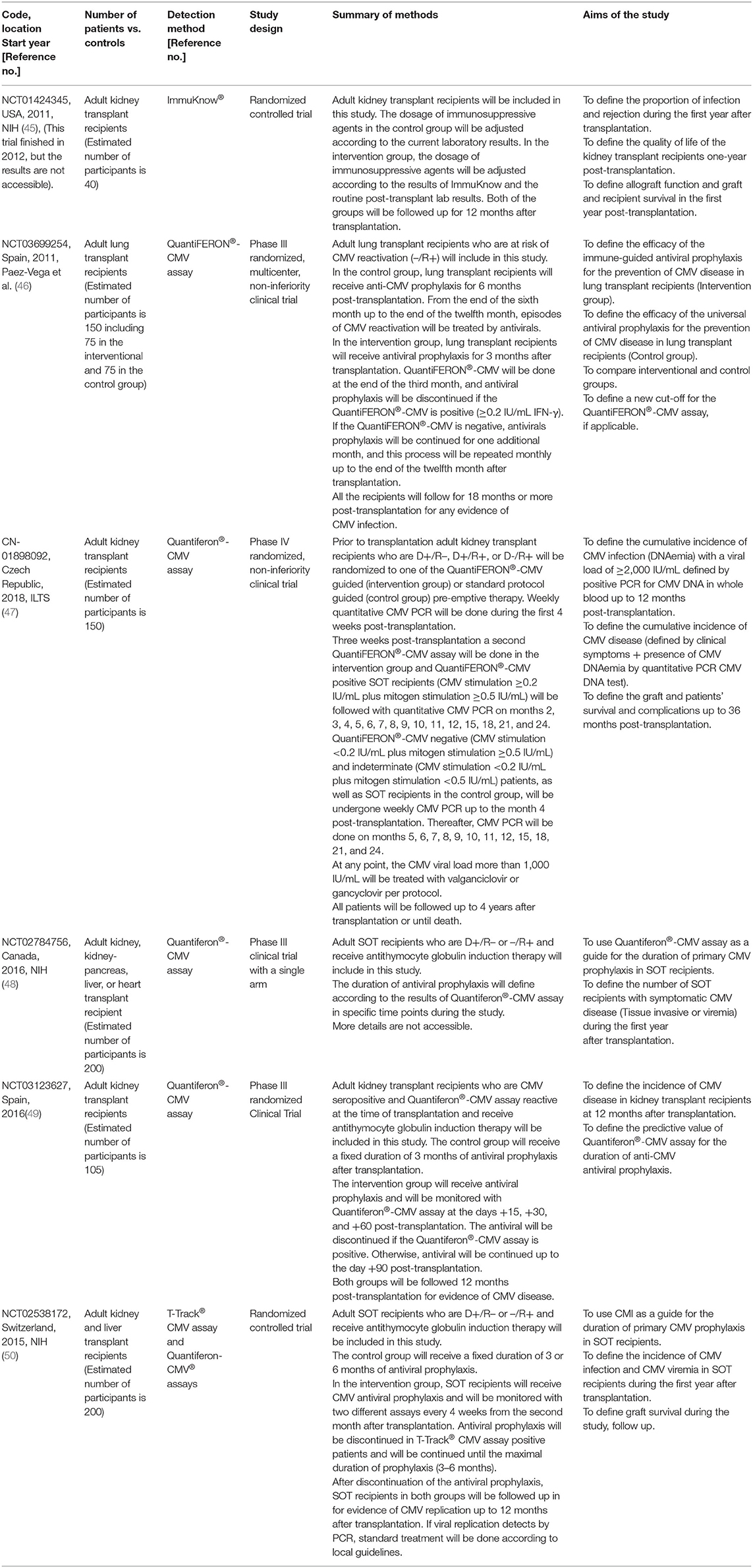
Table 2. Summary of the registered interventional study protocols.
In a randomized trial of 202 adult liver transplant recipients, SOT recipients were assigned to the intervention (100 out of 202) or control groups (102 out of 202) and were followed for 1-year post-transplantation. ImmuKnow® was used to guide the dosage of tacrolimus in the intervention group (39). The tacrolimus dosage was decreased by 25% when the ATP value was lower than 130 ng/mL and increased by 25% when the ATP value was higher than 450 ng/mL (39). In the control group, the tacrolimus dosage was adjusted according to the tacrolimus trough level. Tacrolimus trough level on month 3, 6, and 12 post-transplantation was lower in the intervention group than in the controls. SOT recipients in the intervention group had lower incidence of bacterial (32 vs. 46%, p < 0.05) and fungal (2 vs. 11%, p < 0.05) infections during the first year post-transplantation (39). However, the incidence of viral infections (22 vs. 23%) was similar. Lower ATP levels were associated with the presence of any infection during the first 6 months post-transplantation. In contrast, the tacrolimus trough level was only correlated with the presence of infection during the first month but not with infection in the last 11 months of the first year post-transplantation (39).
Among registered clinical trials, we only found one open-label randomized control trial that used ImmuKnow®, and this trial was registered in 2011 and finished in 2012 (45). However, we could not find any results or published articles related to the clinical trial. No other ongoing or published interventional studies have used ImmuKnow® to guide dosage of anti-infective agents in adult SOT recipients.
T-SPOT®.TB assay was used to decide when to initiate anti-tuberculosis prophylaxis in a randomized clinical trial of 784 adult kidney and/or pancreas transplant recipients in south Korea which is an intermediate-TB-burden country (40). SOT recipients with positive T-SPOT®.TB (263 out of 784), who did not have any clinical or radiologic evidence of active tuberculosis, were randomly assigned to the intervention (131 out of 263) or control (132 out of 263) groups. SOT recipients with negative or indeterminate T-SPOT®.TB results were followed in a parallel arm (521 out of 784) of the study. SOT recipients in the intervention group received 9 months of isoniazid as anti-tuberculosis prophylaxis, while controls, as well as patients in the parallel arm, did not receive isoniazid. In a median follow up of 1.8 years, none of the SOT recipients in the intervention group developed tuberculosis, while 2% of the controls (incidence rate of 1.22 per 100 person-years) and 0.8% of the SOT recipients in the parallel-arm (incidence rate of 0.43 per 100 person-years) were diagnosed with tuberculosis (40).
We could not find any other published interventional studies or study protocols that used QuantiFERON®-TB Gold for dose adjustment of immunosuppressive or anti-infective agents in SOT recipients.
A recent study used QuantiFERON®-CMV to adjust the duration of anti-CMV antiviral (valganciclovir) prophylaxis in a non-randomized clinical trial of 154 heart transplant recipients (42). Prior to transplantation, more than 80% of SOT recipients were CMV seropositive while had seropositive or seronegative donors. All the SOT recipients received antiviral prophylaxis for 100 days post-transplantation. CMV polymerase chain reaction (PCR) was done on the day 100 post-transplantation, and SOT recipients who had negative CMV PCR were categorized into QuantiFERON®-CMV assay guided or standard of care groups. In the QuantiFERON®-CMV assay guided (the intervention group, 41 out of 154) a QuantiFERON®-CMV assay was done and antiviral prophylaxis discontinued if the result was positive. However, if the result was negative, QuantiFERON®-CMV assay repeated every 100 days and antiviral prophylaxis continued until the assay became positive, and at that time, antiviral prophylaxis was discontinued. In the standard of care (the control group, 113 out of 154) antiviral prophylaxis discontinued after 100 days. Participants were followed for 1 year after discontinuation of antiviral prophylaxis. Using QuantiFERON®-CMV, the duration of anti-CMV antiviral prophylaxis was longer (155 ± 102 days vs. 104 ± 48 days, p < 0.05), but the rate of CMV infection (5 vs. 19%, p = 0.03) was lower in the intervention group (42).
In another clinical trial of 118 CMV seropositive lung transplant recipients, QuantiFERON®-CMV was used to guide the duration of antiviral prophylaxis (41). All the SOT recipients received antiviral prophylaxis for 5 months post-transplantation. QuantiFERON®-CMV was done at the end of the fifth month, and antiviral prophylaxis discontinued in SOT recipients who had positive results (control group). In SOT recipients who had negative QuantiFERON®-CMV, antiviral prophylaxis was continued, and viral PCRs were monitored regularly up to the time point when the QuantiFERON®-CMV result converted to positive (Interventional group). The maximum duration of antiviral prophylaxis in SOT recipients who had negative QuantiFERON®-CMV results was 11 months. The CMV infection in the lung allograft was defined as CMV viral load of more than 600 copies/mL in bronchoalveolar lavage (BAL). The incidence of CMV viremia (23 vs. 33%, p = ns) and CMV infection in the lung allograft (37 vs. 58%, p = 0.03) was lower in the intervention group than in the control group. In other words, QuantiFERON®-CMV guided prophylaxis favored a lower incidence of CMV in lung allograft (i.e. BAL) but not CMV viremia. Although, the incidence of severe lung CMV infection (CMV viral load >10,000 copies in BAL) did not differ between the two arms (11 vs. 11%, p = ns) (41).
Several trails of QuantiFERON®-CMV in SOT recipients are underway. An ongoing phase III clinical trial on an estimated number of 150 lung transplant recipients was registered in 2019. In this clinical trial, researchers plan to use QuantiFERON®-CMV guided anti-CMV prophylaxis to reduce the duration of antiviral prophylaxis (46).
A phase III clinical trial with an estimated number of 105 CMV-seropositive kidney transplant recipients plans to assess QuantiFERON®-CMV guided anti-CMV prophylaxis (49). A phase IV randomized clinical trial registered in 2018 with an estimated number of 150 adult kidney transplant recipients aims to use QuantiFERON®-CMV as a guide for preemptive therapy of the CMV infection (47).
A recent multicenter double-blind randomized clinical trial included adult kidney transplant recipients who were anti-CMV antibody donor positive / recipient positive prior to transplantation (44). This clinical trial used T-SPOT®.CMV and assigned SOT recipients into the interventional groups. T-SPOT®.CMV (IE-1 specific) assay was done prior to transplantation, and according to the results, SOT recipients were allocated into the low-risk or high-risk groups. The cut-off to discriminate low- and high-risk SOT recipients were 20 spots per 300,000 PBMCs. Both low- and high-risk SOT recipients underwent randomization to receive either anti-CMV prophylaxis (for 3 months) or preemptive antiviral therapy (44). In addition, T-SPOT®.CMV was done 15 days post-transplantation in both groups. During one-year follow-up post-transplantation, 57 out of 160 (36%) and 9 out of 160 (6%) of SOT recipients developed CMV infection and disease, respectively. High risk SOT recipients who received preemptive therapy had higher rates of CMV infection (73% vs. 44%, p = 0.013), CMV infection that required treatment (53 vs. 19%, p = 0.001) and CMV disease (20 vs. 4%, p = 0.028) than low-risk SOT recipients who received preemptive therapy. When low- and high-risk SOT recipients who received prophylactic antiviral treatment were compared, rates of CMV infection was higher in the high-risk group (33 vs. 4%, p = 0.003) (44).
Other than primary prophylaxis, QuantiFERON®-CMV has been used to guide the duration of secondary prophylaxis in a group of 27 SOT recipients including lung, liver, and kidney transplant recipients (43). Antiviral treatment started in SOT recipients with the first documented episode of CMV infection according to the standard of clinical care. At the end of treatment, the QuantiFERON®-CMV assay was done. Antiviral treatment was discontinued in SOT recipients with positive QuantiFERON®-CMV assay (≥0.2 IU/mL IFN-γ). Otherwise, oral valganciclovir or intravenous ganciclovir were continued for 2 months (secondary prophylaxis). SOT recipients were monitored with CMV PCR with 2-weeks intervals, and up to 3 months after completion of the treatment. SOT recipients who had negative QuantiFERON®-CMV, and received secondary prophylaxis, had a higher rate of recurrence during follow up compared to QuantiFERON®-CMV positive recipients (9 out of the 13 vs. 1 out of the 14, p = 0.001). The study concluded that in the SOT recipients who finished their treatment course and had a positive QuantiFERON®-CMV, it is reasonable to discontinue secondary antiviral prophylaxis (43).
A phase III clinical trial registered in 2016, aims to use QuantiFERON®-CMV guided anti-CMV prophylaxis in an estimated number of 200 adult kidney-, pancreas-, liver-, or heart transplant recipients who received induction therapy with antithymocyte globulin (48). An open-label clinical trial was registered in 2015 and planned to use T-Track® CMV to guide the duration of primary CMV antiviral prophylaxis in kidney-or liver-transplant recipients. The estimated number of SOT recipients to be included in this clinical trial was 200 and the status of the clinical trial is recruiting and results have not communicated yet (50).
TruCulture® is a relatively new IFA in comparison with ImmuKnow® and IGRAs. Hence, it has not been used in clinical trials on SOT recipients yet. We could not find any published or registered clinical trial that used TruCulture® in SOT recipients.
The overall risk of bias was with some concerns for 2 out of 4 randomized clinical trials. The other 2 randomized clinical trials had a high risk of bias (Figure 4). One of the non-randomized clinical trials had a serious overall risk of bias and the other one had a moderate risk of bias (Figure 5).
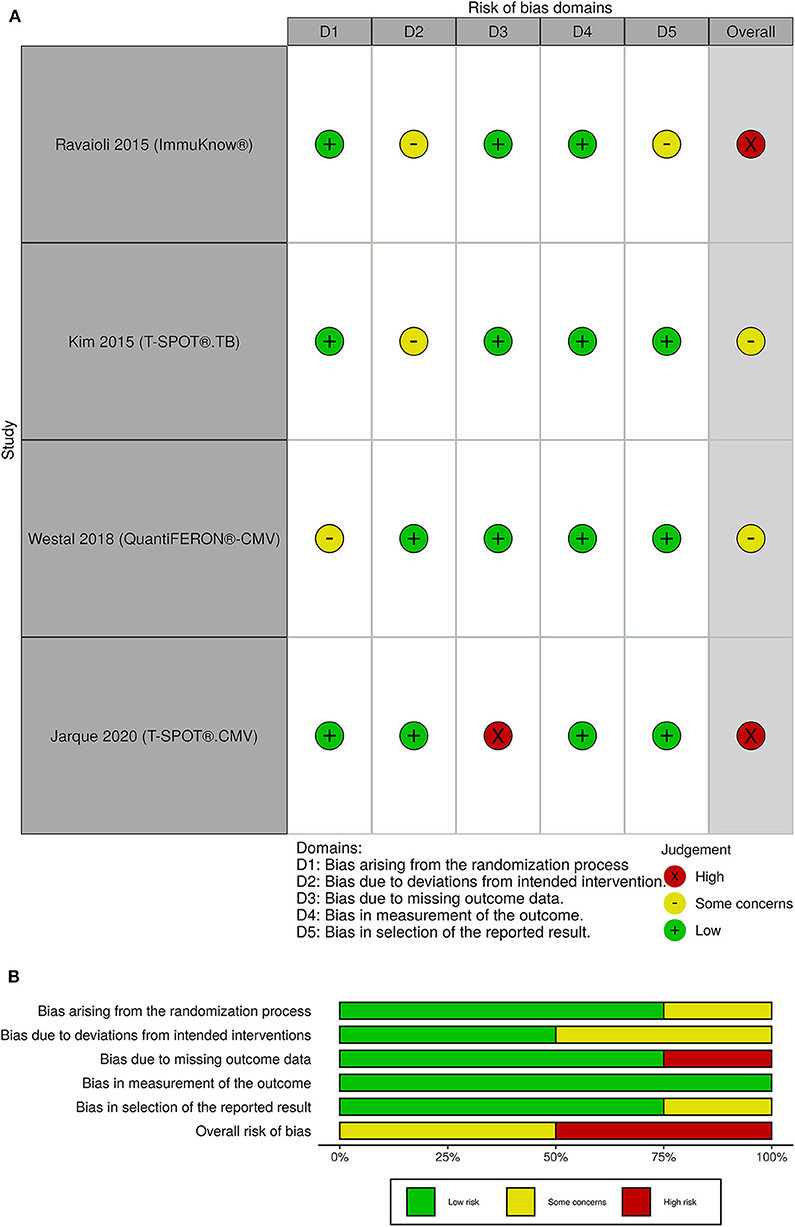
Figure 4. (A) Traffic light plots; (B) weighted bar plots for randomized clinical trials. The overall risk of bias was with some concerns for 2 out of 4 randomized clinical trials. The other 2 randomized clinical trials had a high risk of bias.
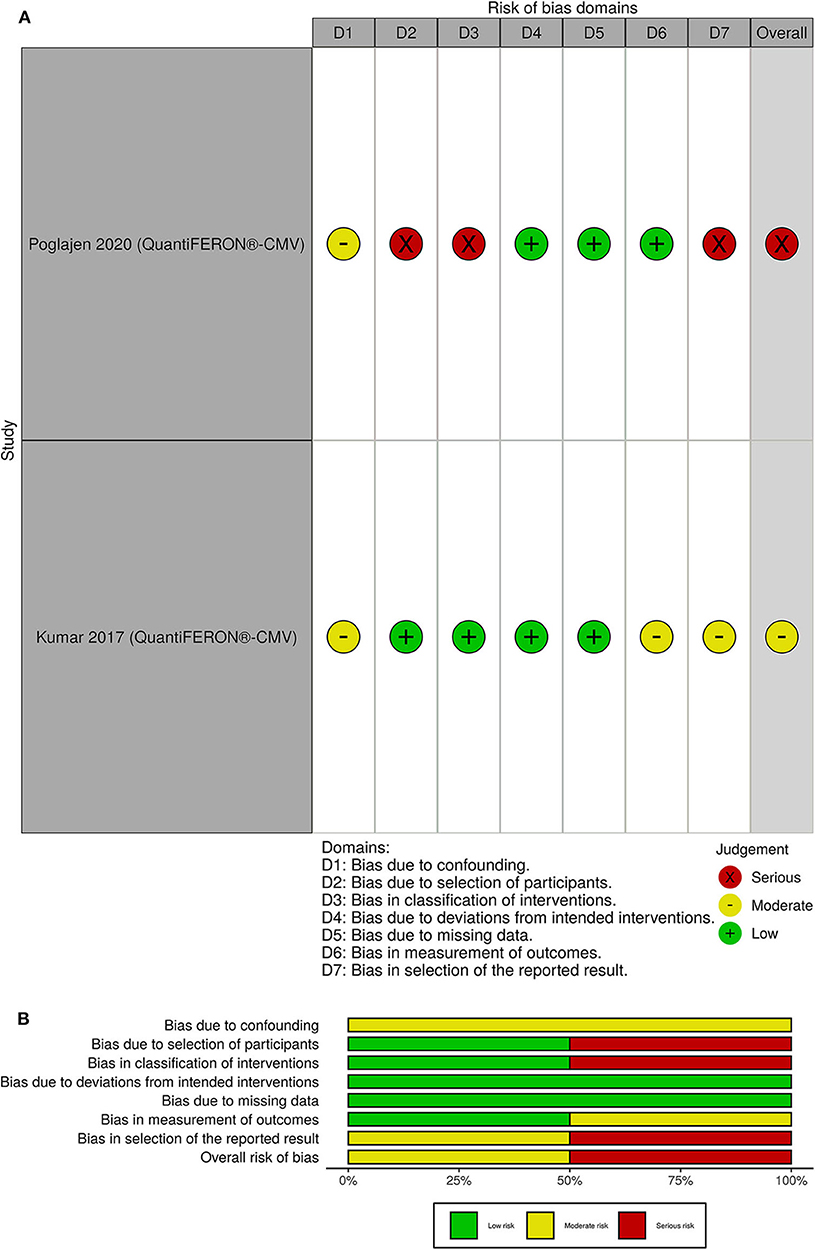
Figure 5. (A) Traffic light plots; (B) weighted bar plots for non-randomized clinical trials. One of the non-randomized clinical trials had a serious overall risk of bias and the other one had a moderate risk of bias.
In a systematic review, we found only six published papers and six registered protocols describing interventional studies aiming to investigate the use of IFAs for adjustment of the immunosuppressive or anti-infective agents in SOT recipients. Four out of the six published clinical trials used one of the commercially available IGRA-CMVs (41–44), and five out of the six registered protocols planned to use the IGRA-CMVs for adjustment of the antiviral prophylaxis or preemptive therapy (46, 48–50).
Infections and drug-related complications are highly prevalent and affect both the survival and quality of life of the SOT recipients (51–54). Only one published interventional study used ImmuKnow® to adjust the dosage of immunosuppression in liver transplant recipients (39). Using ImmuKnow® as a guide to dosing of tacrolimus subsequently decreased bacterial and fungal infections and improved survival in SOT recipients (39). However, it was a single-center study, only liver transplant recipients were included and there were some concerns for risk of bias due to deviation from intended intervention and reported results (39). ImmuKnow® uses PHA as a stimulant and measures the ATP that is produced by CD4+ T lymphocytes. Previous meta-analyses have not reached a consistent conclusion on the routine use of ImmuKnow® for prediction of infection in SOT recipients (55, 56). A meta-analysis included ten studies and showed that ImmuKnow® could be used for the prediction of infections in liver transplant recipients (55). The other meta-analysis included six studies in kidney transplant recipients but the results did not support the role of ImmuKnow® for the prediction of infections (56). It should be noted that the study that we included in our systematic review was not part of the previous meta-analyses (55, 56). Other than the need for further clinical trials to define the safety and feasibility of ImmuKnow® in SOT recipients, we need studies to define the most appropriate ATP cut-off for discrimination of SOT recipients who are at risk of infections (16).
One randomized clinical trial has used an IGRA-TB (T-SPOT®.TB) to guide the use of anti-tuberculosis prophylaxis in SOT recipients (40). In the mentioned study, tuberculosis developed in SOT recipients who did not receive anti-tuberculosis prophylaxis regardless of the T-SPOT®.TB results, although the incidence rate was higher in T-SPOT®.TB positive SOT recipients. The study was well-designed and the overall risk of bias was low (40). It is reported that IGRA-TBs have a high rate of indeterminate results (23), and underestimate the real burden of latent tuberculosis in SOT recipients (48). Therefore, according to the current evidence, it is not possible to decide for or against the initiation of anti-tuberculosis prophylaxis in SOT recipients who have negative or indeterminate T-SPOT®.TB results.
Despite prophylaxis and preemptive antiviral strategies, CMV remains an important cause of post-transplantation infections (51, 57). Moreover, CMV is among the main causes of early graft loss, mortality, and morbidity in SOT recipients (58). Given the importance and burden of CMV infections and accessibility of CMV-specific and commercially available IFAs, it is justifiable that most of the studies that we found targeted CMV.
The feasibility of the IGRA-CMVs for adjustment of the duration of primary or secondary CMV antiviral prophylaxis has been shown in SOT recipients (41–43). It seems to be possible to reduce the duration of primary or secondary CMV antiviral prophylaxis in SOT recipients who are QuantiFERON®-CMV positive post-transplantation (41–43), although the overall risk of bias for current clinical trials are moderate to high and solid evidence preferentially from larger well-designed studies including all types of transplanted solid organs are warranted. Other than QuantiFERON®-CMV, it is possible to use T-SPOT®.CMV for risk stratification of the SOT recipients (44). However, the best cut-off point for discrimination of the positive and negative IGRA-CMV results is not a fixed value. One of the ongoing clinical trials plans to define a new cut-off for QuantiFERON®-CMV in lung transplant recipients (37). The stimulating antigen, the method for measuring the response, and timing of the assessment can significantly affect the results and the cut-off value (44, 59).
In this systematic review, we used a wide range of keywords to find all the available evidence regarding the use of IFAs to guide the dosing of immunosuppressants or anti-infective agents in SOT recipients. It should be mentioned that in the current guidelines there are different clinical indications for use of the IGRA-CMV and IGRA-TB in SOT recipients. IGRA-TB is an assays used for risk assessment of latent TB prior to transplantation (60). Although IGRA-CMV can be used for risk assessment of CMV infection prior to transplantation, IGRA-CMV is mainly used for assessment of risk of CMV reactivation post-transplantation (58). We searched four medical research databases and two clinical trial registries. Nevertheless, some of the ongoing clinical trials might be registered in local or regional registries, and we may have missed such protocols in our systematic review.
In conclusion, our systematic review supports the role of IGRA-CMVs for adjustment of the duration of anti-CMV antiviral prophylaxis in SOT recipients. We do not have enough evidence regarding the routine use of the other T cell mediated IFAs in guiding duration and dosage of immunosuppressive agents or anti-infective agents in SOT recipients to make conclusions regarding the clinical utility. Currently, several ongoing clinical trials are underway, but large, randomized clinical trials including other T cell mediated IFAs and all types of transplanted solid organs are needed to evaluate the role of IFAs in guiding immunosuppressive and anti-infective therapy in SOT recipients.
The original contributions generated for this study are included in the article/supplementary material, further inquiries can be directed to the corresponding author/s.
OR, DM, SS, AR, MP, FG, SO, and SN designed the study. OR performed the initial search and wrote the first draft of the manuscript, DM and AK cross-checked the referenced articles. OR and DM summarized the articles. SS, AR, MP, FG, SO, and SN supervised the review. OR, DM, AK, SS, AR, MP, FG, SO, and SN revised and commented on the manuscript. All authors read and approved the final version of the manuscript.
This work was supported by the Novo Nordisk Foundation, Independent Research Fund (FSS) and the Research Foundation of Rigshospitalet.
OR received a grant from The Research Foundation of Rigshospitalet related, and a grant from A.P. Møller Fonden not related to this work; AK received a grant from The Danish Heart Foundation and a traveling grant from Gilead not related to this work; MP received a grant from Roche, non-financial support from Boehringer Ingelheim, personal fees from Mallinckrodt, Novartis, and Astra-Zeneca not related to this work; FG received personal fees from Abbott, Novartis, Boehringer-Ingelheim, Orion Pharma, Pfizer, Astra-Zeneca and had other financial relationship with Corvia not related to this work; SN received a grant from Novo Nordisk Foundation.
The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
1. Black CK, Termanini KM, Aguirre O, Hawksworth JS, Sosin M. Solid organ transplantation in the 21st century. Ann Transl Med. (2018) 6:409. doi: 10.21037/atm.2018.09.68
2. Ling X, Xiong J, Liang W, Schroder PM, Wu L, Ju W, et al. Can immune cell function assay identify patients at risk of infection or rejection? A meta-analysis. Transplantation. (2012) 93:737–43. doi: 10.1097/TP.0b013e3182466248
3. Mells G, Neuberger J. Long-term care of the liver allograft recipient. Semin Liver Dis. (2009) 29:102–20. doi: 10.1055/s-0029-1192059
4. Drabe CH, Sorensen SS, Rasmussen A, Perch M, Gustafsson F, Rezahosseini O, et al. Immune function as predictor of infectious complications and clinical outcome in patients undergoing solid organ transplantation (the ImmuneMo:SOT study): a prospective non-interventional observational trial. BMC Infect Dis. (2019) 19:573. doi: 10.1186/s12879-019-4207-9
5. Enderby C, Keller CA. An overview of immunosuppression in solid organ transplantation. Am J Manag Care. (2015) 21:s12–23.
6. Holt CD. Overview of immunosuppressive therapy in solid organ transplantation. Anesth Clin. (2017) 35:365–80. doi: 10.1016/j.anclin.2017.04.001
7. Hand J, Patel G. Antimicrobial stewardship in transplant patients. Curr Opin Organ Transplant. (2019) 24:497–503. doi: 10.1097/MOT.0000000000000661
8. Weston MW, Rinde-Hoffman D, Lopez-Cepero M. Monitoring cell-mediated immunity during immunosuppression reduction in heart transplant recipients with severe systemic infections. Clin Transplant. (2020) 34:e13809. doi: 10.1111/ctr.13809
9. Mouton W, Vega CA, Boccard M, Bartolo F, Oriol G, Lopez J, et al. Towards standardization of immune functional assays. Clin Immunol. (2019) 210:108312. doi: 10.1101/718627
10. Kowalski R, Post D, Schneider MC, Britz J, Thomas J, Deierhoi M, et al. Immune cell function testing: an adjunct to therapeutic drug monitoring in transplant patient management. Clin Transplant. (2003) 17:77–88. doi: 10.1034/j.1399-0012.2003.00013.x
11. Albert-Vega C, Tawfik DM, Trouillet-Assant S, Vachot L, Mallet F, Textoris J. Immune functional assays, from custom to standardized tests for precision medicine. Front Immunol. (2018) 9:2367. doi: 10.3389/fimmu.2018.02367
12. Ruhwald M, de Thurah L, Kuchaka D, Zaher MR, Salman AM, Abdel-Ghaffar A-R, et al. Introducing the ESAT-6 free IGRA, a companion diagnostic for TB vaccines based on ESAT-6. Sci Rep. (2017) 7:45969. doi: 10.1038/srep45969
13. Han SH. Immunological prediction of cytomegalovirus (CMV) replication risk in solid organ transplantation recipients: approaches for regulating the targeted anti-CMV prevention strategies. Infect Chemother. (2017) 49:161–75. doi: 10.3947/ic.2017.49.3.161
14. Martinez-Flores JA, Serrano M, Morales P, Paz-Artal E, Morales JM, Serrano A. Comparison of several functional methods to evaluate the immune response on stable kidney transplant patients. J Immunol Methods. (2014) 403:62–5. doi: 10.1016/j.jim.2013.11.019
15. Bonora M, Patergnani S, Rimessi A, De Marchi E, Suski JM, Bononi A, et al. ATP synthesis and storage. Purinergic Signal. (2012) 8:343–57. doi: 10.1007/s11302-012-9305-8
16. Andrikopoulou E, Mather PJ. Current insights: use of immuknow in heart transplant recipients. Prog Transplant. (2014) 24:44–50. doi: 10.7182/pit2014664
17. Bhorade SM, Janata K, Vigneswaran WT, Alex CG, Garrity ER. Cylex ImmuKnow assay levels are lower in lung transplant recipients with infection. J Heart Lung Transplant. (2008) 27:990−4. doi: 10.1016/j.healun.2008.06.005
18. Pai M, Denkinger CM, Kik SV, Rangaka MX, Zwerling A, Oxlade O, et al. Gamma interferon release assays for detection of mycobacterium tuberculosis infection. Clin Microbiol Rev. (2014) 27:3–20. doi: 10.1128/CMR.00034-13
22. Chee CBE, Gan SH, Khinmar KW, Barkham TM, Koh CK, Liang S, et al. Comparison of sensitivities of two commercial gamma interferon release assays for pulmonary tuberculosis. J Clin Microbiol. (2008) 46:1935–40. doi: 10.1128/JCM.02403-07
23. Wigg AJ, Narayana SK, Anwar S, Ramachandran J, Muller K, Chen JW, et al. High rates of indeterminate interferon-gamma release assays for the diagnosis of latent tuberculosis infection in liver transplantation candidates. Transpl Infect Dis. (2019) 21:e13087. doi: 10.1111/tid.13087
24. Tagmouti S, Slater M, Benedetti A, Kik SV, Banaei N, Cattamanchi A, et al. Reproducibility of interferon gamma (IFN-γ) release assays. A systematic review. Ann Am Thorac Soc. (2014) 11:1267–76. doi: 10.1513/AnnalsATS.201405-188OC
25. Du F, Xie L, Zhang Y, Gao F, Zhang H, Chen W, et al. Prospective comparison of QFT-GIT and T-SPOT.TB assays for diagnosis of active tuberculosis. Sci Rep. (2018) 8:5882. doi: 10.1038/s41598-018-24285-3
26. Hornum M, Mortensen KL, Kamper AL, Andersen AB. Limitations of the QuantiFERON-TB gold test in detecting mycobacterium tuberculosis infection in immunocompromised patients. Eur J Intern Med. (2008) 19:137–9. doi: 10.1016/j.ejim.2007.03.020
27. Kim TY, Chang HE, Lee SW, Seo SH, Hong YJ, Park JS, et al. A novel strategy for interpreting the T-SPOT.TB test results read by an ELISPOT plate imager. PLoS ONE. (2019) 14:e0222920. doi: 10.1371/journal.pone.0222920
28. Schmidt T, Schub D, Wolf M, Dirks J, Ritter M, Leyking S, et al. Comparative analysis of assays for detection of cell-mediated immunity toward cytomegalovirus M. tuberculosis in samples from deceased organ donors. Am J Transplant. (2014) 14:2159–67. doi: 10.1111/ajt.12787
29. Walker S, Fazou C, Crough T, Holdsworth R, Kiely P, Veale M, et al. Ex vivo monitoring of human cytomegalovirus-specific CD8+ T-cell responses using QuantiFERON-CMV. Transpl Infect Dis. (2007) 9:165–70. doi: 10.1111/j.1399-3062.2006.00199.x
30. Barabas S, Spindler T, Kiener R, Tonar C, Lugner T, Batzilla J, et al. An optimized IFN-γ ELISpot assay for the sensitive and standardized monitoring of CMV protein-reactive effector cells of cell-mediated immunity. BMC Immunol. (2017) 18:195. doi: 10.1186/s12865-017-0195-y
32. Tanguay S, Killion JJ. Direct comparison of ELISPOT and ELISA-based assays for detection of individual cytokine-secreting cells. Lymphokine Cytokine Res. (1994) 13:259–63.
33. T-Track® CMV. (2020). Available online at: https://www.lophius.com/products/t-track-cmv-elispot-kit.html (accessed August 17, 2020).
34. QuantiFERON®-CMV ELISA Package Insert. (2020). Available online at: https://www.quantiferon.com/wp-content/uploads/2018/10/L1075110-R05-QF-CMV-ELISA-IFU-CE.pdf (accessed August 17, 2020).
35. Moher D, Liberati A, Tetzlaff J, Altman DG, Group TP. Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. PLoS Med. (2009) 6:e1000097. doi: 10.1371/journal.pmed.1000097
36. Liberati A, Altman DG, Tetzlaff J, Mulrow C, Gøtzsche PC, Ioannidis JPA, et al. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate health care interventions: explanation and elaboration. PLoS Med. (2009) 6:e1000100. doi: 10.1371/journal.pmed.1000100
37. Sterne JAC, Hernán MA, Reeves BC, Savović J, Berkman ND, Viswanathan M, et al. ROBINS-I: a tool for assessing risk of bias in non-randomised studies of interventions. BMJ. (2016) 355:i4919. doi: 10.1136/bmj.i4919
38. Sterne JAC, Savovic J, Page MJ, Elbers RG, Blencowe NS, Boutron I, et al. RoB 2: a revised tool for assessing risk of bias in randomised trials. BMJ. (2019) 366:l4898. doi: 10.1136/bmj.l4898
39. Ravaioli M, Neri F, Lazzarotto T, Bertuzzo VR, Di Gioia P, Stacchini G, et al. Immunosuppression modifications based on an immune response assay: results of a randomized, controlled trial. Transplantation. (2015) 99:1625–32. doi: 10.1097/TP.0000000000000650
40. Kim SH, Lee SO, Park IA, Kim SM, Park SJ, Yun SC, et al. Isoniazid treatment to prevent TB in kidney and pancreas transplant recipients based on an interferon-gamma-releasing assay: an exploratory randomized controlled trial. J Antimicrob Chemother. (2015) 70:1567–72. doi: 10.1093/jac/dku562
41. Westall GP, Cristiano Y, Levvey BJ, Whitford H, Paraskeva MA, Paul E, et al. A randomized study of quantiferon cmv-directed vs. fixed-duration valganciclovir prophylaxis to reduce late CMV after lung transplantation. Transplantation. (2019) 103:1005–13. doi: 10.1097/TP.0000000000002454
42. Poglajen G, Zemljic G, Frljak S, Okrajšek R, Šebeštjen M, Cerar A, et al. Quantiferon-CMV guided virostatic prophylaxis after heart transplantation. J Hear Lung Transplant. (2019) 38:S119. doi: 10.1016/j.healun.2019.01.279
43. Kumar D, Mian M, Singer L, Humar A. An interventional study using cell-mediated immunity to personalize therapy for cytomegalovirus infection after transplantation. Am J Transplant. (2017) 17:2468–73. doi: 10.1111/ajt.14347
44. Jarque M, Crespo E, Melilli E, Gutierrez A, Moreso F, Guirado L, et al. Cellular immunity to predict the risk of cytomegalovirus infection in kidney transplantation: a prospective, interventional, multicenter clinical trial. Clin Infect Dis. (2020). doi: 10.1093/cid/ciz1209. [Epub ahead of print].
45. NIH. The Role of ImmuKnow® in the Management of Immunosuppressants in the Renal Transplant Patient. Charleston, WV: NIH (2011).
46. Paez-Vega A, Cantisan S, Vaquero JM, Vidal E, Luque-Pineda A, Lobo-Acosta MA, et al. Efficacy and safety of the combination of reduced duration prophylaxis followed by immuno-guided prophylaxis to prevent cytomegalovirus disease in lung transplant recipients (CYTOCOR STUDY): an open-label, randomised, non-inferiority clinical trial. BMJ Open. (2019) 9:e030648. doi: 10.1136/bmjopen-2019-030648
47. ILTS. Randomized Study Comparing QuantiFERON-CMV Based vs. Standard Cytomegalovirus (CMV) Surveillance Protocol in Pre-emptive Therapy for Cytomegalovirus Prevention After Renal. (2018). Available online at: https://www.cochranelibrary.com/central/doi/10.1002/central/CN-01898092/full (accessed May 25, 2020).
48. NIH. Cell-Mediated Immunity Based Primary Prophylaxis for CMV Infection in Organ Transplant Recipients. Toronto, ON: NIH (2016).
49. NIH. Randomized Clinical Trial, Open, Multicenter Parallel, no Suspension Inferiority Prophylactic Treatment With Valganciclovir in Kidney Transplant CMV-seropositive Cellular Immunity to Develop CD8 + CMV-Specific Treatment After Induction Thymoglobulin. NIH (2016).
51. van Delden C, Stampf S, Hirsch HH, Manuel O, Meylan P, Cusini A, et al. Burden and timeline of infectious diseases in the first year after solid organ transplantation in the swiss transplant cohort study. Clin Infect Dis. (2020). doi: 10.1093/cid/ciz1113. [Epub ahead of print].
52. Neuwirt H, Rudnicki M, Schratzberger P, Pirklbauer M, Kronbichler A, Mayer G. Immunosuppression after renal transplantation. Memo Mag Eur Med Oncol. (2019) 12:216–21. doi: 10.1007/s12254-019-0507-4
53. Gardiner BJ, Chow JK, Brilleman SL, Peleg AY, Snydman DR. The impact of recurrent cytomegalovirus infection on long-term survival in solid organ transplant recipients. Transpl Infect Dis. (2019) 21:e13189. doi: 10.1111/tid.13189
54. Ortega F, Valdés C, Ortega T. Quality of life after solid organ transplantation. Transplant Rev. (2007) 21:155–70. doi: 10.1016/j.trre.2007.06.002
55. Rodrigo E, Lopez-Hoyos M, Corral M, Fabrega E, Fernandez-Fresnedo G, San Segundo D, et al. ImmuKnow as a diagnostic tool for predicting infection and acute rejection in adult liver transplant recipients: a systematic review and meta-analysis. Liver Transplant. (2012) 18:1245–53. doi: 10.1002/lt.23497
56. Wang Z, Liu X, Lu P, Han Z, Tao J, Wang J, et al. Performance of the immuknow assay in differentiating infection and acute rejection after kidney transplantation: a meta-analysis. Transplant Proc. (2014) 46:3343–51. doi: 10.1016/j.transproceed.2014.09.109
57. Fishman JA. Infection in organ transplantation. Am J Transplant. (2017) 17:856–79. doi: 10.1111/ajt.14208
58. Kotton CN, Kumar D, Caliendo AM, Huprikar S, Chou S, Danziger-Isakov L, et al. The third international consensus guidelines on the management of cytomegalovirus in solid-organ transplantation. Transplantation. (2018) 102:900–31. doi: 10.1097/TP.0000000000002191
59. Kim SH. Interferon-gamma release assay for cytomegalovirus (IGRA-CMV) for risk stratification of posttransplant cmv infection: is it time to apply IGRA-CMV in routine clinical practice? Clin Infect Dis. (2020). doi: 10.1093/cid/ciz1211. [Epub ahead of print].
Keywords: transplantation, immune system, immunosuppressive agent, anti-infective agent, immune functional assay
Citation: Rezahosseini O, Møller DL, Knudsen AD, Sørensen SS, Perch M, Gustafsson F, Rasmussen A, Ostrowski SR and Nielsen SD (2020) Use of T Cell Mediated Immune Functional Assays for Adjustment of Immunosuppressive or Anti-infective Agents in Solid Organ Transplant Recipients: A Systematic Review. Front. Immunol. 11:567715. doi: 10.3389/fimmu.2020.567715
Received: 30 May 2020; Accepted: 31 August 2020;
Published: 15 October 2020.
Edited by:
Oriol Bestard, Hospital Universitario de Bellvitge, SpainReviewed by:
Oriol Manuel, Center Hospitalier Universitaire Vaudois (CHUV), SwitzerlandCopyright © 2020 Rezahosseini, Møller, Knudsen, Sørensen, Perch, Gustafsson, Rasmussen, Ostrowski and Nielsen. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Susanne Dam Nielsen, c2RuQGRhZGxuZXQuZGs=
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.