
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Immunol. , 27 May 2020
Sec. Primary Immunodeficiencies
Volume 11 - 2020 | https://doi.org/10.3389/fimmu.2020.00982
This article is part of the Research Topic Advances in Primary Immunodeficiency in Central-Eastern Europe View all 12 articles
 Marcin Ziętkiewicz1*†
Marcin Ziętkiewicz1*† Ewa Więsik-Szewczyk2*†
Ewa Więsik-Szewczyk2*† Aleksandra Matyja-Bednarczyk3
Aleksandra Matyja-Bednarczyk3 Katarzyna Napiórkowska-Baran4Zbigniew Zdrojewski1
Katarzyna Napiórkowska-Baran4Zbigniew Zdrojewski1 Karina Jahnz-Różyk2
Karina Jahnz-Różyk2Common variable immunodeficiency (CVID) is the most clinically significant primary antibody immunodeficiency recognized in adulthood. Previously published data have shown an average diagnostic delay of 10 years for Polish adult patients with CVID. In the current study, we aimed to analyze the current diagnostic delay of adult patients with CVID in Poland. To this end, we identified patients from four immunological centers specialized in the care of adult patients with primary immunodeficiencies (PID). Demographic and clinical data of patients were collected using an internet database. We identified 103 adult patients (F:M 44.7%:55.3%) in Poland with CVID. The median age at onset of symptoms was 24 (0–66), 33 (4–70) at diagnosis, and 37 (18–73) years at the time of analysis. The median diagnostic delay for the entire study population was 6 (0–57) years. However, this delay was higher in patients with symptom onset before the year 2000 than after the year 1999 [15 (0–57) vs. 3 (0–19) years; p < 0.001]. Comparing patients (median ≤ 6 years, N = 53) with short diagnostic delay (SDD) and those (median > 6 years, N = 50) with long diagnostic delay (LDD), the LDD group had a statistically significant higher incidence of infections of the lower respiratory tract before diagnosis (90.0 vs. 71.70%). During the entire observation period, cytopenias (44.00 vs. 22.64%), granulomatous lesions (28.00 vs. 11.32%), and solid tumors (14.00 vs. 1.89%) were significantly more frequent in the LDD group. In conclusion, we found a significant reduction in the median diagnostic delay in Polish CVID patients with disease onset in the last two decades.
Primary immunodeficiencies (PIDs) are rare diseases. Because of their innate nature, they are diagnosed mainly in childhood (1). More than half of PID cases are associated with a defect in antibody production or function (2). In this group, the most common symptomatic deficiency is common variable immunodeficiency (CVID) (1, 3). CVID is a heterogeneous group of disorders characterized by recurrent upper and lower respiratory tract infections, which occur in more than 85% of patients (4). Besides, up to 70% of patients have at least one non-infectious manifestation, such as autoimmunization, granulomatous lesions, unexplained polyclonal lymphoproliferation, enteropathy, or malignancy (5–7).
Epidemiological data indicate that CVID has two peaks of onset. The first peak occurs in childhood, and the second peak occurs in the third or fourth decade of life. However, symptoms of CVID can start at any time of life, even in elderly patients (8). In Europe, 60% of CVID diagnosis occurs in adults (Table 1).
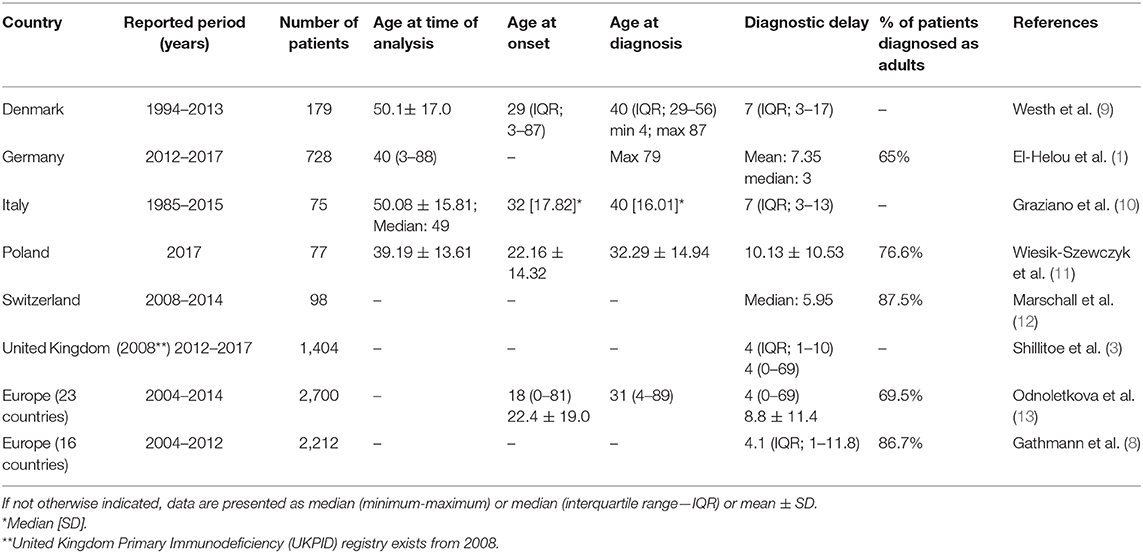
Table 1. Summary of most relevant CVID epidemiological studies in selected countries.
Due to low awareness among physicians regarding PID in adults, the onset of symptoms in adulthood, and a heterogeneous clinical picture of CVID, it may take up to several years to establish a proper diagnosis (14). The analysis of nearly 3,000 CVID cases showed a relationship between diagnosis delay and a higher risk of death [1.04 (1.02, 1.06), p = 0.0003], and organ complications (13). Aghamohammadi et al. demonstrated that the delay in diagnosis correlated significantly with the severity of the infection and the number of hospitalizations in children with primary antibody deficiencies, including CVID (15). Diagnostic delay of CVID generates high socioeconomic costs. According to Sadeghi et al., a diagnosis of CVID in a single patient can save US$ 6500 annually (16).
Similar to other rare diseases, data on CVID epidemiology are derived mainly from registries. In the last decade, several papers have been published, analyzing data from the ESID register (8, 13) or national registers (1, 3, 9, 10, 12). According to these studies, the diagnostic delay ranges between 3 and 9 years (Table 1). The period between the onset of first symptoms and CVID diagnosis is reportedly significantly shortened after 2000 in Spain (8) and the United Kingdom (3). In several other countries, there has been a tendency to shorten the delay of diagnosis, but the differences have not reached statistical significance (1, 8).
In Poland, we have very limited knowledge regarding CVID epidemiology. Considering the estimated prevalence of 1:25,000–1:50,000 and the population of Poland, which is about 38.386 million (17), there should be about 760–1,500 patients with CVID in this country. According to available data, 78 new cases were identified in 2014 (including 49 in children, 29 in adults) (18), and the median diagnostic delay in one of the pediatric centers (Kraków, 32 patients) was 1.8 years (8). According to data published in 2018, in a group of 77 adult Polish CVID patients, the mean diagnosis delay was 10.13 ± 10.53 years (19).
This study aimed to determine the length of the diagnostic delay of CVID in a group of Polish adult patients and compare groups of patients with short (SDD) and long diagnostic delay (LDD).
Data of CVID patients were collected from May 24, 2017, to December 31, 2019, using an internet database. The database did not contain personal data, and the patients were identified by code numbers. Only the attending physician of a particular patient could link the code number and patient's data. Entries older than 12 months were updated every year.
The study group consisted of patients treated under the Polish Ministry of Health's drug programs B.62 and B.78. A drug program is defined as follows: “guaranteed compensation, including therapies with innovative, expensive active substances, which are not financed by other guaranteed benefits. The treatment is carried out in selected disease entities and includes a strictly defined group of patients” (20). Within the aforementioned drug programs, immunoglobulin replacement therapy and monitoring are reimbursed for patients with primary humoral immunodeficiencies. Patients were treated at four immunological centers specializing in the care of adult patients with primary immunodeficiencies (Department of Allergology, Clinical Immunology and Internal Diseases, Ludwik Rydygier Collegium Medicum in Bydgoszcz Nicolaus Copernicus University in Torun, Bydgoszcz; Department of Internal Medicine, Connective Tissue Diseases and Geriatrics, Medical University of Gdansk, Gdansk; Outpatient Clinic for the Immunological and Hypercoagulable Diseases, The University Hospital in Krakow, Cracow; and Department of Internal Medicine, Pneumonology, Allergology and Clinical Immunology, Central Clinical Hospital of the Ministry of National Defense, Military Institute of Medicine, Warsaw). All patients met the Registry Working Definitions of the European Society for Immunodeficiencies (ESID) for CVID (21).
Of note, the most important epidemiological and clinical data are available as a Data Sheet, in the Supplementary Materials.
We collected data on the age of onset of the first symptoms, age at the time of CVID diagnosis, immunoglobulin (Ig) levels at the time of diagnosis, and type of infections before diagnosis. We also recorded the most important organ complications and co-morbidities associated with CVID from the time of the first symptoms until the data were entered in the database or updated. The year in which the first symptoms occurred was considered as the year in which the frequency of infection increased, a severe infection requiring hospitalization or intravenous antibiotic treatment, or the year in which symptoms of autoimmunity, polyclonal lymphoproliferation, or malignancy occurred. The age of onset of the first symptoms and that at the time of diagnosis was calculated as the difference in years between the year of birth of the patient and the year in which the event occurred. The diagnostic delay was calculated as the difference of full years between the years of onset of symptoms and diagnosis.
Due to the median delay in diagnosis for all patients (6 years), the cohort was divided into the following groups: SDD (median delay ≤ 6 years; N = 53) and LDD (median delay > 6 years; N = 50). The groups were compared in terms of age of first symptoms, age of diagnosis, as well as IgG, IgA, and IgM levels at the time of diagnosis, the incidence of infection in the period before diagnosis, and incidence of complications and co-morbidities throughout the observation period.
The normality of the observed values was tested using the Shapiro-Wilk test. For the continuous variables, mean and standard deviation were calculated if they followed a normal distribution; for non-normal distributions, the median (minimum to maximum) was used. Continuous variables were analyzed using Student's T, Mann-Whitney-U, and Kruskal–Wallis tests. Categorical variables were analyzed using the Chi-square test. For all data analyses, differences were considered statistically significant when p < 0.05. The statistical analysis was performed using the STATISTICA software (TIBCO Software Inc. Palo Alto, CA, USA), version 13.
The study was approved by the Ethics Committee of the Military Institute of Medicine, Warsaw (7/WIM/2020). All patients provided written consent to the collection and analysis of their demographic and medical data.
This study consisted of 103 adult patients, including 46 women (44.7%) and 57 men (55.3%) with CVID. At the time of data analysis, their median age was 37 (18–73) years.
The first symptoms of the disease commonly appeared from 0 to 14 years (39 patients; 37.9%) and 25–39 years of age (38 patients; 36.9%). Additionally, for the age of diagnosis, a bimodal distribution was observed. CVID was diagnosed in the highest percentage of patients at 10–19 years (21 patients; 20.4%) and 30–39 years of age (32 patients; 31.1%) (Figure 1A).
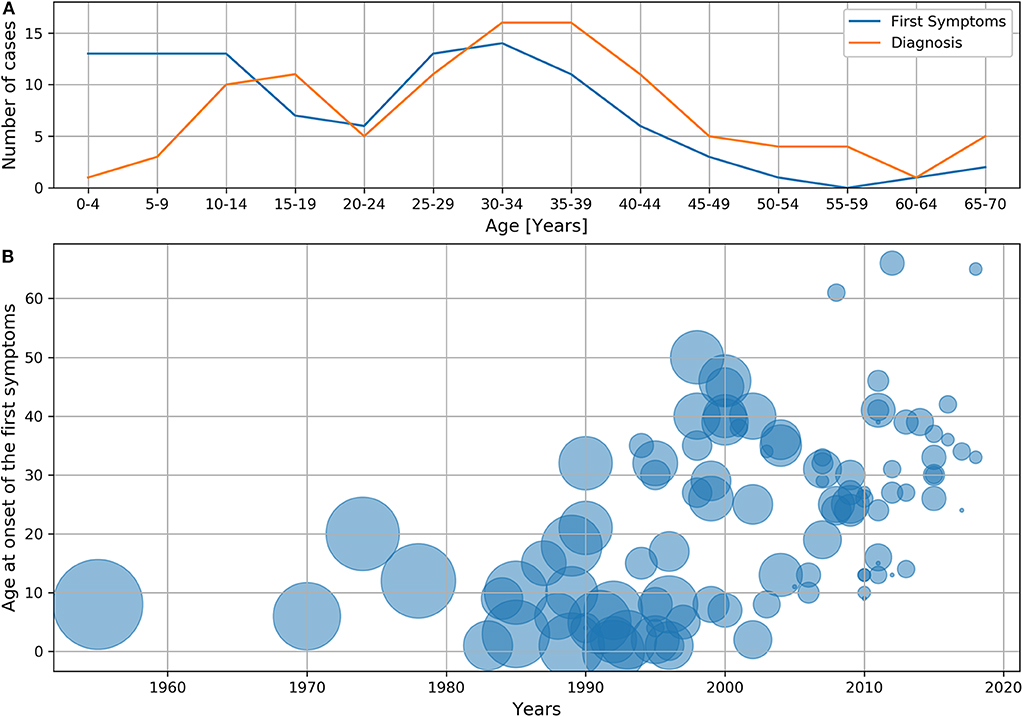
Figure 1. Age of first symptoms or diagnosis and diagnostic delay: (A) Age of first symptoms and age of diagnosis. (B) Diagnostic delay depending on the age and year at which the first symptoms occurred. The diameter of the circle corresponds to the delay expressed in years, and the center indicates the age and year at which the first symptoms occurred.
The median age at onset of symptoms was 24 (0–66) years. The first symptoms occurred in 44 patients (42.7%) before 18 years of age. In 41 patients (39.8%), disease onset occurred before the year 2000. In the decades following 1980, the mean age of patients at the onset of symptoms increased from 8.11 ± 5.97 to 29.7 ± 14.1 years (Table 2).
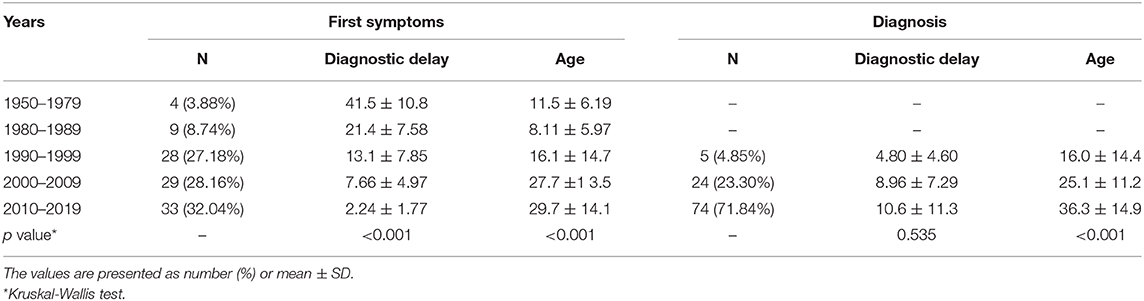
Table 2. Mean delay of CVID diagnosis and mean age of patients in subsequent decades, depending on the age of first symptoms and the age of diagnosis.
The median age at the time of CVID diagnosis was 33 years (4–70). In subsequent decades, the diagnosis was established in increasingly older patients. The age of diagnosis at specified intervals is presented in Table 2. Childhood (<18 years of age) diagnosis was established in 23 patients (22.3%). In 74 patients (71.8%), CVID was diagnosed between 2010 and 2019 (Table 2). In 7 cases (6.8%), including five patients under 18 years of age, the diagnosis was established in the same calendar year in which the first symptoms occurred.
The median diagnostic delay of the study group was 6 (0–57) years (mean 9.91 ± 10.3 years). In men, the median delay was 9.0 (0–39) years and 5.0 (0–57) years in women. These differences were not statistically significant (p = 0.191). The mean diagnostic delay was 41.5 ± 10.8 years in patients whose first symptoms occurred between 1950 and 1979. In subsequent decades, this delay systematically decreased, and from 2010 to 2019, it was 2.24 ± 1.77 years (Table 2). The median delay in patients with first symptoms before 2000 was 15 (0–57) years and 3 (0–19) years after 1999 (p < 0.001). Further, we observed a reduction in diagnostic delay, even if the first symptoms occurred in elderly patients (Figure 1B), which was the most prominent after the year 2000.
In the decades following 1990, the mean delay assessed at the time of diagnosis increased from 4.80 ± 4.60 to 10.6 ± 11.3 years. The differences in subsequent analyzed periods were not statistically significant (Table 2).
There were statistically significant differences between groups of patients with SDD and LDD (Table 3) in the age of appearance of first symptoms [27.0 (1–66) vs. 15.0 (0–50) p = 0.004], the age at which the diagnosis was established [31.0 (4–70) vs. 34.5 (12–70) p = 0.04], and the age at the time of analysis [35.0 (18–73) vs. 41.0 (19–72) p = 0.036]. In both groups, at the time of diagnosis, IgG, IgA, and IgM levels were comparable. Infections of the lower respiratory tract occurred in a significantly higher percentage of patients in the LDD group than in the SDD group (90.0 vs. 71.70%; p = 0.019). There were no significant differences in other infections between SSD and LDD groups.
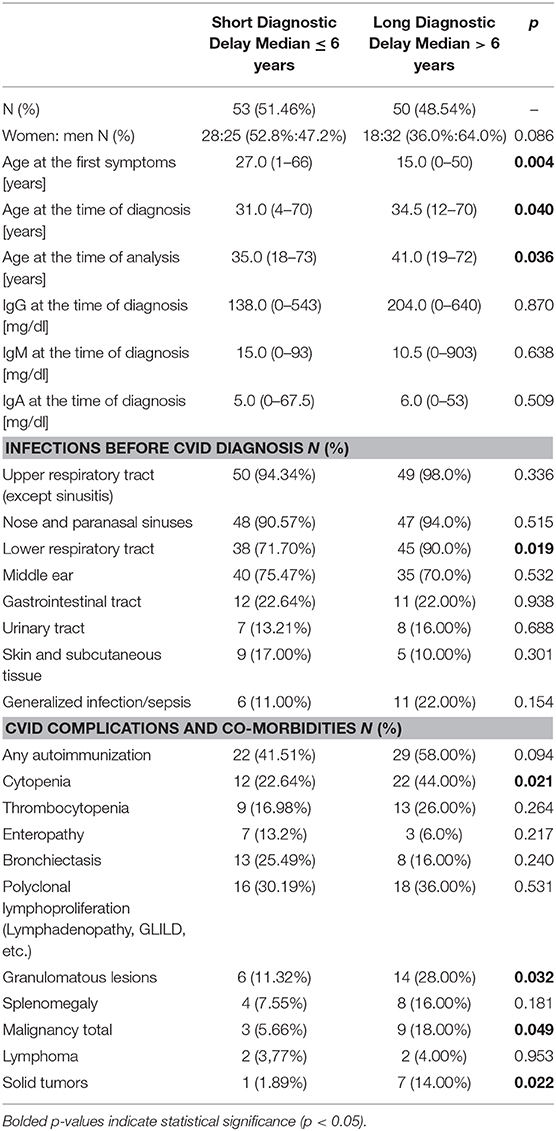
Table 3. Comparison of patients with short and long diagnostic delay.
Cytopenias (44.00 vs. 22.64% p = 0.021), granulomatous lesions (28.00 vs. 11.32% p = 0.032), and malignancies (18.00 vs. 5.66% p = 0.049), including solid tumors (14.0 vs. 1.89% p = 0.022), were significantly more frequent in the LDD group than in the SDD group (Table 3). Autoimmunization, thrombocytopenia (as the most frequent cytopenia), polyclonal lymphoproliferation, splenomegaly, and lymphoma were more frequent in the LDD group than in the SDD group, although these differences were not statistically significant. Further, in the SDD group, bronchiectasis, and enteropathy were more frequent. However, these differences were not significant.
According to data published after 2010, the median delay in CVID diagnosis (Table 1) ranges from 3 years in Germany (1) to 7 years in Italy (10) and Denmark (9). In the 23 European countries analyzed together, the median diagnostic delay is 4 (0–69) years, and the mean is 8.8 ± 11.4 years (13).
In our group, the median delay was 6 years. However, for patients whose first symptoms appeared between 2010 and 2019, the mean delay was shortened to slightly over 2 years. According to the 2014 ESID registry, a significant shortening of the median delay was achieved only in Spain (9.0 vs. 4.6 years) (8). Furthermore, the United Kingdom demonstrated a statistically significant but weak correlation for a decrease in diagnostic delay over time from 2012 to 2017 (3).
At present, in Poland, CVID diagnosis is more rapid than that before 2000, even in elderly patients. However, compared to other European countries, a lower percentage of patients whose diagnosis was established in the year in which the first symptoms occurred remains (6.8 vs. 16.0%) (13).
In the group of Polish patients, we observed an increase in the mean diagnostic delay, assessed at the time of diagnosis, over the last three decades (Table 2). This finding may result from patients who had undiagnosed CVID symptoms for several years. A similar phenomenon occurred in Europe, in which the mean delay assessed at the time of diagnosis before and in 1980 was 7.4 years, and in and after 2000 was 8.8 years (13).
Most CVID cases were identified in Poland after 1999, which is higher than in other European countries (95.15 vs. 69.1%) (13). This striking difference was possibly due to efforts by the Polish Ministry of Health, which provided reimbursements of immunoglobulin treatment for patients with primary immunodeficiency in 2015 as part of its drug programs (11). Additionally, after year 2000 new Polish centers for adult PID patients were established that improved accessibility for clinical immunologist consultations.
Comparing the group of patients with SDD and LDD, statistically significant differences were found between the age of first symptoms and the age at which CVID was diagnosed. Patients from the SDD group were older at the time of onset, while they were younger at the time of diagnosis compared to patients from the LDD group. This could be due to at least three reasons. First, at the time of analysis, there were no patients under 18 years old in the study group, which increased the median age at the onset of the first symptoms and decreased the median age at which the diagnosis was established. Second, in patients who were older at the time of data analysis, the first symptoms could have occurred in childhood, which lowered the age median when the first symptoms occurred in the LDD group. Third, before 2000, the delay in diagnosis was considerably longer than in recent years, which resulted in patients waiting longer to be diagnosed, even if symptoms occurred at a young age.
A statistically significant difference in the percentage of patients who had infections before CVID diagnosis was found exclusively in the case of lower respiratory tract infection, which was higher in the LDD group. This finding could be due to the delay in the initiation of IgG substitution.
Many studies have highlighted the occurrence of numerous complications and co-morbidities during the course of CVID (6, 8, 13, 22, 23). In this study cytopenias, granulomatous lesions, solid tumors, and neoplastic diseases were more frequent in the LDD group. The more frequent occurrence of the above-mentioned non-infectious complications in the LDD group could be a consequence of several phenomena. Due to low awareness among physicians of PID in adults, in patients who do not present with recurrent infections, diagnostics focus may divert from CVID. For instance, granulomatous lesions may occasionally be misdiagnosed as sarcoidosis (24). Moreover, the analysis of 21 patients with CVID and idiopathic thrombocytopenic purpura showed that only 19% of patients were diagnosed with immunodeficiency before the diagnosis of ITP (25). The more frequent occurrence of cancers, in the LDD group may be associated with the patients' older age and longer disease duration. In addition, Kiaee et al. performed a meta-analysis showing that CVID patients diagnosed with malignancy were older at the time of diagnosis, relative to patients without malignancy (5).
Recurrent lung infections are a recognized risk factor for bronchiectasis (26). Although the percentage of patients with lower respiratory tract infections was higher in the LDD group examined here, the percentage of patients with bronchiectasis in the LDD group was lower than that in the SDD group. This discrepancy may have resulted from the lack of discrimination between patients affected by chronic conditions from those with sporadic lower respiratory tract infections. Nevertheless, other cofactors, such as very low IgA or IgM level, or low neonatal Fc receptor expression, reportedly contribute to bronchiectasis (26). It can be assumed that the occurrence of bronchiectasis may have directed and accelerated the diagnosis toward CVID.
In the available literature, data on the relationship between delayed diagnosis and the occurrence of individual complications are unclear. Odnoletkova et al. reported in a group of 2700 patients with CVID that the diagnostic delay is associated with a higher risk of death, bronchiectasis, solid tumors, and enteropathy (13). In contrast, Razi et al., in a meta-analysis of 8,535 patients, did not show a correlation between delayed diagnosis and the occurrence of bronchiectasis. The incidence of bronchiectasis in the group of patients with 3 years or longer delay compared to the group with a shorter delay did not show a statistical difference (37.4 vs. 25.8%) (23). Further, in a group of 40 patients, researchers found a correlation between diagnosis delay and bronchiectasis (r = 0.323, p = 0.042), but did not confirm the correlation between chronic diarrhea and diagnostic delay (27).
Undoubtedly, further research on the relationship between the delayed diagnosis and occurrence of complications is necessary for a larger patient population.
Our study had a few limitations. Only adult patients were included in the analysis, which may have resulted in the overestimation of some indicators, such as the age of first symptoms or that of diagnosis. Further, four clinical, immunological centers participated in the study. Therefore, the analysis consisted of only a segment of Polish patients with CVID. Additionally, the relatively small number of patients made it difficult to analyze the incidence of rare complications statistically. Finally, for patients whose first symptoms occurred a long time ago (even in the 1950s), we had incomplete medical documentation, especially from the initial period of the disease. In a few cases, the type of infection before establishing a diagnosis was based on the oral records of the patients.
To the best of our knowledge, this is the first study on the delay in CVID diagnosis in the largest group of Polish patients. Notably, in recent years, the median time of delay in CVID diagnosis in Poland has significantly shortened and reached values comparable to that of other European countries. Presently, even an adult patient whose first symptoms occur at a late age can be diagnosed more quickly. However, further efforts are needed to assess the epidemiological and clinical landscape of patients with CVID and other primary immunodeficiencies (PID). To this end, we plan to establish the Polish Register of Primary Immunodeficiency Deficiencies in Adults (POLPIDA) that will facilitate a better, more comprehensive understanding of the needs of Polish patients for the diagnosis and therapy of PID and especially CVID. We believe that our continued effort will help reduce the incidence and severity of clinical complications.
All datasets generated for this study are included in the article/Supplementary Material.
The studies involving human participants were reviewed and approved by Ethics Committee of the Military Institute of Medicine, Warsaw, Poland. The patients/participants provided their written informed consent to participate in this study.
MZ and EW-S designed the study and wrote the first draft of the manuscript. This text was produced with an equal contribution of both authors. MZ, EW-S, AM-B, and KN-B collected data and performed managed the literature searches. MZ performed the statistical analyzes. AM-B, KN-B, ZZ, and KJ-R performed a critical revision of the manuscript for intellectual content. All authors have read and agreed to the published version of the manuscript.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fimmu.2020.00982/full#;supplementary-material
1. El-Helou SM, Biegner A-K, Bode S, Ehl SR, Heeg M, Maccari ME, et al. The german national registry of primary immunodeficiencies (2012–2017). Front Immunol. (2019) 10:1272. doi: 10.3389/fimmu.2019.01272
2. Modell V, Orange JS, Quinn J, Modell F. Global report on primary immunodeficiencies: 2018 update from the Jeffrey Modell Centers Network on disease classification, regional trends, treatment modalities, and physician reported outcomes. Immunol Res. (2018) 66:367–80. doi: 10.1007/s12026-018-8996-5
3. Shillitoe B, Bangs C, Guzman D, Gennery AR, Longhurst HJ, Slatter M, et al. The United Kingdom Primary Immune Deficiency. (UKPID) registry 2012 to 2017. Clin Exp Immunol. (2018) 192:284–91. doi: 10.1111/cei.13125
4. Moazzami B, Mohayeji Nasrabadi MA, Abolhassani H, Olbrich P, Azizi G, Shirzadi R, et al. Comprehensive assessment of respiratory complications in patients with common variable immunodeficiency. Ann Allergy, Asthma Immunol. (2020) 124:505–11. doi: 10.1016/j.anai.2020.01.019
5. Kiaee F, Azizi G, Rafiemanesh H, Zainaldain H, Sadaat Rizvi F, Alizadeh M, et al. Malignancy in common variable immunodeficiency: a systematic review and meta-analysis. Expert Rev Clin Immunol. (2019) 15:1105–13. doi: 10.1080/1744666X.2019.1658523
6. Gupta S, Pattanaik D, Krishnaswamy G. Common variable immune deficiency and associated complications. Chest. (2019) 156:579–93. doi: 10.1016/j.chest.2019.05.009
7. Ho H-E, Cunningham-Rundles C. Non-infectious complications of common variable immunodeficiency: updated clinical spectrum, sequelae, and insights to pathogenesis. Front Immunol. (2020) 11:149. doi: 10.3389/fimmu.2020.00149
8. Gathmann B, Mahlaoui N, Ceredih L, Gérard L, Oksenhendler E, Warnatz K, et al. Clinical picture and treatment of 2212 patients with common variable immunodeficiency. J Allergy Clin Immunol. (2014) 134:116–26. doi: 10.1016/j.jaci.2013.12.1077
9. Westh L, Mogensen TH, Dalgaard LS, Bernth Jensen JM, Katzenstein T, Hansen A-BE, et al. Identification and characterization of a nationwide danish adult common variable immunodeficiency cohort. Scand J Immunol. (2017) 85:450–61. doi: 10.1111/sji.12551
10. Graziano V, Pecoraro A, Mormile I, Quaremba G, Genovese A, Buccelli C, et al. Delay in diagnosis affects the clinical outcome in a cohort of cvid patients with marked reduction of iga serum levels. Clin Immunol. (2017) 180:1–4. doi: 10.1016/j.clim.2017.03.011
11. Wiesik-Szewczyk E, Jahnz-Rózyk K, Kucharczyk A. Current treatment options with immunoglobulin G for adult patients with primary immunodeficiency disease in Poland. J Heal Policy Outcomes Res. (2014) 2:42–9. doi: 10.7365/JHPOR.2014.2.5
12. Marschall K, Hoernes M, Bitzenhofer-Grüber M, Jandus P, Duppenthaler A, Wuillemin WA, et al. The swiss national registry for primary immunodeficiencies: report on the first 6 years' activity from 2008 to 2014. Clin Exp Immunol. (2015) 182:45–50. doi: 10.1111/cei.12661
13. Odnoletkova I, Kindle G, Quinti I, Grimbacher B, Knerr V, Gathmann B, et al. The burden of common variable immunodeficiency disorders: a retrospective analysis of the European Society for Immunodeficiency. (ESID) registry data. Orphanet J Rare Dis. (2018) 13:201. doi: 10.1186/s13023-018-0941-0
14. Ilkjær FV, Rasmussen LD, Martin-Iguacel R, Westh L, Katzenstein TL, Hansen A-BE, et al. How to identify common variable immunodeficiency patients earlier: general practice patterns. J Clin Immunol. (2019) 39:641–52. doi: 10.1007/s10875-019-00666-9
15. Aghamohammadi A, Bahrami A, Mamishi S, Mohammadi B, Abolhassani H, Parvaneh N, et al. Impact of delayed diagnosis in children with primary antibody deficiencies. J Microbiol Immunol Infect. (2011) 44:229–34. doi: 10.1016/j.jmii.2011.01.026
16. Sadeghi B, Abolhassani H, Naseri A, Rezaei N, Aghamohammadi A. Economic burden of common variable immunodeficiency: annual cost of disease. Exp Rev Clin Immunol. (2015) 11:681–8. doi: 10.1586/1744666X.2015.1029457
17. Central Statistical Office. Population. Size and Structure and Vital Statistics in Poland by Territorial Division in 2019. As of 30th June (2019) Available online at: https://stat.gov.pl/obszary-tematyczne/ludnosc/ludnosc/ludnosc-stan-i-struktura-w-przekroju-terytorialnym-stan-w-dniu-30-06-2019,6,26.html (accessed February 8, 2020).
18. Pac M, Bernatowska E. Comprehensive activities to increase recognition of primary immunodeficiency and access to immunoglobulin replacement therapy in Poland. Eur J Pediatr. (2016) 175:1099–105. doi: 10.1007/s00431-016-2746-2
19. Wiȩsik-Szewczyk E, Ziȩtkiewicz M, Matyja-Bednarczyk A, Napiórkowska-Baran K, Suchanek H, Jahnz-Rózyk K. The first Polish cohort of adult patients with common variable immunodeficiency from 4 specialized centers: do we provide standards of care? Polish Arch Intern Med. (2018) 128:563–6. doi: 10.20452/pamw.4315
20. Programy, lekowe - Ministerstwo Zdrowia - Portal Gov,.pl. Available online at: https://www.gov.pl/web/zdrowie/programy-lekowe (accessed February 8, 2020).
21. ESID Registry. Working Definitions for Clinical Diagnosis of PID. Available online at: https://esid.org/Working-Parties/Registry-Working-Party/Diagnosis-criteria (accessed december 30, 2019).
22. Maglione PJ. Autoimmune and lymphoproliferative complications of common variable immunodeficiency. Curr Allergy Asthma Rep. (2016) 16:19. doi: 10.1007/s11882-016-0597-6
23. Ramzi N, Jamee M, Bakhtiyari M, Rafiemanesh H, Zainaldain H, Tavakol M, et al. Bronchiectasis in common variable immunodeficiency: a systematic review and meta-analysis. Pediatr Pulmonol. (2020) 55:292–9. doi: 10.1002/ppul.24599
24. Verbsky J, Routes J. Sarcoidosis and common variable immunodeficiency: similarities and differences. Semin Respir Crit Care Med. (2014) 35:330–5. doi: 10.1055/s-0034-1376862
25. Michel M, Chanet V, Galicier L, Ruivard M, Levy Y, Hermine O, et al. Autoimmune thrombocytopenic purpura and common variable immunodeficiency: analysis of 21 cases and review of the literature. Medicine. (2004) 83:254–63. doi: 10.1097/01.md.0000133624.65946.40
26. Wall LA, Wisner EL, Gipson KS, Sorensen RU. Bronchiectasis in primary antibody deficiencies: a multidisciplinary approach. Front Immunol. (2020) 11:522. doi: 10.3389/fimmu.2020.00522
Keywords: primary antibody deficiency, hypogammaglobulinemia, common variable immunodeficiency, diagnostic delay, adults, epidemiology
Citation: Ziętkiewicz M, Więsik-Szewczyk E, Matyja-Bednarczyk A, Napiórkowska-Baran K, Zdrojewski Z and Jahnz-Różyk K (2020) Shorter Diagnostic Delay in Polish Adult Patients With Common Variable Immunodeficiency and Symptom Onset After 1999. Front. Immunol. 11:982. doi: 10.3389/fimmu.2020.00982
Received: 01 March 2020; Accepted: 27 April 2020;
Published: 27 May 2020.
Edited by:
Ismail Reisli, Necmettin Erbakan University, TurkeyReviewed by:
Asghar Aghamohammadi, Tehran University of Medical Sciences, IranCopyright © 2020 Ziętkiewicz, Więsik-Szewczyk, Matyja-Bednarczyk, Napiórkowska-Baran, Zdrojewski and Jahnz-Różyk. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Marcin Ziętkiewicz, bWFyY2luLnppZXRraWV3aWN6QGd1bWVkLmVkdS5wbA==; Ewa Więsik-Szewczyk, ZXdhLncuc3pld2N6eWtAZ21haWwuY29t
†These authors have contributed equally to this work
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.