 Gabriella Moroni
Gabriella Moroni Mirco Belingheri
Mirco Belingheri Giulia Frontini1
Giulia Frontini1 Piergiorgio Messa
Piergiorgio Messa- 1Dialysis, and Renal Transplant Unit, Fondazione IRCCS Ca' Granda Ospedale Maggiore Policlinico, Milan, Italy
- 2Department of Clinical Science and Community, Università degli Studi di Milano, Milan, Italy
IgA nephropathy (IgAN) is the most common primary glomerular disease worldwide. The disease generally runs an indolent course but may lead to ESRD in 20–30% of patients in 20 years or more after diagnosis. Patients with IgA nephropathy are ideal candidates for renal transplant because they are generally relatively young and with few comorbidities. Their graft survival is better or comparable to that of controls at 10 years, though few data are available after 10 years of follow-up. Recurrence of the original disease in the graft is a well-known complication of transplant in IgAN and is a significant cause of deterioration of graft function. Recurrent IgAN rarely manifests clinically before 3 years post transplantation. Recurrence rate is estimated to be around 30% with considerable differences among different series. Despite these factors there is no certain recurrence predictor, young age at renal transplant, rapid progression of the original disease and higher levels of circulating galactose-deficient IgA1 and IgA-IgG immune complexes are all associated with a higher rate of recurrence. Which pathogenetic mechanisms are responsible for the progression of the recurrence to graft function deterioration, and what therapy can prevent or slow down the progression of the disease in the graft, are open questions. The aim of this review is to describe the clinical outcome of renal transplantation in IgA patients with attention to the rate and the predictors of recurrence and to discuss the available therapeutic options for the management of recurrence.
Introduction
Glomerulonephritis (GN) is one of the most common diseases responsible for ESRD in the renal registries worldwide with an incidence ranging from 10.5 to 38.2% and a prevalence from 17.6 to 53.5% (1). In Australia, in the period between 2010 and 2013, IgAN was responsible for 16% of all incidents ESRD (2). Kidney transplantation is the best therapeutic option for IgAN patients. They have greater access to kidney transplant compared to patients with other kidney diseases because they are generally young and with few comorbidities. In the United States, between 2007 and 2011, the proportion of patients who received a kidney transplant within 1 year was 30.2% for IgAN compared to 2.4% for those with diabetes (3).
IgAN frequently recurs in the graft. Owing to the progressive improvement of graft survival resulting from reduced incidence of acute rejection, the number of patients potentially exposed to recurrence has increased. The incidence of IgAN recurrence is not clearly estimated; it is reported to range from 9 to 53% (4, 5), but the incidence increases if we consider only patients submitted to graft biopsy. Several reasons can account for this large discrepancy. The variable indication to graft biopsy in the different centers is one of the reasons. The rate of IgAN recurrence is higher in studies in which protocol biopsies are performed (5) in comparison to studies that reported graft biopsies done for clinical reasons only (6, 7) and in Registry analysis (4). As a matter of fact, recurrences of IgAN can be “histological only” when diagnosed on protocol biopsies in asymptomatic patients; or “clinical,” when associated with urinary abnormalities and/or graft dysfunction. The duration of post-transplant follow-up is another important factor for the development of recurrence of IgAN because the rate of recurrence increases as the time from transplant lengthens (5). It is unclear if recurrence is (8–10) or is not (11, 12) more frequent in transplants using related donors but this uncertainty does not preclude consideration of living donation in IgAN.
Recurrent glomerulonephritis is a significant cause of graft loss in transplant patients. Largest registry studies of Australia and New Zealand reported that IgAN recurrence was a significant cause of graft loss, third only to chronic allograft nephropathy and death with graft function. At 10 years the rate of graft loss for IgAN was similar to that of other forms of glomerulonephritis and to those of other causes of ESRD (13, 14). Outcomes after 10 years have been insufficiently studied in registry studies to draw firm conclusions, although results of a recent European Registry analysis (15) and some cohort studies suggested increasing graft loss after 10 years (16, 17).
IgA Nephropathy in the Native Kidney
Among primary chronic glomerular diseases, IgA nephropathy (IgAN) is the most prevalent worldwide (18). The clinical presentation is highly heterogeneous ranging from macroscopic hematuria with or without acute renal dysfunction during an infective episode and microscopic hematuria, isolated, or associated with proteinuria and hypertension. The diagnosis of certainty requires a renal biopsy, which shows the presence of dominant or codominant diffuse mesangial deposition of IgA which, in most cases, are aberrantly glycosylated. The mesangial IgA is exclusively of the IgA1 subclass and is deficient in galactose (19).
The pathogenesis of the disease is not completely clarified. Recent genome-wide association studies have identified multiple susceptibility loci for IgAN implicating independent defects in adaptive and innate immunity, and alternative complement pathways that potentially influence the different pathogenetic steps of the disease (20). By combining genetic and biochemical data, at least four processes seem to contribute to the development of the disease. Based on the available knowledge, there is in IgAN a primary, inherited defect that leads to preferential production of IgA1 with galactose-deficient O-glycans in the hinge-region (21). In the presence of inheritance of permissive MHC haplotypes, IgA1 deficient in galactose elicits the production of antiglycan autoantibodies, that lead to the formation and subsequent glomerular deposition of immune complexes. In particular IgA based activation of alternative complement pathway play a critical role in the IgAN pathogenesis and C3 is frequently involved in the formation of circulating immune deposits inducing mesangial stress, podocyte damages (22), and progressive deterioration of kidney function (23). On this basis IgAN is classified as an autoimmune disease (24). Recent attempts to characterize mediators of this response have focused on facilitators of B-cell differentiation and proliferation (25). The B cell activation factor of TNF family (BAFF) and a proliferation-inducing ligand (APRIL) has been indicated as modulating factors of B cell in the IgA pathogenesis by reducing both IgA serum levels and IgA glomerular deposition. These molecules may represent intriguing therapeutic targets for new IgAN treatments (26).
The disease generally runs an indolent course with a 10-year renal survival rate of about 90% among adults (27) and children (28) with normal renal function at diagnosis. However, 20–30% of patients develop end stage renal disease (ESRD) after 20 years or more follow-up (29), and need chronic dialysis or renal transplantation.
Proteinuria of at least 1 g/day, decreased estimated glomerular filtration rate (eGFR) at diagnosis and uncontrolled arterial hypertension are the clinical risk factors for the progression to ESRD (30). The Oxford classification of histological features of IgAN in the native kidney, that is based on the semiquantitative score of four histological features (mesangial hypercellularity, segmental glomerulosclerosis, endocapillary hypercellularity, and tubular atrophy/interstitial fibrosis), was found to be associated with increased risk of eGFR loss independent of clinical variables (31).
Histological Features of IgAN Recurrence in Kidney Transplant
Biopsy is mandatory not only to diagnose the disease in the native kidney, but also to identify and characterize graft recurrence of IgAN in the kidney graft. For this reason, the biopsy policies of the different centers and the techniques of histological evaluation have an important role in the definition of presence, frequency, and type of recurrence. Recurrence can be histological only, characterized by mesangial IgA with or without mesangial proliferation in the absence or presence of mild clinical manifestations. Ortiz et al. (32) evaluated the incidence of IgAN recurrence through protocol biopsies in 65 patients and found that the histological recurrence of IgAN can be recognized in almost one-third of patients within 2 years from transplantation. These results confirm those of a previous study with protocol biopsies that reported a 53% recurrence rate in 32 IgAN transplanted patients. Most of these patients did not have clinical signs of recurrence (5). The clinical value and the outcome of silent recurrent IgA deposits is not completely clarified. In some cases the disease progressed to overt clinical IgAN recurrence, (33) in others, IgA deposits disappeared in subsequent biopsies (34). The possibility of disappearance of IgA deposits from the kidney was also demonstrated in repeated renal biopsies of native IgAN (35). The demonstration that some apparently normal donors (living or deceased) may have latent IgA deposits in the kidney, raises the possibility that some histological recurrence can have such origin (36). Actually, when allografts with latent mesangial IgA deposits were transplanted in non IgA patients, the IgA was rapidly cleared by the recipients as demonstrated in follow-up biopsies (37). The transformation of the histological recurrence in clinical recurrence could be mediated by the activation of accessory factors such as activation of complement and cytokines production (38). However, based on the few available data about the clinical value of “histological” recurrence and the lack of an effective therapy, protocol biopsies in renal transplant patients with IgAN are not recommended unless steroid withdrawal is considered. The histological findings recorded at graft biopsy performed for clinical reasons, are not different from those of the original disease. In graft biopsy the diagnosis can be complicated by the simultaneous presence of other glomerular or vascular lesions secondary to acute or chronic graft rejections. In these cases, not only light microscopy and immunofluorescence, but also electron microscopy is needed to clearly define the possible association of two different diseases. In addition to mesangial IgA immunodeposits at immunofluorescence, mesangial proliferative glomerulonephritis is the typical histological pattern at light microscopy in IgAN recurrence with, in a minority of cases, features of glomerular cellular crescents. In a cohort of 71 IgAN transplanted patients, cellular or fibrocellular crescents were demonstrated in 14.1% of graft biopsies and were associated with a higher degree of interstitial inflammation and with a significant worse graft survival (39).
Some studies suggest that, the Oxford classification of histological features of IgAN in the native kidney, (31) applied to biopsies of recurrent IgAN has prognostic value for graft failure (40, 41). Based on these results the evaluation of the Oxford classification score, should be performed in all cases of IgAN recurrence.
Clinical Manifestations of IgAN Recurrence in Kidney Transplant
In the majority of studies the IgAN recurrence is diagnosed in graft biopsies performed for clinical reasons. The clinical presentation and the outcome of recurrences is extremely variable. Hematuria, the hallmark of IgAN in the native kidney, is not a reliable manifestation in recurrence as it was not present in 64% of cases diagnosed on protocol biopsies (32). Even in biopsies performed for clinical reasons hematuria is not the rule. In our cohort of 190 IgAN transplanted patients, the 43 recurrences presented with isolated microscopic haematuria in 5, isolated proteinuria in 8, microscopic haematuria and proteinuria in 12, isolated increase in plasma creatinine in 4, increase in plasma creatinine associated with haematuria or haematuria and proteinuria in the other 13 cases. In the four patients with an isolated increase in serum creatinine proteinuria and haematuria developed later, instead in seven patients all the urinary abnormalities regressed during the follow-up (17). Altogether in about one quarter of our patients, microscopic haematuria, the hallmark of IgAN in the native kidney, was not present at diagnosis of recurrences. This underlines that graft biopsy is essential to ensure the correct diagnosis.
Incidence of IgAN Recurrence in Kidney Transplant
The reported incidence of IgAN recurrence in biopsies performed for clinical reasons is around 30% but with a range of 9–53% among the different series if we consider protocol and clinical biopsies (Table 1). This large discrepancy can be attributed to several reasons in addition to the above reported different biopsy policies and techniques of histological evaluation in the different centers. The different racial and geographical distributions of IgAN may influence the rate of recurrence. The presence of IgA deposits in donated kidneys, frequently observed in Japanese series (36) was hypothesized to increase the probability of recurrence (47). The rate of recurrence can be underestimated if all patients who receive a renal transplant do not have a histological diagnosis of the original disease, or if the follow-up after transplant is too short. Recurrence rate reported in the ANZDATA registry for IgAN at 5 and at 10 years were, respectively 5.4% (4.3–6.5) and 10.8% (9.2–12.5%) (4). These data suggest that, recurrence of IgAN is apparently a time dependent event; the longer the follow-up, the higher the probability of recurrence. The incidence of IgAN recurrence can be underestimated if all patients with deterioration of renal function or with proteinuria are not submitted to graft biopsy. In the absence of graft biopsy, it is possible that some graft losses classified as chronic allograft nephropathy could be cases of unrecognized recurrence of IgAN (13).
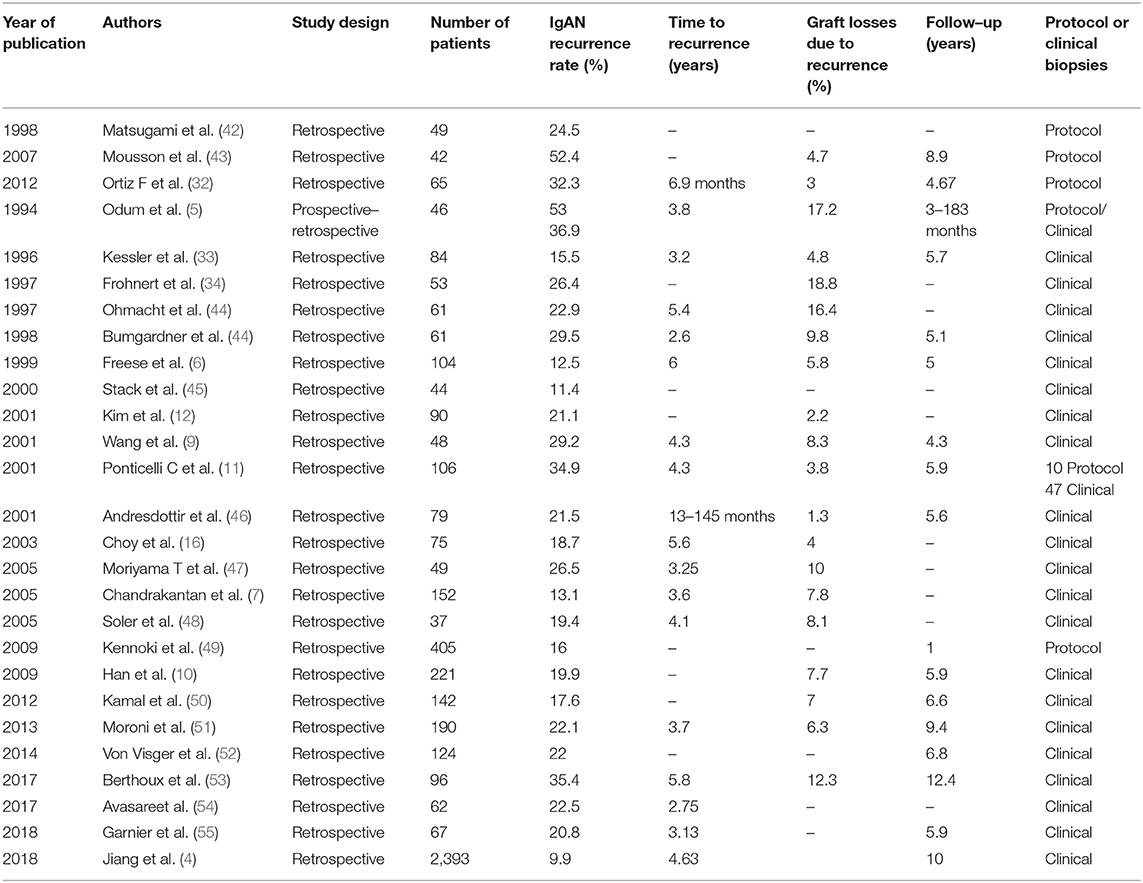
Table 1. Main studies on IgA nephropathy recurrence.
The rate of graft loss due to recurrence is reported to range from 1.3 (46) to 17% (5). However, the attribution of graft loss to the recurrence is not easy due to the possible presence of concomitant lesions due to acute or chronic graft rejections or to calcineurin inhibitors toxicity. This is particularly true if graft biopsy is not available close to the graft function deterioration (56).
Predictors of IgAN Recurrence in Kidney Transplant
Analysis of risk factors for IgAN recurrence have not provided consistent results. Young age at renal transplantation, male gender, and rapidly progressive course of the original disease before transplantation were associated with a higher risk of recurrence in some studies (10, 11, 13, 57). Avesare et al. (54) reevaluated the clinical and biopsy features of native kidney in 62 IgAN patients who received a transplant at Columbia University Medical Center from 2001 to 2012. They found that younger age at onset of IgAN and greater burden of crescents on native biopsy predicted recurrence after transplant.
Garnier et al. (55) found that serum IgA levels 6 months post-transplant was a risk factor of IgAN recurrence, independently of age, and serum creatinine. This was particularly true in patients who had serum IgA levels above 222.5 mg/dL at month 6 post-transplant.
Berthoux et al. (53) tested serum autoantibodies specific for galactose deficient-IgA1 at time of transplant or at time of native-kidney diagnosis in 96 first renal transplant recipients with IgAN. This study demonstrated that normalized serum levels of galactose deficient -IgA1–specific IgG autoantibody was an independent risk factor for recurrence of the disease in the allograft. This was particularly true for the earlier recurrences: 75% of events occurring before 8.79 years after transplantation (53).
Another unsolved question is whether living related donor kidneys have a higher risk of recurrence than kidneys from non-related donors. Some studies have failed to detect a significant difference (7, 11, 12, 34, 58) while others noted more frequent recurrences in grafts from living related donors (6, 9, 10). A review of the Australia-New Zealand registry data reported that IgAN recurrence was significantly more frequent in zero HLA mismatched living donor grafts (59). However, these results should be interpreted with caution because several details are lacking in retrospective reviews of registry data.
The risk of recurrence in the second graft in glomerulonephritis patients who lost the first graft for recurrence was investigated in 7,236 patients of the ANZDATA transplant registry. No increased risk of further recurrence in a subsequent graft was demonstrated for IgAN patients (4). This result is in contrast with previous small reports which suggested an increased risk of recurrences in patients with IgAN who lost the first graft for recurrence (6, 44, 60)
Current immunosuppressive agents used in transplantation do not seem to reduce IgAN recurrence in the allograft. Retrospective data from a single center suggests that induction therapy with antithymocyte globulin prevents the development of IgAN recurrence (57). Von Visger et al reported a significantly higher rate of IgA recurrence in patients maintained on steroid-free immunosuppression in comparison to those who received steroid-based immunosuppression (52).
Patient and Renal Survival of Kidney Transplant in IgAN Patients
Outcome of patients and graft survival in IgAN can be obtained from Registry analysis and from single centers observational studies. In comparison to single center studies, Registry analysis have the advantage of reporting data on a high number of patients but, some outcomes, such as causes of allograft failure, and incidence of recurrence are not accurately measured or are underestimated due to the different policies of the included centers. Single center retrospective studies provide more detailed information on different aspects of the disease in IgA transplanted patients but have low power in predicting the outcome.
The survival of transplanted patients with IgAN seems to be comparable or slightly better with that of recipients with other renal diseases both in Registry analysis and in single center studies. Among 32,131 patients with glomerulonephritis transplanted in the United States between 1996 and 2011, patients with IgAN had the lowest mortality rates (10% mortality at 10 years) in comparison to other glomerulonephritis forms and a slightly better survival than that of transplanted patients with adult polycystic kidney disease (APKD) (61). UK Renal Registry data, that analyzed patient survival in 2,975 incident patients with primary glomerulonephritis in comparison to 1,775 transplanted APKD patients who received a renal transplant between 1997 and 2009, reported unadjusted 10-year patient survival of 80.7% for APKD and 85.6% for IgAN (62).
Instead, the results of graft survival in patients with IgAN have been differently estimated across different countries and populations. The UNOS/OPTN database, in patients transplanted between 1999 and 2008, reported, in patients stratified for donor type (living vs. deceased) that at multivariable regression analysis the adjusted HR for death-censored allograft survival was not significantly different between IgAN and non-IgAN patients (63). Data from the European ERA-EDTA registry reported that the risk of death-adjusted graft failure for IgAN patients was not different from that of APKD until 10 years after transplant, thereafter the risk of graft loss was greater in IgAN (15). In addition, this study demonstrated that living related transplants in IgAN patients had lower risk of death-adjusted graft failure compared with deceased related transplants. The same lower death-adjusted graft survival of IgAN patients in comparison to APKD was reported by a largest study of transplanted patients in the United States (61).
The results concerning graft survival of IgAN patients reported by the single center studies are equally contrasting and depend partly on the length of the observation.
Some investigators reported a more favorable graft survival in IgAN patients than in other transplant recipients (64, 65), but other authors found similar results in an IgAN group than in non-IgAN transplant patients (48, 50, 58, 66). In particular, during the first 5 years after transplantation allograft survival for primary IgAN patients seems to be better than that of recipients with other primary renal diseases (12, 46, 64, 66, 67). Based on these short-term results, the recurrence of IgAN was considered to have little or no impact on graft function or on patient outcome (5, 68). At 10 years, graft survival of IgAN patients became comparable to that of recipients with other renal diseases (11, 12).
Choy et al. (16) found that the graft survival of up to 10 years was worse in IgAN patients than in controls, the two survival curves crossover at around 12 years. Our results are in agreement with actuarial death censored graft survival rates at 15 years of 62.6% in IgAN patients significantly worse than the 72.4% in the control group. In our cohort, the difference between the two survival curves become significant after the 15th year. When we separately evaluated the outcome of patients with and without recurrence we found that death censored graft survival at 15 years was 51.2% in the recurrent patients and significantly better (68.3%) in the non-recurrent recipients. Finally, graft survival in non-recurrent patients was not different from that of controls (17). The worst graft survival in the long-term of recurrent in comparison to non-recurrent IgAN patients was confirmed both in the recent report of the ANZDATA Registry (4) and by a retrospective study in 221 Korean recipients. In this study around 50% of patients received a graft from living related donors. Ten-years graft survival was 61% in recurrent IgAN group vs. 85.1% in non-recurrent patients (10).
It is well-known, that recurrence of glomerulonephritis is the third most frequent cause of allograft loss at 10 years, after chronic rejection and death with a functioning graft (13, 69). Based on these recent results, it seems that also for IgAN, the graft recurrence represents a substantial risk factor for graft failure in the very long-term as hypothesized by Ponticelli and Glassock (70). The introduction of new and more effective immunosuppressive agents has reduced graft loss by decreasing the incidence of acute rejection and of interstitial fibrosis and tubular atrophy. In this scenario, the recurrence of glomerulonephritis became progressively more frequent and can be a significant cause of graft loss in clinical practice. Mulay et al. reported that, after adjusting for important covariates, the use of cyclosporine, tacrolimus, azathioprine, mycophenolate mofetil, sirolimus, or prednisone does not prevent graft failure due to recurrent glomerulonephritis, including IgAN. However, any change in immunosuppression during follow-up was independently associated with graft loss due to recurrence (71).
Probably, old and short-term studies failed to detect a clinical impact of recurrent disease because, it is rare that the function of a graft with IgAN recurrence deteriorates during the first years after transplantation (67).
Treatment of Graft Recurrences of IgAN Patients
No universally accepted guidelines for the treatment of recurrence of IgAN in renal transplant are currently available. The goal of the therapy should be to prevent recurrence of IgAN.
Clayton et al. (14) suggested that steroid withdrawal may increase graft loss risk because of recurrence of IgAN. These results were confirmed in two subsequent studies (72, 73). In a retrospective analysis of the UNOS/OPTN database that included 9,690 IgAN adults who received their first kidney transplant between 2000 and 2014, early steroid-withdrawal was associated with an increased risk of recurrence at multivariate analysis (72).
At present treatment should aim to reduce proteinuria, to optimize blood pressure and to reduce inflammation as suggested by the KDIGO Transplant guidelines (74). The institution of good supportive therapy in particular the use of angiotensin converting enzyme inhibitors or angiotensin II receptor blocker in patients with proteinuria higher than 0.5 g/day is recommended based on good results reported in some studies (75, 76). Careful blood pressure control, particularly in patients with proteinuria > than 1 g/day, seems to be important to preserve graft function. However, it is important to consider that the use of these drugs in renal transplant may cause significant decreases in glomerular filtration rate and hematocrit (77). Studies from Japan report favorable outcomes after tonsillectomy in patients with recurrent IgAN (49, 78, 79) but these results need to be confirmed in different ethnicities. In the few cases of recurrent IgAN with rapid progressive renal insufficiency and crescents at biopsy, a rescue treatment with high-dose corticosteroids with cyclophosphamide, and or plasmapheresis may be attempted, although the results are usually poor. A promising therapeutic option is represented by drugs which target directly the intestinal mucosa, such as budesonide. Fellström et al. reported a reduction of proteinuria and a stabilization of renal function after budesonide administration in IgAN patients, suggesting a possible role of this drug also in patients with IgAN recurrence after kidney transplant (80).
Conclusions
Despite the high rate of recurrence and its potential negative impact on graft survival, renal transplant is the best choice for patients with ESRD secondary to IgAN. In our experience, recurrence of IgAN significantly reduced from 1981 to 2010 and in particular, recurrences occurred less frequently in transplants performed during the decade 2000–2010 (17). These results and the apparent reduction in graft loss from recurrent IgAN reported by Mulay et al. (71) and by Clayton et al. (14) in recent years may portend a progressive improvement of prognosis of renal transplant in IgAN patients in the near future. Better understanding of pathogenesis of the disease may enable more “specific” therapy. A large prospective multicenter randomized controlled trial with a long follow-up to evaluate interventions for recurrent IgA would be welcome and of importance in helping clinicians and patients.
Author Contributions
GM, MB, GF, FT, and PM conceived the article contents, prepared the manuscript, and endorsed the final draft submitted.
Conflict of Interest Statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
References
1. Schena FP. Epidemiology of end-stage renal disease: international comparisons of renal replacement therapy. Kidney Int. (2000) 57:S39–45. doi: 10.1046/j.1523-1755.2000.07407.x
2. ANZDATA Registry. Chapter 1: Incidence of End Stage Kidney Disease. The 37th Annual ANZDATA Report Australia and New Zealand Dialysis and Transplant Registry Adelaide, South Australia (2014).
3. US Renal Data System (USRDS). Annual Data Report: Atlas of Chronic Kidney Disease and End Stage Renal Disease in the United States. Bethesda, MD: National Institute of Health, National Institute of Diabetes and Digestive and Kidney Diseases (2013).
4. Jiang SH, Kennard AL, Walters GD. Recurrent glomerulonephritis following renal transplantation and impact on graft survival. BMC Nephrol. (2018) 19:344. doi: 10.1186/s12882-018-1135-7
5. Odum J, Peh CA, Clarkson AR, Bannister KM, Seymour AE, Gillis D, et al. Recurrent mesangial IgA nephritis following renal transplantation. Nephrol Dial Transplant. (1994) 9:309–12.
6. Freese P, Svalander C, Nordén G, Nyberg G. Clinical risk factors for recurrence of IgA nephropathy. Clin Transplant. (1999) 13:313–7. doi: 10.1034/j.1399-0012.1999.130406.x
7. Chandrakantan A, Ratanapanichkich P, Said M, Barker CV, Julian BA. Recurrent IgA nephropathy after renal transplantation despite immunosuppressive regimens with mycophenolate mofetil. Nephrol Dial Transplant. (2005) 20:1214–21. doi: 10.1093/ndt/gfh773
8. Andresdottir MB, Haasnoot GW, Doxiadis II, Persijn GG, Claas FH. Exclusive characteristics of graft survival and risk factors in recipients with immunoglobulin a nephropathy: a retrospective analysis of registry data. Transplantation. (2005) 80:1012–8. doi: 10.1097/01.tp.0000179150.84803.56
9. Wang AY, Lai FM, Yu AW, Lam PK, Chow KM, Choi PC, et al. Recurrent IgA nephropathy in renal transplant allografts. Kidney Dis. (2001) 38:588–96. doi: 10.1053/ajkd.2001.26885
10. Han SS, Huh W, Park SK, Ahn C, Han JS, Kim S, et al. Impact of recurrent disease and chronic allograft nephropathy on the long-term allograft outcome in patients with IgA nephropathy. Transpl Int. (2010) 23:169–75. doi: 10.1111/j.1432-2277.2009.00966.x
11. Ponticelli C, Traversi L, Feliciani A, Cesana BM, Banfi G, Tarantino A. Kidney transplantation in patients with IgA mesangial glomerulonephritis. Kidney Int. (2001) 60:1948–54. doi: 10.1046/j.1523-1755.2001.00006.x
12. Kim YS, Moon JI, Jeong HJ, Kim MS, Kim SI, Choi KH, et al. Live donor renal allograft in end-stage renal failure patients from immunoglobulin a nephropathy. Transplantation. (2001) 71:233–8. doi: 10.1097/00007890-200101270-00011
13. Briganti EM, Russ GR, McNeil JJ, Atkins RC, Chadban SJ. Risk of renal allograft loss from recurrent glomerulonephritis. N Engl J Med. (2002) 347:103–9. doi: 10.1056/NEJMoa013036
14. Clayton P, McDonald S, Chadban S. Steroids and recurrent IgA nephropathy after kidney transplantation. Am J Transplant. (2011) 11:1645–9. doi: 10.1111/j.1600-6143.2011.03667.x
15. Pippias M, Stel VS, Aresté-Fosalba N, Couchoud C, Fernandez-Fresnedo G, Finne P, et al. Long-term kidney transplant outcomes in primary glomerulonephritis: analysis from the ERA-EDTA registry. Transplantation. (2016) 100:1955–62. doi: 10.1097/TP.0000000000000962
16. Choy BY, Chan TM, Lo SK, Lo WK, Lai KN. Renal transplantation in patients with primary immunoglobulin A nephropathy. Nephrol Dial Transplant. (2003) 18:2399–404. doi: 10.1093/ndt/gfg373
17. Moroni G, Longhi S, Quaglini S, Gallelli B, Banfi G, Montagnino G, et al. The long-term outcome of renal transplantation of IgA nephropathy and the impact of recurrence on graft survival. Nephrol Dial Transplant. (2013) 28:1305–14. doi: 10.1093/ndt/gfs472
18. Donadio JV, Grande JP. IgA nephropathy. N Engl J Med. (2002) 347:738–48. doi: 10.1056/NEJMra020109
19. Wyatt RJ, Julian BA. IgA nephropathy. N Engl J Med. (2013) 368:2402–14. doi: 10.1056/NEJMra1206793
20. Gharavi AG, Kiryluk K, Choi M, Hou P, Xie J, Sanna-Cherchi S, et al. Genome-wide association study identifies susceptibility loci for IgA nephropathy. Nat Genet. (2011) 43:321–7. doi: 10.1038/ng.787
21. Moldoveanu Z, Wyatt RJ, Lee J, Tomana M, Julian BA, Mestecky J, et al. Patients with IgA nephropathy have increased serum galactose-deficient IgA1 levels. Kidney Int. (2007) 71:1148–54. doi: 10.1038/sj.ki.5002185
22. Suzuki H, Kiryluk K, Novak J, Moldoveanu Z, Herr AB, Renfrow MB, et al. The pathophysiology of IgA nephropathy. J Am Soc Nephrol. (2011) 22:1795–803. doi: 10.1681/ASN.2011050464
23. Kiryluk K, Novak J, Gharavi AG. Pathogenesis of immunoglobulin A nephropathy: recent insight from genetic studies. Annu Rev Med. (2013) 64:339–56. doi: 10.1146/annurev-med-041811-142014
24. Suzuki H, Fan R, Zhang Z, Brown R, Hall S, Julian BA, et al. Aberrantly glycosylated IgA1 in IgA nephropathy patients is recognized by IgG antibodies with restricted heterogeneity. J Clin Invest. (2009). 119:1668–77. doi: 10.1172/JCI38468
25. Penfold RS, Prendecki M, McAdoo S, Tam FW. Primary IgA nephropathy: current challenges and future prospects. Int J Nephrol Renovasc Dis. (2018) 12:137–48. doi: 10.2147/IJNRD.S129227
26. Wu MY, Chen CS, Yiang GT, Cheng PW, Chen YL, Chiu HC, et al. The emerging role of pathogenesis of IgA nephropathy. J Clin Med. (2018) 20. doi: 10.3390/jcm7080225
27. Lv J, Zhang H, Zhou Y, Li G, Zou W, Wang H. Natural history of immunoglobulin A nephropathy and predictive factors of prognosis: a long-term follow up of 204 cases in China. Nephrology. (2008) 13:242–6. doi: 10.1111/j.1440-1797.2007.00898.x
28. Ronkainen J, Ala-Houhala M, AutioHarmainen H, Jahnukainen T, Koskimies O, Merenmies J, et al. Long-term outcome 19 years after childhood IgA nephritis: a retrospective cohort study. Pediatr Nephrol. (2006) 21:1266–73. doi: 10.1007/s00467-006-0163-x
29. Berthoux F, Mohey H, Laurent B, Mariat C, Afiani A, Thibaudin L. Predicting the risk for dialysis or death in IgA nephropathy. J Am Soc Nephrol. (2011) 22:752–61. doi: 10.1681/ASN.2010040355
30. Barbour SJ, Reich HN. Risk stratification of patients with IgA nephropathy. Am J Kidney Dis. (2012) 59:865–73. doi: 10.1053/j.ajkd.2012.02.326
31. Working Group of the International IgA Nephropathy Network and the Renal Pathology Society, Roberts IS, Cook HT, Troyanov S, Alpers CE, Amore A, et al. The Oxford classification of IgA nephropathy: pathology definitions, correlations, and reproducibility. Kidney Int. (2009) 76:546–56. doi: 10.1038/ki.2009.168
32. Ortiz F, Gelpi R, Koskinen P, Manonelles A, Räisänen-Sokolowski A, Carrera M, et al. IgA nephropathy recurs early in the graft when assessed by protocol biopsy. Nephrol Dial Transplant. (2012) 27:2553–8. doi: 10.1093/ndt/gfr664
33. Kessler M, Hiesse C, Hestin D, Mayeux D, Boubenider K, Charpentier B. Recurrence of immunoglobulin A nephropathy after renal transplantation in the cyclosporine era. Am J Kidney Dis. (1996) 28:99–104. doi: 10.1016/S0272-6386(96)90137-7
34. Frohnert PP, Donadio JVJr, Velosa JA, Holley KE, Sterioff S. The fate of renal transplants in patients with IgA nephropathy. Clin Transplant. (1997) 11:127–33.
35. Hotta O, Furuta T, Chiba S, Tomioka S, Taguma Y. Regression of IgA nephropathy: a repeat biopsy study. Am J Kidney Dis. (2002) 39:493–502. doi: 10.1053/ajkd.2002.31399
36. Suzuki K, Honda K, Tanabe K, Toma H, Nihei H, Yamaguchi Y. Incidence of latent mesangial IgA deposition in renal allograft donors in Japan. Kidney Int. (2003) 63:2286–94. doi: 10.1046/j.1523-1755.63.6s.2.x
37. Silva FG, Chander P, Pirani CL, Hardy MA. Disappearance of glomerular mesangial IgA deposits after renal allograft transplantation. Transplant. (1982) 33:241–6. doi: 10.1097/00007890-198202000-00027
38. Coppo R, Feehally J, Glassock RJ. IgA nephropathy at two score and one. Kidney Int. (2010) 77:181–6. doi: 10.1038/ki.2009.427
39. Jeong HJ, Kim YS, Kwon KH, Kim SI, Kim MS, Choi KH, et al. Glomerular crescents are responsible for chronic graft dysfunction in post-transplant IgA nephropathy. Pathol Int. (2004) 54:837–42. doi: 10.1111/j.1440-1827.2004.01751.x
40. Trimarchi H, Barratt J, Cattran DC, Cook HT, Coppo R, Haas M, et al. IgAN classification working group of the international IgA nephropathy network and the renal pathology society; conference participants. Oxford classification of IgA nephropathy: an update from the IgA nephropathy classification working group. Kidney Int. (2017) 91:1014–21. doi: 10.1016/j.kint.2017.02.003
41. Park S, Go H, Baek CH, Kim YH, Kim YC, et al. Clinical importance of the updated Oxford classification in allograft IgA nephropathy. Am J Transplant Apr. (2019). doi: 10.1111/ajt.15400. [Epub ahead of print].
42. Matsugami K, Naito T, Nitta K, Nihei H, Tanabe K, Toma H, et al. A clinicopathological study of recurrent IgA nephropathy following renal transplantation. Nihon Jinzo Gakkai Shi. (1998) 40:322–8.
43. Mousson C, Charon-Barra C, Funes de la Vega M, Tanter Y, Justrabo E, Martin L, et al. Recurrence of IgA nephropathy with crescents in kidney transplants. Transplant Proc. (2007) 39:2595–6. doi: 10.1016/j.transproceed.2007.08.025
44. Ohmacht C, Kliem V, Burg M, Nashan B, Schlitt HJ, Brunkhorst R, et al. Recurrent immunoglobulin a nephropathy after renal transplantation: a significant contributor to graft Loss1. Transplantation. (1997) 64:1493–6. doi: 10.1097/00007890-199711270-00024
45. Stack A, Campbell E, Browne O, Saran R, Dorman T, Donohoe J. Prevalence and predictors of recurrent IgA nephropathy following renal transplantation. Ir J Med Sci. (2000) 169:248–52. doi: 10.1007/BF03173525
46. Andresdottir MB, Hoitsma AJ, Assmann KJ, Wetzels JF. Favorable outcome of renal transplantation in patients with IgA nephropathy. Clin Nephrol. (2001) 56:279–88.
47. Moriyama T, Nitta K, Suzuki K, Honda K, Horita S, Uchida K, et al. Latent IgA deposition from donor kidney is the major risk factor for recurrent IgA nephropathy in renal transplantation. Clin Transpl. (2005) 19:41–8. doi: 10.1111/j.1399-0012.2005.00403.x
48. Soler MJ, Mir M, Rodriguez E, Orfila A, Munne A, Va'zquez S, et al. Recurrence of IgA nephropathy and Henoch–Schoenlein purpura after kidney transplantation: risk factors and graft survival. Transplant Proc. (2005) 37:3705–9. doi: 10.1016/j.transproceed.2005.09.172
49. Kennoki T, Ishida H, Yamaguchi Y, Tanabe K. Proteinuria-reducing effects of tonsillectomy alone in IgA nephropathy recurring after kidney transplantation. Transplantation. (2009) 88:935–41. doi: 10.1097/TP.0b013e3181b75374
50. Kamal A, Mousson C, Berthoux F, Ducloux D, Chalopin JM. Renal transplantation outcome in selected recipients with IgA nephropaty as native disease: a bicentric study. Ann Transplant. (2012). 17:45–51. doi: 10.12659/AOT.883457
51. Moroni G, Longhi S, Quaglini S, Rognoni C, Simonini P, Binda V, et al. The impact of recurrence of primary glomerulonephritis on renal allograft outcome. Clin Transplant. (2014) 28:368–76. doi: 10.1111/ctr.12322
52. Von Visger JR, Gunay Y, Andreoni KA, Bhatt UY, Nori US, Pesavento TE, et al. The risk of recurrent IgA nephropathy in asteroid-free protocol and other modifying immunosuppression. Clin Transpl. (2014). 28:845–54. doi: 10.1111/ctr.12389
53. Berthoux F, Suzuki H, Mohey H, Maillard N, Mariat C, Novak J, et al. Prognostic value of serum biomarkers of autoimmunity for recurrence of IgA nephropathy after kidney transplantation. J Am Soc Nephrol. (2017) 28:1943–50. doi: 10.1681/ASN.2016060670
54. Avasare RS, Rosenstiel PE, Zaky ZS, Tsapepas DS, Appel GB, Markowitz GS, et al. Predicting post-transplant recurrence of IgA nephropathy: the importance of crescents. Am J Nephrol. (2017) 45:99–106. doi: 10.1159/000453081
55. Garnier AS, Duveau A, Demiselle J, Croué A, Subra JF, Sayegh J, et al. Early post-transplant serum IgA level is associated with IgA nephropathy recurrence after kidney transplantation. PLoS ONE. (2018) 13:e0196101. doi: 10.1371/journal.pone.0196101
56. Floege J, Gröne HJ. Recurrent IgA nephropathy in the renal allograft: not a benign condition. Nephrol Dial Transplant. (2013) 28:1070–3. doi: 10.1093/ndt/gft077
57. Berthoux F, El Deeb S, Mariat C, Diconne E, Laurent B, Thibaudin L. Antithymocyte globulin (ATG) induction therapy and disease recurrence in renal transplant recipients with primary IgA nephropathy. Transplantation. (2008) 85:1505–7. doi: 10.1097/TP.0b013e3181705ad4
58. Bumgardner GL, Amend WC, Ascher NL, Vincenti FG. Single-center long-term results of renal transplantation for IgA nephropathy. Transplantation. (1998) 65:1053–60. doi: 10.1097/00007890-199804270-00008
59. McDonald SP, Russ GR. Recurrence of IgA nephropathy among renal allograft recipients from living donors is greater among those with zero HLA mismatches. Transplantation. (2006) 82:759–62. doi: 10.1097/01.tp.0000230131.66971.45
60. Briggs DJ, Jones E. Recurrence of glomerulonephritis following renal transplantation. Scientific advisory board of the Era-EDTA registry european renal association -european dialysis and transpant associaton. Nephrol Dial Tranplant. (1999) 14:564–5. doi: 10.1093/ndt/14.3.564
61. O'Shaughnessy MM, Liu S, Montez-Rath ME, Lenihan CR, Lafayette RA, Winkelmayer WC. Kidney transplantation outcomes across GN Subtypes in the United States. J Am Soc Nephrol. (2017). 28:632–44. doi: 10.1681/ASN.2016020126
62. Pruthi R, McClure M, Casula A, Roderick PJ, Fogarty D, Harbe RM, et al. Long-term graft outcomes and patient survival are lower posttransplant in patients with a primary renal diagnosis of glomerulonephritis. Kidney Int. (2016) 89:918–26. doi: 10.1016/j.kint.2015.11.022
63. Kadiyala A, Mathew AT, Sachdeva M, Sison CP, Shah HH, Fishbane S, et al. Outcomes following Kidney transplantation in IgA nephropathy: a UNOS/OPTN analysis. Clin Transplant. (2015) 29:911–9. doi: 10.1111/ctr.12594
64. Lim EC, Terasaki PI. Outcome of renal transplantation in different primary diseases. Clin Transpl. (1991) 1991:293–303.
65. Jeong HJ, Park SK, Cho YM, Kim MS, Kim YS, Choi J, et al. Progression of renal allograft histology after renal transplantation in recurrent and nonrecurrent immunoglobulin A nephropathy. Hum Pathol. (2008) 39:1511–8. doi: 10.1016/j.humpath.2008.03.003
66. Chacko B, George JT, Neelakantan N, Korula A, Chakko JK. Outcomes of renal transplantation in patients with immunoglobulin A nephropathy in India. J Postgrad Med. (2007) 53:92–5. doi: 10.4103/0022-3859.32207
67. Floege J. Recurrent IgA nephropathy after renal transplantation. Semin Nephrol. (2004) 24:287–91. doi: 10.1016/j.semnephrol.2004.01.008
68. Berger J. Recurrence of IgA nephropathy in renal allografts. Am J Kidney Dis. (1988) 12:371–2. doi: 10.1016/S0272-6386(88)80027-1
69. Golgert W, Appel G, Hariharan S. Recurrent glomerulonephritis and renal transplantation: an unsolved problem. Clin J Am Soc Nephrol. (2008) 3:800–7. doi: 10.2215/CJN.04050907
70. Ponticelli C, Glassock RJ. Posttransplant recurrence of primary glomerulonephritis. Clin J Am Soc Nephrol. (2010) 5:2363–72. doi: 10.2215/CJN.06720810
71. Mulay AV, van Walraven C, Knoll GA. Impact of immunosuppressive medication on the risk of renal allograft failure due to recurrent glomerulonephritis. Am J Transplant. (2009) 9:804–11. doi: 10.1111/j.1600-6143.2009.02554.x
72. Leeaphorn N, Garg N, Khankin EV, Cardarelli F, Pavlakis M. Recurrence of IgA nephropathy after kidney transplantation in steroid continuation versus early steroid-withdrawal regimens: a retrospective analysis of the UNOS/OPTN database. Transpl Int. (2018) 31:175–86. doi: 10.1111/tri.13075
73. Di Vico MC, Messina M, Fop F, Barreca A, Segoloni GP, Biancone L. Recurrent IgA nephropathy after renal transplantation and steroid withdrawal. Clin Transplant. (2018) 32:e13207. doi: 10.1111/ctr.13207
74. Kidney Disease. Improving Global Outcomes (KDIGO) Transplant Work Group. KDIGO clinical practice guideline for the care of kidney transplant recipients. 2009. Am J Transplant. (2009) 9:S1–155. doi: 10.1111/j.1600-6143.2009.02834.x
75. Oka K, Imai E, Moriyama T, Akagi Y, Ando A, Hori M, et al. A clinicopathological study of IgA nephropathy in renal transplant recipients: beneficial effect of angiotensin-converting enzyme inhibitor. Nephrol Dial transplant. (2000) 15:689–95. doi: 10.1093/ndt/15.5.689
76. Courtney AE, McNamee PT, Nelson WE, Maxwell AP. Does angiotensin blockade influence graft outcome in renal transplant recipients with IgA nephropathy? Nephrol Dial Transplant. (2006) 21:3550–4. doi: 10.1093/ndt/gfl506
77. Hiremath S, Fergusson D, Doucette S, Mulay AV, Knoll GA. Renin angiotensin system blockade in kidney transplantation: a systematic review of the evidence. Am J Transplant. (2007) 7:2350–60. doi: 10.1111/j.1600-6143.2007.01928.x
78. Hotta K, Fukasawa Y, Akimoto M, Tanabe T, Sasaki H, Fukuzawa N, et al. Tonsillectomy ameliorates histological damage of recurrent immunoglobulin A nephropathy after kidney transplantation. Nephrology. (2013) 18:808–12. doi: 10.1111/nep.12151
79. Ushigome H, Suzuki T, Fujiki M, Nobori S, Sakamoto S, Okamoto M, at al. Efficacy of tonsillectomy for patients with recurrence of IgA nephropathy after kidney transplantation. Clin Transplant. (2009) 23:17–22. doi: 10.1111/j.1399-0012.2009.01003.x
Keywords: IgA nephropathy, kidney transplant, proteinuria, humans, glomerulonephritis IgA, prognosis, therapy
Citation: Moroni G, Belingheri M, Frontini G, Tamborini F and Messa P (2019) Immunoglobulin A Nephropathy. Recurrence After Renal Transplantation. Front. Immunol. 10:1332. doi: 10.3389/fimmu.2019.01332
Received: 12 March 2019; Accepted: 28 May 2019;
Published: 19 June 2019.
Edited by:
Niels Olsen Saraiva Camara, University of São Paulo, BrazilReviewed by:
Viktoria Woronik, Fundação Faculdade de Medicina, BrazilLeonardo V. Riella, Brigham and Women's Hospital and Harvard Medical School, United States
Copyright © 2019 Moroni, Belingheri, Frontini, Tamborini and Messa. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Gabriella Moroni, Z2FicmllbGxhLm1vcm9uaSYjeDAwMDQwO3BvbGljbGluaWNvLm1pLml0