
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
OPINION article
Front. Immunol. , 16 November 2018
Sec. Multiple Sclerosis and Neuroimmunology
Volume 9 - 2018 | https://doi.org/10.3389/fimmu.2018.02652
This article is part of the Research Topic Neurotropism of Parasites and Immune Responses View all 8 articles
 Andrea Toledo1
Andrea Toledo1 Rocio Osorio1
Rocio Osorio1 Carlos Matus1Yazmin Martinez Lopez1Nancy Ramirez Cruz1Edda Sciutto2Gladis Fragoso2Antonio Arauz3
Carlos Matus1Yazmin Martinez Lopez1Nancy Ramirez Cruz1Edda Sciutto2Gladis Fragoso2Antonio Arauz3 Roger Carrillo-Mezo4
Roger Carrillo-Mezo4 Agnès Fleury1,5*
Agnès Fleury1,5*Neurocysticercosis (NCC) is the most common parasitic brain infection worldwide. NCC is a disease clearly associated with poverty and is endemic in most of the countries of Latin America, Africa, and Asia (1–3). Also, linked with migration, NCC is increasingly diagnosed in non-endemic countries (4, 5). In 2015, the World Health Organization identified T. solium as a leading cause of deaths from food-borne diseases, resulting in a considerable total of 2.8 million disability-adjusted life-years (DALYs) (6). It is caused by the establishment of the larval stage of Taenia solium (cysticerci) in the central nervous system. The main factors underlying the pathogeny of NCC are the location, number and stage of the parasite, the host genetic background and the host inflammatory reaction (7, 8). With respect to the latter, the intensity of the inflammation elicited by the parasite is clearly related to clinical severity (9). When parasites are located in the brain parenchyma, local inflammation promotes seizures, the most common neurological symptom in NCC patients (10). On the other hand, when parasites are located in the subarachnoid space, arachnoiditis and arteritis are frequently observed (11). Due to these potentially serious complications and to the severity of early symptoms (mainly intracranial hypertension, often requiring a ventriculoperitoneal shunt, VPS), extraparenchymal NCC (EP-NCC) is the most severe form of NCC (12).
Moreover, it should be noted that the intensity of the central inflammation is highly heterogeneous among patients, even for parasites located in the same cerebral area. Considering the cell count in the lumbar cerebrospinal fluid (CSF) as an indicator of neuroinflammation, 67% of EP-NCC patients exhibited 15–200 cell/mL; 24% presented an almost normal cell count, and around 9% of them had counts over 200 cells/mL (12). CSF protein levels are also variable in these EP-NCC patients, with 27.9% having a normal concentration (< 40 mg/dL), 60% exhibited increased levels (40–300 mg/dL), and 12.1% had very high concentrations, over 300 mg/dL (12).
The current treatment of NCC includes anthelminthic drugs (albendazole, ABZ, or praziquantel, PZQ) to destroy cysts, and corticosteroids (mainly dexamethasone and prednisone) to prevent complications from the exacerbated inflammatory response promoted by the parasite itself and by its destruction (13–16).
Corticosteroid treatment has been demonstrated to reduce seizure recurrence and accelerate the resolution of lesions in parenchymal NCC patients (17, 18) while reducing the frequency of VPS dysfunctions and improving the clinical outcome in patients with vasculitis associated to extraparenchymal parasites (19, 20). The dose and duration of corticosteroid treatment is practitioner-dependent, as randomized clinical trial evidences are scarce (16). However, it is generally admitted that corticosteroid treatment must be short and at doses relatively low when treating parenchymal NCC patients, and more prolonged with higher doses in cases of EP-NCC (21, 22).
The efficacy of anthelminthic therapy is variable. A clear clinic-radiological benefit is often recognized in parenchymal NCC patients, but its efficacy for EP-NCC is less immediate (11). The reasons underlying this difference are still not clear and multiple factors could be involved, like differences in parasite size, much larger in EP locations than in parenchymal ones.
We hypothesize that some central immune-inflammatory factors are required to act along with cysticidal drugs to maximize the efficiency of parasite destruction. Although other factors are also probably involved, immune-inflammatory factors could play a central role in the marked differences observed in the response to treatment among parasites located in different compartments, and in the heterogeneity of the response to treatment among patients with parasites located in the same compartment.
Indeed, parenchymal cysts are in an environment with abundance of resident immune-competent cells, while extraparenchymal ones are surrounded by CSF, a mostly acellular medium under normal conditions. Also, in swine NCC, it was demonstrated that the intensity of pericystic inflammation associated with PZQ treatment was significantly higher in parenchymal cysts than in subarachnoid ones (23). According to those reports, these differences would likely contribute to the known differences in treatment efficacy between parenchymal and subarachnoid NCC (23).
With respect to the heterogeneous response to treatment of parasites located in the same compartment, an association between the presence of proinflammatory mediators and response to treatment in EP-NCC patients was recently found (24). On the other hand, in swine NCC, ABZ alone was shown to be more effective than when combined with corticosteroids, especially in parenchymal cysts (25). Finally, in a recent study on naturally infected pigs, the administration of dexamethasone before and during PZQ treatment significantly reduced the damage to the cyst wall (26). The relevance of an exacerbated central inflammation in parasite damage might be favored by an increase in the permeability of the blood-brain barrier, favoring the influx of cysticidal drugs, as well as the arrival of peripheral inflammatory cells and mediators (27, 28).
Medical practitioners face a dual situation, where the inflammatory reaction contributes to treatment success but where its control, necessary to elude severe neurological complications, may reduce the efficacy of the cysticidal treatment.
Currently, the administration of corticosteroids to control neuroinflammation is highly recommended (16). However, it should be noted that the use of steroids could be beneficial for the parasite in several ways. Indeed, the well-known immunosuppression promoted by steroids could favor parasite survival. Moreover, steroids stimulate the expansion of regulatory T cells and the production of TGFβ, a molecule that can also promote the survival of the cysticerci (29). An additional direct effect of corticosteroids on parasites can also play a role in the resistance to treatment. In vitro studies on Taenia crassiceps (a worm closely related to T. solium) showed that corticosteroids improved its ability to synthesize androgens and estrogens, enhancing its reproductive capacity (30).
This situation stressed the need for personalized therapies based on the intensity of the extremely heterogeneous central inflammatory reaction (Figure 1).
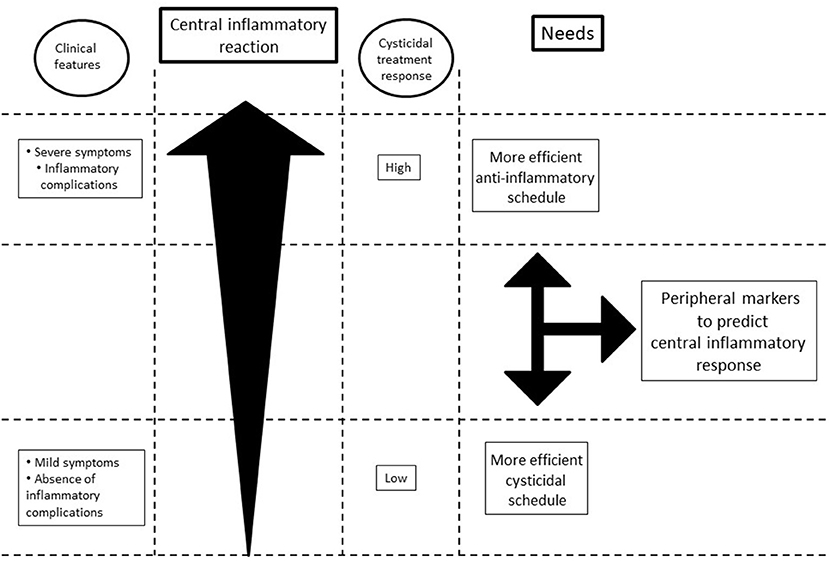
Figure 1. Schematic representation of the relationship among inflammation, symptomatology, and response to treatment.
Therefore, future research on the treatment of EP-NCC should consider the following issues: With respect to anti-inflammatory drugs, the patients who exhibited less inflammation could receive lower doses without risk of inflammatory complications, thus preserving the effectivity of cysticidal drugs. On the other hand, those patients who exhibited a higher inflammatory response would require either higher doses or more efficient/specific anti-inflammatory drugs to prevent complications.
With respect to cysticidal drugs, the patients who exhibited less inflammation should receive the therapeutic schedule of 30 mg/kg/day of ABZ for 10 days (31), with the possibility of extending or repeating the treatment in case of no-response. A combined ABZ-PZQ treatment has proved to be more efficient than single drug administration in patients with more than 2 parenchymal parasites (32), and this could be an option for patients lodging extraparenchymal parasites. Research on other cysticidal drugs should continue. On the other hand, patients with a higher inflammatory status will probably respond to the current ABZ treatment schedule (15 mg/kg/day for 10 days).
The challenge now is how to determine beforehand which patients belong to which group (higher/lower inflammation), to provide the most appropriate combined treatment (cysticidal + corticosteroid). In this context, finding sensitive and specific new peripheral biomarkers with predictive capacity on the magnitude of neuroinflammation during the cysticidal response is much needed. CSF cellularity is currently used to evaluate central inflammation, but unfortunately lumbar puncture is not accepted in all settings and could be contraindicated when hydrocephalus is associated. The use of new radiological tools to identify infiltrated inflammatory cells and mediators in the periphery could also be very useful in the future (33), as well as studies allowing us to clarify the role of genetic in the variable treatment responsiveness of patients, since it is likely a factor of major relevance (34–36).
Finding peripheral biomarkers reflecting the intensity of central inflammation is a crucial point to reduce the morbidity of NCC resulting from the lack of response to treatment and the occurrence of inflammatory complications.
AT, RO, CM, YM, and NR: made substantial contributions to conception and design, have been involved in drafting the manuscript, gave final approval of the version to be published, agreed to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved. ES, GF, AA, RC-M, and AF: made substantial contributions to conception and design, have been involved in drafting the manuscript and revising it critically for important intellectual content, gave final approval of the version to be published, agreed to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved.
This work was supported by the Consejo Nacional de Ciencia y Tecnología [grant number S0008-2015-1, 261153].
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
The authors thank Juan Francisco Rodriguez and Carolyn O'Meara for copyediting this manuscript.
ABZ, albendazole; CSF, cerebrospinal fluid; EP-NCC, extraparenchymal NCC; NCC, Neurocysticercosis; PZQ, Praziquantel; VPS, ventriculoperitoneal shunt.
1. Millogo A, Kongnyu Njamnshi A, Kabwa-PierreLuabeya M. Neurocysticercosis and epilepsy in sub-Saharan Africa. Brain Res Bull. (2018). doi: 10.1016/j.brainresbull.2018.08.011. [Epub ahead of print].
2. Wu HW, Ito A, Ai L, Zhou XN, Acosta LP, Lee Willingham A III. Cysticercosis/taeniasis endemicity in Southeast Asia: current status and control measures. Acta Trop. (2017) 165:121–32. doi: 10.1016/j.actatropica.2016.01.013
3. Fleury A, Sciutto E, de Aluja AS, Carpio A. Cysticercosis: a preventable, but embarrassing neglected disease still prevalent in non-developed countries. In: Sing A, editor. Zoonoses - Infections Affecting Humans and Animals. 1st ed. Netherlands: Springer (2015). p. 335–54.
4. Symeonidou I, Arsenopoulos K, Tzilves D, Soba B, Gabriël S, Papadopoulos E. Human taeniasis/cysticercosis: a potentially emerging parasitic disease in Europe. Ann Gastroenterol. (2018) 31:406–12. doi: 10.20524/aog.2018.0260
5. O'Neal SE, Flecker RH. Hospitalization frequency and charges for neurocysticercosis, United States, 2003–2012. Emerg Infect Dis. (2015) 21:969–76. doi: 10.3201/eid2106.141324
6. Torgerson PR, Devleesschauwer B, Praet N, Speybroeck N, Willingham AL, Kasuga F, et al. World Health Organization Estimates of the global and regional disease burden of 11 foodborne parasitic diseases, 2010: a data synthesis. PLoS Med. (2015) 12:e1001920. doi: 10.1371/journal.pmed.1001920.
7. Fleury A, Escobar A, Fragoso G, Sciutto E, Larralde C. Clinical heterogeneity of human neurocysticercosis results from complex interactions among parasite, host and environmental factors. Trans R Soc Trop Med Hyg. (2010) 104:243–50. doi: 10.1016/j.trstmh.2010.01.005.
8. Lachuriya G, Garg RK, Jain A, Malhotra HS, Singh AK, Jain B, et al. Toll-like receptor-4 polymorphisms and serum matrix metalloproteinase-9 in newly diagnosed patients with calcified neurocysticercosis and seizures. Medicine (2016) 95:e3288. doi: 10.1097/MD.0000000000003288.
9. Chavarría A, Fleury A, García E, Márquez C, Fragoso G, Sciutto E. Relationship between the clinical heterogeneity of neurocysticercosis and the immune-inflammatory profiles. Clin Immunol. (2005) 116:271–8. doi: 10.1016/j.clim.2005.04.008.
10. Kumar Garg R, Kumar Singh M, Misra S. Single-enhancing CT lesions in Indian patients with seizures: a review. Epilepsy Res. (2000) 38:91–104. doi: 10.1016/S0920-1211(99)00092-3
11. Fleury A, Carrillo-Mezo R, Flisser A, Sciutto E, Corona T. Subarachnoid basal neurocysticercosis: a focus on the most severe form of the disease. Expert Rev Anti Infect Ther. (2011) 9:123–33. doi: 10.1586/eri.10.150.
12. Marcin Sierra M, Arroyo M, Cadena Torres M, Ramírez Cruz N, García Hernández F, Taboada D, et al. Extraparenchymal neurocysticercosis: demographic, clinicoradiological, and inflammatory features. Plos Negl Trop Dis. (2017) 11: e0005646. doi: 10.1371/journal.pntd.0005646.
13. Bang OY, Heo JH, Choi SA, Kim DI. Large cerebral infarction during praziquantel therapy in neurocysticercosis. Stroke (1997) 28: 211–3
14. Nash TE, Mahanty S, Garcia HH, Cysticercosis Group in Peru. Corticosteroid use in neurocysticercosis. Expert Rev Neurother. (2013) 11:1175–83. doi: 10.1586/ern.11.86.
15. Mahanty S, Orrego MA, Mayta H, Marzal M, Cangalaya C, Paredes A, et al. Post-treatment vascular leakage and inflammatory responses around brain cysts in porcine neurocysticercosis. PLoS Negl Trop Dis. (2015) 9:e0003577. doi: 10.1371/journal.pntd.0003577.
16. White AC, Coyle CM, Rajshekhar V, Singh G, Hauser WA, Mohanty A, et al. Diagnosis and treatment of neurocysticercosis: 2017 clinical practice guidelines by the Infectious Diseases Society of America (IDSA) and the American Society of Tropical Medicine and Hygiene (ASTMH). Am J Trop Med Hyg. (2018) 98:945–66. doi: 10.4269/ajtmh.18-88751.
17. Cuello-García CA, Roldán-Benítez YM, Pérez-Gaxiola G, Villarreal-Careaga J. Corticosteroids for neurocysticercosis: a systematic review and meta-analysis of randomized controlled trials. Int J Infect Dis. (2013) 17:e583–92. doi: 10.1016/j.ijid.2012.12.010.
18. Garcia HH, Gonzales I, Lescano AG, Bustos JA, Pretell EJ, Saavedra H, et al. Enhanced steroid dosing reduces seizures during antiparasitic treatment for cysticercosis and early after. Epilepsia (2014) 55:1452–9. doi: 10.1111/epi.12739.
19. Suastegui Roman RA, Soto-Hernandez JL, Sotelo J. Effects of prednisone on ventriculoperitoneal shunt function in hydrocephalus secondary to cysticercosis: a preliminary study. J Neurosurg. (1996) 84:629–33. doi: 10.3171/jns.1996.84.4.0629.
20. Del Brutto OH. Cysticercosis and cerebrovascular disease: a review. J Neurol Neurosurg Psychiatry (1992) 55:252–4
21. Garcia HH, Nash TE, Del Brutto OH. Clinical symptoms, diagnosis, and treatment of neurocysticercosis. Lancet Neurol. (2014) 13:1202–15. doi: 10.1016/S1474-4422(14)70094-8.
22. Webb CM, White AC Jr. Update on the diagnosis and management of neurocysticercosis. Curr Infect Dis Rep. (2016) 18:44. doi: 10.1007/s11908-016-0547-4
23. Cangalaya C, Zimic M, Marzal M, González AE, Guerra-Giraldez C, Mahanty S, et al. Inflammation caused by praziquantel treatment depends on the location of the Taenia solium cysticercus in porcine neurocysticercosis. PLoS Negl Trop Dis. (2015) 9:e0004207. doi: 10.1371/journal.pntd.0004207.
24. Cárdenas G, Fragoso G, Rosetti M, Uribe-Figueroa L, Rangel-Escareño C, Saenz B, et al. Neurocysticercosis: the effectiveness of the cysticidal treatment could be influenced by the host immunity. Med Microbiol Immunol. (2014) 203:373–81. doi: 10.1007/s00430-014-0345-2.
25. Singh AK, Singh SK, Singh A, Gupta KK, Khatoon J, Prasad A, et al. Immune response to Taenia solium cysticerci after anti-parasitic therapy. Int J Parasitol. (2015) 45:749–59. doi: 10.1016/j.ijpara.2015.05.007.
26. Mahanty S, Orrego MA, Cangalaya C, Adrianzen MP, Arroyo G, Calcina J, et al. TNF-α blockade suppresses pericystic inflammation following anthelmintic treatment in porcine neurocysticercosis. PLoS Negl Trop Dis. (2017) 11:e0006059. doi: 10.1371/journal.pntd.0006059.
27. Erickson MA, Dohi K, Banks WA. Neuroinflammation: a common pathway in CNS diseases as mediated at the blood-brain barrier. Neuroimmunomodulation (2012) 19:121–30. doi: 10.1159/000330247.
28. Guerra-Giraldez C, Marzal M, Cangalaya C, Balboa D, Orrego MÁ, Paredes A, et al. Disruption of the blood-brain barrier in pigs naturally infected with Taenia solium, untreated and after anthelmintic treatment. Exp Parasitol. (2013) 134:443–6. doi: 10.1016/j.exppara.2013.05.005.
29. Adalid-Peralta L, Rosas G, Arce-Sillas A, Bobes RJ, Cárdenas G, Hernández M, et al. Effect of transforming growth factor-β upon taenia solium and Taenia crassiceps Cysticerci. Sci Rep. (2017) 7:12345. doi: 10.1038/s41598-017-12202-z.
30. Romano MC, Jiménez P, Miranda-Brito C, Valdez RA. Parasites and steroid hormones: corticosteroid and sex steroid synthesis, their role in the parasite physiology and development. Front Neurosci. (2015) 9:224. doi: 10.3389/fnins.2015.00224.
31. Gongora-Rivera F, Soto-Hernández JL, González Esquivel D, Cook HJ, Márquez-Caraveo C, Hernández Dávila R, et al. Albendazole trial at 15 or 30 mg/kg/day for subarachnoid and intraventricular cysticercosis. Neurology (2006) 66:436–8. doi: 10.1212/01.wnl.0000195887.63124.dc
32. Garcia HH, Lescano AG, Gonzales I, Bustos JA, Pretell EJ, Horton J, et al. Cysticidal efficacy of combined treatment with praziquantel and albendazole for parenchymal brain cysticercosis. Clin Infect Dis. (2016) 62:1375–9. doi: 10.1093/cid/ciw134.
33. Pacilio M, Lauri C, Prosperi D, Petitti A, Signore A. New SPECT and PET Radiopharmaceuticals for imaging inflammatory diseases: a meta-analysis of the Last 10 Years. Semin Nucl Med. (2018) 48:261–76. doi: 10.1053/j.semnuclmed.2017.12.004.
34. Pérez MG, Macchiaroli N, Lichtenstein G, Conti G, Asurmendi S, Milone DH, et al. microRNA analysis of Taenia crassiceps cysticerci under praziquantel treatment and genome-wide identification of Taenia solium miRNAs. Int J Parasitol. (2017) 47:643–53. doi: 10.1016/j.ijpara.2017.04.002.
35. Singh A, Prasad KN, Singh AK, Singh SK, Gupta KK, Paliwal VK, et al. Human Glutathione S-Transferase enzyme gene polymorphisms and their association with Neurocysticercosis. Mol Neurobiol. (2017) 54:2843–51. doi: 10.1007/s12035-016-9779-4
36. Fleury A, Alaez C, Dessein A, Rosetti M, Saenz B, Hernández M, et al. No association of IL2, IL4, IL6, TNF, and IFNG gene polymorphisms was found with Taenia solium human infection or neurocysticercosis severity in a family-based study. Hum Immunol. (2018) 79:578–82. doi: 10.1016/j.humimm.2018.04.011
Keywords: neurocysticercosis, Taenia solium, treatment, inflammation, parasite, Mexico
Citation: Toledo A, Osorio R, Matus C, Martinez Lopez Y, Ramirez Cruz N, Sciutto E, Fragoso G, Arauz A, Carrillo-Mezo R and Fleury A (2018) Human Extraparenchymal Neurocysticercosis: The Control of Inflammation Favors the Host…but Also the Parasite. Front. Immunol. 9:2652. doi: 10.3389/fimmu.2018.02652
Received: 14 August 2018; Accepted: 26 October 2018;
Published: 16 November 2018.
Edited by:
Miriam Postan, Consejo Nacional de Investigaciones Científicas y Técnicas (CONICET), ArgentinaReviewed by:
Amit Prasad, Indian Institute of Technology Mandi, IndiaCopyright © 2018 Toledo, Osorio, Matus, Martinez Lopez, Ramirez Cruz, Sciutto, Fragoso, Arauz, Carrillo-Mezo and Fleury. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Agnès Fleury, YWZsZXVyeUBiaW9tZWRpY2FzLnVuYW0ubXg=
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.