
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Endocrinol. , 27 September 2019
Sec. Thyroid Endocrinology
Volume 10 - 2019 | https://doi.org/10.3389/fendo.2019.00671
 Clément Bouvet1
Clément Bouvet1 Bertrand Barres1,2
Bertrand Barres1,2 Fabrice Kwiatkowski3
Fabrice Kwiatkowski3 Marie Batisse-Lignier4,5Meryem Chafai El Alaoui1Philippe Kauffmann6Florent Cachin1,2,7Igor Tauveron2,4,5
Marie Batisse-Lignier4,5Meryem Chafai El Alaoui1Philippe Kauffmann6Florent Cachin1,2,7Igor Tauveron2,4,5 Antony Kelly1
Antony Kelly1 Salwan Maqdasy2,4,5*
Salwan Maqdasy2,4,5*Introduction: Loco regional persistence or recurrence of differentiated thyroid cancer (DTC) is frequent despite initial thyroidectomy and radioactive iodine therapy (RAI). The aim of this study was to analyze the impact of a complementary adjuvant RAI (Ad-RAI) on disease recurrence following re-operation on patients with locally persistent or recurrent DTC.
Patients and Methods: A retrospective study of 85 patients with DTC was conducted. All patients were initially treated with total thyroidectomy and RAI, and re-operated for a locally persistent or recurrent disease. Propensity score was calculated to predict the impact of Ad-RAI on survival after reoperation, and to reduce the bias of the limited sample size and the prognostic tests.
Results: 49 (58%) patients were re-treated with Ad-RAI after re-operation while 36 (42%) were only followed up. Disease recurrence after re-treatment (re-operation ± Ad-RAI) was detected in 31 patients (36.5%). In multivariate analysis, age >55 years (HR: 3.9 [1.6; 9.5]; p < 0.00001) was the main poor prognostic factor for recurrence-free survival. Three parameters independently influenced the decision to administer ad-RAI: low number of previous RAI administrations, Nx before re-operation, and pTg > 30 μg/l. These parameters were incorporated in the Propensity score calculation. If ad-RAI tended to improve recurrence-free survival (median survival 17.4 vs. 10.9 months), adjustment using the Propensity score removed any difference between the groups (p = 0.54), confirming the limited value of ad-RAI.
Conclusion: In patients with locally persistent or recurrent DTC, age is the main independent prognostic factor. Adjuvant RAI does not improve recurrence-free survival of DTC patients.
Differentiated thyroid cancer (DTC) is the most frequent endocrine cancer. Despite the increased incidence of DTC in recent decades, disease progression is usually slow and 10-year survival is excellent (1, 2). Nevertheless, post-surgical loco regional disease persistence and recurrence are detected in about 20 and 30% of patients, respectively (3–5). These two conditions are defined by the presence of morphological anomalies, detected by imaging techniques (e.g., ultrasound, CT scan, PET-CT), and/or biological anomalies (e.g., persistently elevated thyroglobulin levels >1 μg/l under suppressed TSH and/or >10 μg/l after TSH stimulation) (6).
The prognostic value of re-operation in patients with locally persistent or recurrent disease has been demonstrated previously (7). According to the American Thyroid Association (ATA), re-operation is recommended for persistent or recurrent loco regional disease when the lesion exceeds 8–10 mm on the smallest diameter (6). For smaller lesions, active follow up is suggested (8). Thus, these recent modifications in the management of DTC support a less aggressive strategy, limiting the indications of re-operation and re-treatment with adjuvant radioactive iodine 131I (RAI) for more extensive disease. In a retrospective study on 45 patients, Yim et al. demonstrated that adjuvant RAI did not reduce thyroglobulin levels in 23 patients with persistent or recurrent disease, including distant metastases (9). Hirsch et al. analyzed 44 patients who were re-operated before re-treatment. In this group, 47% had a persistent disease despite re-treatment with RAI (10). Whether a treatment with complementary or adjuvant RAI after re-operation is useful or not remains a matter of debate, as no randomized controlled clinical trials have been conducted.
This study aims to identify the prognostic factors, including adjuvant RAI, that influence recurrence-free survival in patients re-operated for persistent or recurrent DTC following initial ablative management by surgery and RAI.
We have conducted a retrospective study in the Department of Nuclear Medicine at the Jean Perrin Comprehensive Cancer Center (Université Clermont Auvergne). Clinical and biological data obtained, as well as imaging results, are registered in our database. Of the 1,416 patients treated for differentiated thyroid cancer between 1995 and 2010, 159 (11.2%) patients presented a structurally persistent or recurrent disease. Management and clinical follow up of persistent and/or recurrent disease was done according to the French national guidelines for the management of differentiated thyroid cancer, and was systematically validated through weekly multidisciplinary meetings. Structural disease recurrence/persistence was confirmed through morphological evaluation (cervical ultrasound, CT-scan, 18FDG PET-CT) to identify proven malignant tissue in the cervical region. Due to incomplete follow up or to distant metastases, 74 patients were excluded. The remaining 85 patients with DTC who presented with loco regional (cervical) cancer persistence or recurrence after initial thyroidectomy and RAI for remnant ablation were included. These patients received second surgical intervention (re-operated) for disease persistence or recurrence. Among them, 49 patients had a complementary adjuvant RAI (Ad-RAI) performed shortly after re-operation, while 36 patients without an adjuvant RAI were only followed-up (Figure 1).
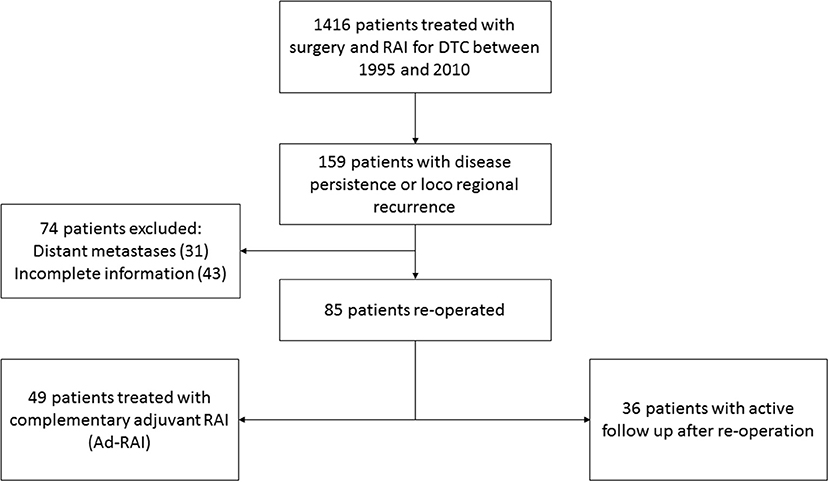
Figure 1. Flow chart of inclusion of patients in the study.
The impact of ad-RAI on recurrence-free survival was evaluated in comparison to patients without adjuvant RAI.
Each patient was informed about this retrospective study before inclusion and analysis. No signed consent was necessary according to French legislation. Authorization and approval for data inclusion in this study was requested through individual letters sent to each patient describing the study's purpose and methods. Patients' opposition was respected, and their data was excluded from the database. Included patients had the right to obtain the main results of study if they wished. Study ethics approval was obtained on June 30, 2017 (CECIC Rhône-Alpes-Auvergne, Grenoble), IRB 5921.
All patients had undergone total thyroidectomy, either at our institution or at a regional hospital, followed by RAI ablation (100 mCi). A detailed histopathological description of the DTC with its particularities (cell types), extension, and staging was performed for all patients. RAI ablation was systematically decided through a multi-disciplinary meeting.
All RAIs were administered under thyroid hormone withdrawal (THW). THW consisted of LT4 withdrawal during the 5 weeks prior to RAI administration. LT4 was substituted with LT3 during the first 3 weeks, then stopped. Stimulated thyroglobulin (sTg) and anti-Tg antibodies were evaluated on the day of RAI therapy. A diagnostic whole body scintiscan (WBS) was performed on day 5 after RAI in order to document the RAI avidity of any structural disease or thyroid remnant. Six to twelve months after RAI administration, measurement of rhTSH-stimulated serum Tg, WBS, and cervical ultrasonography were performed to evaluate response to initial treatment and Tg status. Afterwards, patients were followed up through clinical checkup, laboratory testing and ultrasonography. In selected cases, additional CT imaging at varying intervals were performed.
TNM staging system of AJCC 2010 (7th edition) was used. Thyroid capsule invasion (i.e., the difference between T2 and T3) and tumor size were considered in our cohort in order to be compatible with the new TNM system published just after the completion of the collection of our variables (2017).
Thyroglobulin measurement methodology remained unaltered throughout the duration of the study. The measurement was performed in the laboratory of radiopharmacology in the Jean Perrin Center. Immuno-radiometric assay with coated tubes (CisBio:TgIRMA) was used for this purpose, with a nadir of 0.1 μg/l. Evaluation of possible antibody interference was thoroughly performed.
Initial management or treatment is defined as a primary thyroidectomy followed by remnant ablation by RAI. Long-term remission, deemed an excellent response, is defined by absence of biochemical and/or morphological signs of disease, and absence of any need for a second treatment (re-operation or ad-RAI).
Persistent disease is defined based on the identification of a structural and/or biochemical persistence of cancer after the initial management.
Recurrent disease is defined as evidence of disease re-emergence after an initial remission (i.e., structural lesion identified by US, WBS, and/or biochemical increment of thyroglobulin). Disease recurrence was detected as a result of regular radiological and biochemical monitoring of these patients.
Biological and morphological evaluation was performed 6–12 months after RAI. Patients were evaluated under rhTSH stimulation. Undetectable sTg, normal cervical ultrasound, and normal radio isotope scan (0.18 GBq of 131I) suggest a long-term remission or excellent response.
Any anomaly persisting during the initial evaluation (e.g., incomplete biochemical and/or structural response) is considered disease persistence. Disease recurrence is defined as the appearance of biochemical or structural anomalies in patients previously considered in remission.
The statistical analysis aimed to describe the general characteristics of the population at inclusion. Quantitative parameters are expressed as a mean with standard deviation (SD), or median [range] in cases of non-Gaussian distribution. Categorical parameters are expressed as population per category and as frequencies (%). Relationships between variables were analyzed with Chi2 for qualitative parameters, and Anova and Kruskal-Wallis H tests for quantitative parameters (depending on normality and/or homoscedasticity of distributions).
The prognostic value of different factors affecting recurrence-free survival was estimated using Kaplan-Meier curves. Statistical comparisons were achieved with Log-Rank and Mantel-Haenszel tests. The study of the impact of complementary RAI on survival without recurrence was adjusted on the Propensity score using the Cox model. Propensity score was incorporated in the statistical analyses to limit bias of the prognostic tests.
Propensity score was calculated based on significant parameters in univariate analysis (p ≤ 0.05). They were then included in a multiple logistic regression model. The resulting probability to be re-treated by RAI was used as the propensity score (11, 12). Score validity was verified by ROC analysis and an AUC > 0.7 was considered acceptable.
Among the 85 patients included in the study, 59 were females (69.4%). Mean age at re-operation was 50.5 years (SD: 18.7). Papillary cancer was the predominant histological type of carcinoma in this cohort (92.9%). The median follow up period was 10.3 years [0.5–21.4]. The main characteristics of the population are summarized in Table 1.
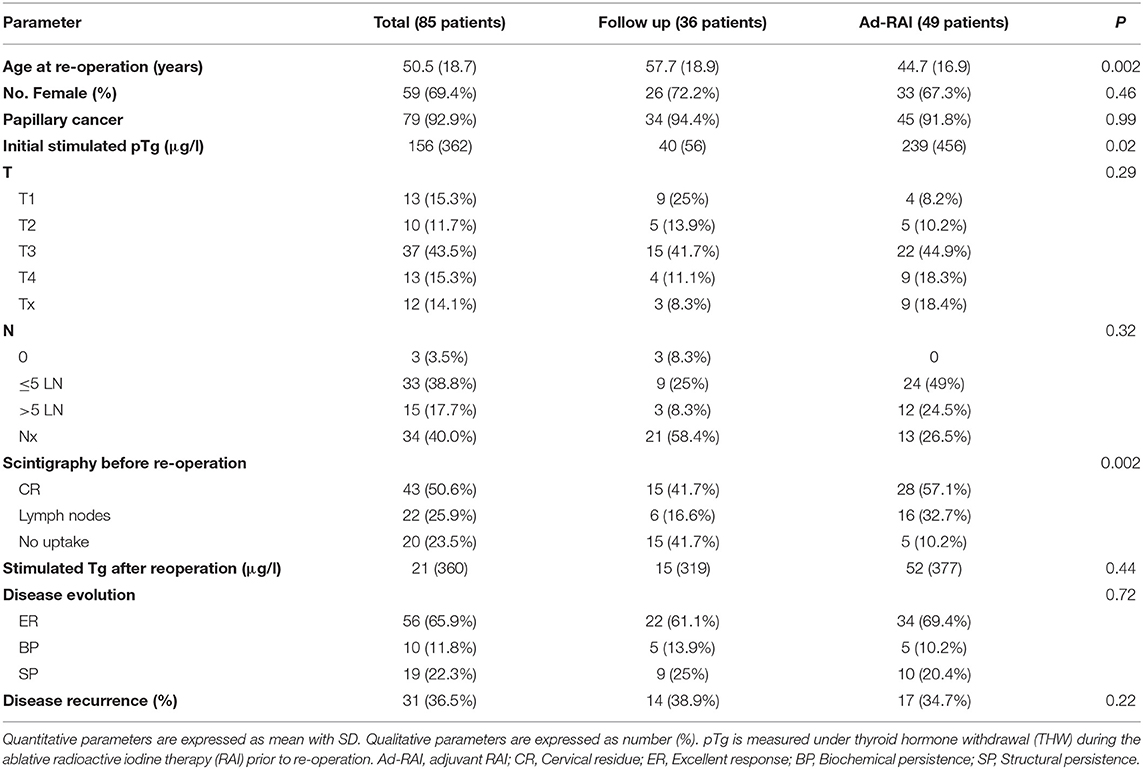
Table 1. General characteristics of the patients included in the study.
We compared patients who received an ad-RAI after re-operation (Ad-RAI group) with those who had only active follow-up after re-operation (follow-up group). Ad-RAI group patients were younger (44 years old in the Ad-RAI group vs. 57 years old in the follow-up group, p < 0.002) (Table 1). Additionally, lymph node involvement was more frequent in the Ad-RAI group (73.5 vs. 33% of patients; p < 0.00001), pre-surgical whole body scintigraphy with a positive fixation (cervical or lymph node) was more frequent in the RAI-Ad group (89.8 vs. 58.3% of patients; p < 0.01), and pre-ablation thyroglobulin levels after THW were higher in the Ad-RAI group (239 vs. 40 μg/l; p < 0.05) (Table 1).
Disease recurrence after re-treatment was detected in 31 patients (36.5%), with a median recurrence-free survival of 15.9 years. The survival curve showed a steady decline in recurrence-free survival with time (Figure 2A). The frequency of disease recurrence was stable for years following re-operation. The annual incidence of disease recurrence was 3.5%.
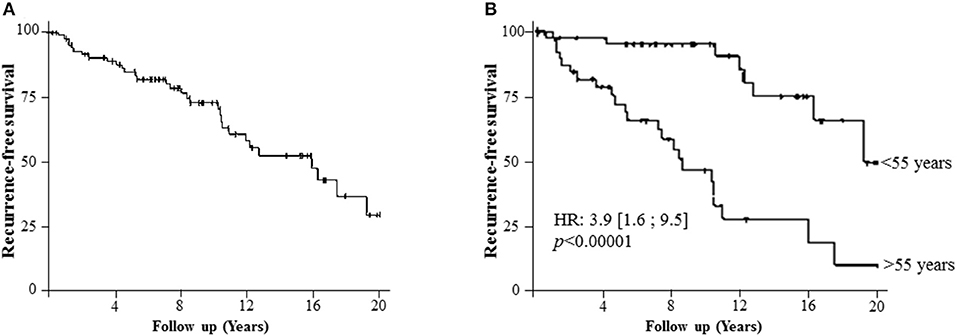
Figure 2. The recurrence-free survival of the cohort. (A) Recurrence-free survival (median 15.9 years) of the cohort demonstrating a steady decline of survival with time. (B) Recurrence-free survival in patients younger or older than 55 years old.
After a multivariate COX analysis, the main poor prognostic factor in terms of recurrence-free survival was age over 55 years (HR: 3.9 [1.6; 9.5]; p < 0.00001) (Figure 2B). Indeed, patients older than 55 years have a higher risk of recurrence independently of time, employment or not of ad-RAI. Sex, initial LN invasion status (Nx or N1), and initial radio-isotope scintigraphy results had no influence on disease recurrence.
After reoperation, thyroglobulin levels were statistically indifferent between both groups (52 vs. 15 μg/l (p = 0.44) (Table 1). Disease remission rates in the Ad-RAI group and the follow-up group did not differ (61 vs. 69%). Recurrence rates were statistically indifferent (39 vs. 34%) (Table 1). Follicular cancer was described in 6 patients (2 in the follow up group and 4 in the Ad-RAI group). All of them suffered from disease persistence or recurrence with or without ad-RAI.
Three variables were considered significant and independently predicted the choice of an ad-RAI after re-operation. These variables were used in the calculation of the Propensity score, and included: low number of previous RAI treatments, presence or absence of initial LN involvement (Nx or N1; p < 0.00001) and pTg ≥ 30 μg/l (Figure 3A). ROC analysis validated the resulting Propensity score, with an AUC > 80 (Figure 3B). Without any adjustment, the recurrence-free survival of two groups of patients (with or without adjuvant RAI) were not significantly different (p = 0.11), but tended to be in favor of the ad-RAI (median 17.4 vs. 10.9 months) (Figure 4A). The multivariate analyses adjusted on the Propensity score eliminated any difference between both groups of patients (p = 0.54), as demonstrated by Kaplan Meier curves (Figure 4B). Furthermore, multivariate analyses and Kaplan Meier curves did not show any significant benefit of ad-RAI in patients with a poor prognostic factor (age >55 years) (Figure 4C).
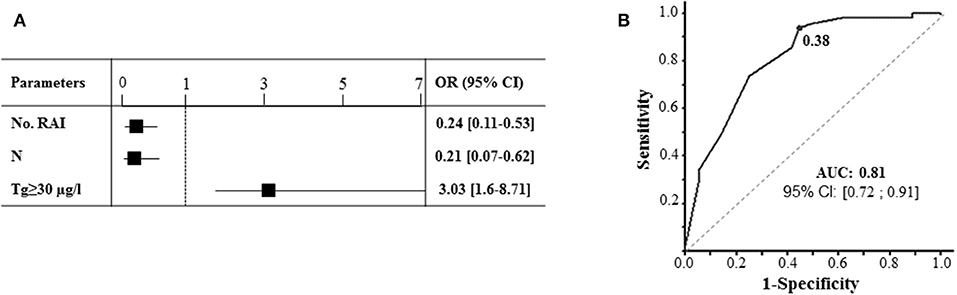
Figure 3. Estimation of Propensity score necessary for adjustment of the effect of adjuvant RAI on disease recurrence. (A) Multivariate analysis identifying parameters independently influencing the decision of administration of ad-RAI. These parameters are incorporated in the estimation of propensity score calculation. “No. RAI” represents the number of RAI therapies administered before re-operation; N represents the initial lymph node invasion status; pTg is measured under THW stimulation during the radioactive iodine therapy prior to re-operation. (B) ROC analysis with estimation of AUC to validate the Propensity score.
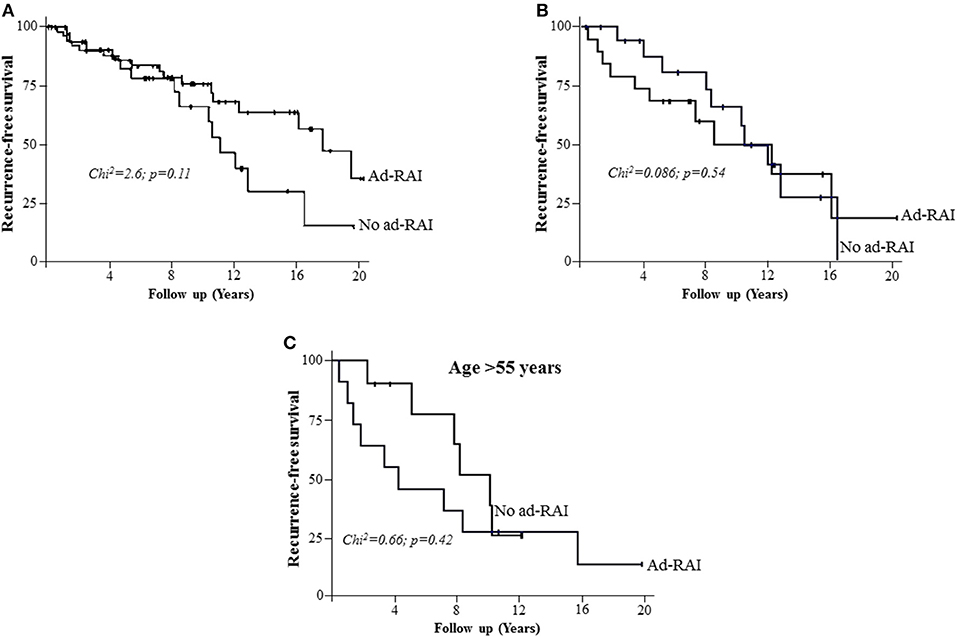
Figure 4. The impact of adjuvant RAI on the recurrence-free survival. (A) Kaplan Meier analysis demonstrating the recurrence-free survival in patients with (Ad-RAI) or without adjuvant RAI (No Ad-RAI). No significant difference between the populations was identified. (B) Kaplan Meier analysis, adjusted using the Propensity score, demonstrating the recurrence-free survival in patients with (Ad-RAI) or without (No Ad-RAI) adjuvant RAI. (C) Kaplan Meier analysis demonstrating the recurrence-free survival in patients older than 55 years old with (Ad-RAI) or without (No Ad-RAI) adjuvant RAI.
In this retrospective study, we analyzed the general prognosis of patients with DTC who were re-treated for recurrent and/or persistent loco regional (cervical) disease despite an initial thyroidectomy and RAI remnant ablation. Age, the main prognostic factor influencing recurrence-free survival, and the effect of re-treatment by ad-RAI were evaluated and adjusted using Propensity score. This study demonstrates that ad-RAI does not impact recurrence-free survival of DTC patients.
Disease persistence occurred in 34% of patients, while disease recurrence occurred in 36.5% of the patients over 15 years. Similarly, many other retrospective studies estimated the risk of disease recurrence between 1 and 50% (13–19). In addition, the survival curve of the whole population demonstrated a steady decline in the recurrence-free survival. This evidence confirms that patients with a loco regional recurrence or biochemical persistence should be followed up on a long term basis and may be considered a high risk group for disease recurrence. It is believed that this variability in the recurrence rate is highly dependent on the risk rate of DTC and the response to the initial management (6). Indeed, ATA recommendations suggest that the clinical outcome of the “structural incomplete response category” is usually disease persistence or recurrence in about 50–85% of the patients despite further therapies (7, 20–22). Such patients have worse clinical outcomes than the biochemical persistence category of patients (20).
Age constitutes a major prognostic element, and consequently, it is incorporated in the staging system (23, 24). Age over 55 years was the main poor prognostic factor in our cohort. Although survival rates in patients over the age of 45 are reduced (6, 25, 26), patients older than 55 years are known to have a higher risk of recurrence and lowest survival rates. Consequently the new staging AJCC/TNM system modified the age cut-off to 55 years (23, 24). Other factors like histological subtypes or the presence of Hashimoto's thyroiditis could change the prognosis of the patients either by increasing or reducing the recurrence rates (27–30).
Compared to the 36 patients who were only followed up after re-operation, 49 patients were re-treated with ad-RAI. After a median follow up of 10 years, no significant difference, in terms of recurrence-free survival, was noticed between patients with or without adjuvant RAI. Indeed, few studies have evaluated the impact of re-treatment with RAI on the prognosis of patients with a persistent or recurrent loco regional DTC. Yim et al. retrospectively studied 45 patients with high Tg levels who received an ad-RAI treatment (23 patients) or follow-up only (22 patients) after re-operation, and demonstrated no benefit of Ad-RAI treatment in terms of reduction of survival without recurrence or Tg levels (9). In this study, 8 patients in the ad-RAI group and 5 patients in the follow up group had disease recurrence (29% of patients). Hirsch et al. analyzed 114 patients with a persistent structural or biochemical disease after initial treatment who obtained a second dose of RAI. Only 44 patients had complete data and were re-operated on before re-treatment. In this group, 47% had a persistent disease despite the retreatment (10). In this study, no control group exists. Other studies have demonstrated a spontaneous reduction in thyroglobulin levels without further RAI in patients who previously received high doses of RAI (31, 32). With these results, ad-RAI seems hazardous for such patients and re-operation for larger tumors seems sufficient to improve the survival in patients with loco regional recurrence or persistence (7, 22). However, for smaller tumors, early re-operation could increase the risk of incomplete surgery and persistent disease. Active follow up could be useful in such patients in order to better localize the tumor burden to optimize the surgical management.
The limitations of this study include the limited sample size and the non-randomization. Furthermore, selection bias could exist due to the retrospective nature of the inclusion, as patients with Ad-RAI had higher disease burden (Tg levels, lymph node involvement, scintigraphic data before reoperation). Despite the initial difference between both groups, thyroglobulin levels after reoperation were not different. These results reflect the impact of reoperation on disease burden especially in patients with high initial thyroglobulin levels (ad-RAI group) (7). Thus, the prognosis of patients with higher disease burden in the ad-RAI group could be considered as subjectively improved as their remission and recurrence rates were aligned to the follow up group. However, this benefit is largely contributed to reoperation rather than re-treatment with RAI.
Besides, there is no randomized controlled trial evaluating the benefits of ad-RAI. Unfortunately, Yim et al.'s study which seeks to address this issue has limitations related to the general guidelines in the management of DTC. Indeed, it will be difficult to design a randomized prospective study on patients with a high disease burden with “simple follow up” vs. Ad-RAI.
However, our data are regularly and prospectively registered in our database. In order to overcome these limitations, we used a Propensity score as previously described (11, 12) and this is the best methodology when no prospective randomized trial can be performed.
Adjuvant RAI in patients re-treated for locally persistent or recurrent DTC did not improve the recurrence-free survival of patients. The recurrence rate was constant with time and was mainly dependent on age. Re-operation for larger tumors appears sufficient to improve survival in patients with loco regional disease recurrence or persistence.
All datasets generated for this study are included in the manuscript/supplementary files.
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards. All individual participants included in the study were informed and their opposition was respected. Study ethics approval was obtained on June 30, 2017 (CECIC Rhône-Alpes-Auvergne, Grenoble), IRB 5921.
CB, BB, and AK collected data. FK completed statistical analyses. PK, MB-L, IT, AK, FC, MC, and SM participated in the management of patients. AK, FC, IT, MB-L, and SM designed the study, carefully reviewed the results, and reviewed the paper. SM wrote the paper.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
1. Davies L, Welch HG. Increasing incidence of thyroid cancer in the United States, 1973-2002. JAMA. (2006) 295:2164–7. doi: 10.1001/jama.295.18.2164
2. Schlumberger MJ. Papillary and follicular thyroid carcinoma. N Engl J Med. (1998) 338:297–306. doi: 10.1056/NEJM199801293380506
3. Mazzaferri EL, Jhiang SM. Long-term impact of initial surgical and medical therapy on papillary and follicular thyroid cancer. Am J Med. (1994) 97:418–28. doi: 10.1016/0002-9343(94)90321-2
4. Leboulleux S, Rubino C, Baudin E, Caillou B, Hartl DM, Bidart J-M, et al. Prognostic factors for persistent or recurrent disease of papillary thyroid carcinoma with neck lymph node metastases and/or tumor extension beyond the thyroid capsule at initial diagnosis. J Clin Endocrinol Metab. (2005) 90:5723–9. doi: 10.1210/jc.2005-0285
5. Nascimento C, Borget I, Ghuzlan AA, Deandreis D, Chami L, Travagli JP, et al. Persistent disease and recurrence in differentiated thyroid cancer patients with undetectable postoperative stimulated thyroglobulin level. Endocr Relat Cancer. (2011) 18:R29–40. doi: 10.1677/ERC-10-0292
6. Haugen BR, Alexander EK, Bible KC, Doherty GM, Mandel SJ, Nikiforov YE, et al. 2015 American Thyroid Association management guidelines for adult patients with thyroid nodules and differentiated thyroid cancer: the American Thyroid Association guidelines task force on thyroid nodules and differentiated thyroid cancer. Thyroid. (2016) 26:1–133. doi: 10.1089/thy.2015.0020
7. Yim JH, Kim WB, Kim EY, Kim WG, Kim TY, Ryu J-S, et al. The outcomes of first reoperation for locoregionally recurrent/persistent papillary thyroid carcinoma in patients who initially underwent total thyroidectomy and remnant ablation. J Clin Endocrinol Metab. (2011) 96:2049–56. doi: 10.1210/jc.2010-2298
8. Rondeau G, Fish S, Hann LE, Fagin JA, Tuttle RM. Ultrasonographically detected small thyroid bed nodules identified after total thyroidectomy for differentiated thyroid cancer seldom show clinically significant structural progression. Thyroid. (2011) 21:845–53. doi: 10.1089/thy.2011.0011
9. Yim JH, Kim WB, Kim EY, Kim WG, Kim TY, Ryu J-S, et al. Adjuvant radioactive therapy after reoperation for locoregionally recurrent papillary thyroid cancer in patients who initially underwent total thyroidectomy and high-dose remnant ablation. J Clin Endocrinol Metab. (2011) 96:3695–700. doi: 10.1210/jc.2011-1270
10. Hirsch D, Gorshtein A, Robenshtok E, Masri-Iraqi H, Akirov A, Duskin Bitan H, et al. Second radioiodine treatment: limited benefit for differentiated thyroid cancer with locoregional persistent disease. J Clin Endocrinol Metab. (2018) 103:469–76. doi: 10.1210/jc.2017-01790
11. Kwiatkowski F, Slim K, Verrelle P, Chamorey E, Kramar A. [Propensity score: interest and limits]. Bull Cancer. (2007) 94:680–6. doi: 10.1684/bdc.2007.0412
12. Filleron T, Kwiatowski F. [Propensity score: a credible alternative to randomization?]. Bull Cancer. (2016) 103:113–22. doi: 10.1016/j.bulcan.2015.10.012
13. Tuttle RM, Tala H, Shah J, Leboeuf R, Ghossein R, Gonen M, et al. Estimating risk of recurrence in differentiated thyroid cancer after total thyroidectomy and radioactive iodine remnant ablation: using response to therapy variables to modify the initial risk estimates predicted by the new American Thyroid Association staging system. Thyroid. (2010) 20:1341–9. doi: 10.1089/thy.2010.0178
14. Vaisman F, Momesso D, Bulzico DA, Pessoa CH, Dias F, Corbo R, et al. Spontaneous remission in thyroid cancer patients after biochemical incomplete response to initial therapy. Clin Endocrinol. (2012) 77:132–8. doi: 10.1111/j.1365-2265.2012.04342.x
15. Castagna MG, Maino F, Cipri C, Belardini V, Theodoropoulou A, Cevenini G, et al. Delayed risk stratification, to include the response to initial treatment (surgery and radioiodine ablation), has better outcome predictivity in differentiated thyroid cancer patients. Eur J Endocrinol. (2011) 165:441–6. doi: 10.1530/EJE-11-0466
16. Piccardo A, Arecco F, Morbelli S, Bianchi P, Barbera F, Finessi M, et al. Low thyroglobulin concentrations after thyroidectomy increase the prognostic value of undetectable thyroglobulin levels on levo-thyroxine suppressive treatment in low-risk differentiated thyroid cancer. J Endocrinol Invest. (2010) 33:83–7. doi: 10.1007/BF03346558
17. Kloos RT. Thyroid cancer recurrence in patients clinically free of disease with undetectable or very low serum thyroglobulin values. J Clin Endocrinol Metab. (2010) 95:5241–8. doi: 10.1210/jc.2010-1500
18. Brassard M, Borget I, Edet-Sanson A, Giraudet A-L, Mundler O, Toubeau M, et al. Long-term follow-up of patients with papillary and follicular thyroid cancer: a prospective study on 715 patients. J Clin Endocrinol Metab. (2011) 96:1352–9. doi: 10.1210/jc.2010-2708
19. Verburg FA, Stokkel MPM, Düren C, Verkooijen RBT, Mäder U, van Isselt JW, et al. No survival difference after successful (131)I ablation between patients with initially low-risk and high-risk differentiated thyroid cancer. Eur J Nucl Med Mol Imaging. (2010) 37:276–83. doi: 10.1007/s00259-009-1315-6
20. Vaisman F, Tala H, Grewal R, Tuttle RM. In differentiated thyroid cancer, an incomplete structural response to therapy is associated with significantly worse clinical outcomes than only an incomplete thyroglobulin response. Thyroid. (2011) 21:1317–22. doi: 10.1089/thy.2011.0232
21. Vaisman F, Shaha A, Fish S, Michael Tuttle R. Initial therapy with either thyroid lobectomy or total thyroidectomy without radioactive iodine remnant ablation is associated with very low rates of structural disease recurrence in properly selected patients with differentiated thyroid cancer. Clin Endocrinol. (2011) 75:112–9. doi: 10.1111/j.1365-2265.2011.04002.x
22. Al-Saif O, Farrar WB, Bloomston M, Porter K, Ringel MD, Kloos RT. Long-term efficacy of lymph node reoperation for persistent papillary thyroid cancer. J Clin Endocrinol Metab. (2010) 95:2187–94. doi: 10.1210/jc.2010-0063
23. Tuttle RM, Haugen B, Perrier ND. Updated American Joint Committee on Cancer/Tumor-Node-Metastasis Staging System for differentiated and anaplastic thyroid cancer (eighth edition): what changed and why? Thyroid. (2017) 27:751–6. doi: 10.1089/thy.2017.0102
24. Nixon IJ, Wang LY, Migliacci JC, Eskander A, Campbell MJ, Aniss A, et al. An international multi-institutional validation of age 55 years as a cutoff for risk stratification in the AJCC/UICC staging system for well-differentiated thyroid cancer. Thyroid. (2016) 26:373–80. doi: 10.1089/thy.2015.0315
25. Schvartz C, Bonnetain F, Dabakuyo S, Gauthier M, Cueff A, Fieffé S, et al. Impact on overall survival of radioactive iodine in low-risk differentiated thyroid cancer patients. J Clin Endocrinol Metab. (2012) 97:1526–35. doi: 10.1210/jc.2011-2512
26. Jonklaas J, Nogueras-Gonzalez G, Munsell M, Litofsky D, Ain KB, Bigos ST, et al. The impact of age and gender on papillary thyroid cancer survival. J Clin Endocrinol Metab. (2012) 97:E878–87. doi: 10.1210/jc.2011-2864
27. Vita R, Ieni A, Tuccari G, Benvenga S. The increasing prevalence of chronic lymphocytic thyroiditis in papillary microcarcinoma. Rev Endocr Metab Disord. (2018) 19:301–9. doi: 10.1007/s11154-018-9474-z
28. Kim EY, Kim WG, Kim WB, Kim TY, Kim JM, Ryu J-S, et al. Coexistence of chronic lymphocytic thyroiditis is associated with lower recurrence rates in patients with papillary thyroid carcinoma. Clin Endocrinol. (2009) 71:581–6. doi: 10.1111/j.1365-2265.2009.03537.x
29. van Velsen EFS, Stegenga M, van Kemenade FJ, Kam B, van Ginhoven TM, Visser WE, et al. Evaluating the 2015 American Thyroid Association risk stratification system in high risk papillary and follicular thyroid cancer patients. Thyroid. (2019) 29:1073–9. doi: 10.1089/thy.2019.0053
30. Barres B, Kelly A, Kwiatkowski F, Batisse-Lignier M, Fouilhoux G, Aubert B, et al. Stimulated thyroglobulin and thyroglobulin reduction index predict excellent response in differentiated thyroid cancers. J Clin Endocrinol Metab. (2019) 104:3462–72. doi: 10.1210/jc.2018-02680
31. Pacini F, Agate L, Elisei R, Capezzone M, Ceccarelli C, Lippi F, et al. Outcome of differentiated thyroid cancer with detectable serum Tg and negative diagnostic (131)I whole body scan: comparison of patients treated with high (131)I activities versus untreated patients. J Clin Endocrinol Metab. (2001) 86:4092–7. doi: 10.1210/jcem.86.9.7831
32. Baudin E, Do Cao C, Cailleux AF, Leboulleux S, Travagli JP, Schlumberger M. Positive predictive value of serum thyroglobulin levels, measured during the first year of follow-up after thyroid hormone withdrawal, in thyroid cancer patients. J Clin Endocrinol Metab. (2003) 88:1107–11. doi: 10.1210/jc.2002-021365
Keywords: differentiated thyroid cancer, adjuvant RAI, recurrence, persistence, re-operation, re-treatment
Citation: Bouvet C, Barres B, Kwiatkowski F, Batisse-Lignier M, Chafai El Alaoui M, Kauffmann P, Cachin F, Tauveron I, Kelly A and Maqdasy S (2019) Re-treatment With Adjuvant Radioactive Iodine Does Not Improve Recurrence-Free Survival of Patients With Differentiated Thyroid Cancer. Front. Endocrinol. 10:671. doi: 10.3389/fendo.2019.00671
Received: 29 April 2019; Accepted: 16 September 2019;
Published: 27 September 2019.
Edited by:
Caterina Mian, University of Padova, ItalyReviewed by:
Roberto Vita, University of Messina, ItalyCopyright © 2019 Bouvet, Barres, Kwiatkowski, Batisse-Lignier, Chafai El Alaoui, Kauffmann, Cachin, Tauveron, Kelly and Maqdasy. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Salwan Maqdasy, c21hcWRhc3lAY2h1LWNsZXJtb250ZmVycmFuZC5mcg==
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.