 Pâmella Goveia1*
Pâmella Goveia1* Wilson Cañon-Montañez2
Wilson Cañon-Montañez2 Danilo de Paula Santos1
Danilo de Paula Santos1 Gabriela W. Lopes1
Gabriela W. Lopes1 Ronald C. W. Ma3Bruce B. Duncan1Patricia K. Ziegelman1Maria Inês Schmidt1
Ronald C. W. Ma3Bruce B. Duncan1Patricia K. Ziegelman1Maria Inês Schmidt1- 1Postgraduate Program in Epidemiology, Universidade Federal do Rio Grande do Sul, Porto Alegre, Brazil
- 2Faculty of Nursing, Universidad de Antioquia, Medellín, Colombia
- 3Department of Medicine and Therapeutics, The Chinese University of Hong Kong, Prince of Wales Hospital, Shatin, China
Background: Type 2 diabetes is increasing among the young, and gestational diabetes (GDM) offers a unique opportunity for diabetes prevention. We aimed to systematically review postpartum randomized trials to summarize the benefits of lifestyle interventions for women with previous GDM.
Methods:We searched for RCTs involving women with previous GDM that compared lifestyle interventions—diet, physical activity or breastfeeding—at postpartum with usual care up to May 2018.
Results:Of 1,895 abstracts identified, we selected 15 studies investigating incidence of diabetes or changes in glycemia. Most interventions focused on changes in diet and physical activity, only one also on incentive to breastfeeding. Meta-analysis of 8 studies investigating incidence of diabetes revealed a homogeneous (I2 = 10%), reduction of 25% (RR = 0.75; 95%CI: 0.55–1.03) borderline statistically significant. Only trials offering intervention soon after delivery (< 6 months post-partum) were effective (RR = 0.61; 95%CI: 0.40–0.94; p for subgroup comparison = 0.11). Overall, no benefit was found regarding measures of glycemia. Although moderate reductions in weight (MD = −1.07 kg; −1.43−0.72 kg); BMI (MD = −0.94 kg/m2; −1.79 −0.09 kg/m2); and waist circumference (MD = −0.98 cm; −1.75 −0.21 cm) were observed, effects were larger with longer follow-up.
Conclusions:Summary results of the available evidence support benefits of lifestyle interventions at postpartum for women with previous GDM. Benefits, although smaller than those of major trials based in older subjects receiving intensive interventions, appear clinically relevant for this young subset of woman. Further studies are needed to improve the quality of the evidence and to further tailor interventions to this specific setting.
Introduction
The International Diabetes Federation (IDF) estimates that at least 425 million persons in the world have diabetes (1).From 1980 to 2014 the global age–standardized prevalence of diabetes in adults more than doubled in men and increased almost 60% in women (2). If these trends continue, the World Health Organization (WHO) goal of halting the rise of diabetes by 2025 will not be achieved (2). The increasing burden of diabetes challenges individuals, families and health systems globally.
Diabetes can be prevented or delayed with intensive lifestyle changes offered to high-risk people, as indicated as indicated by the following now classical studies. The Da Qing Diabetes Prevention Study, after 6 years of lifestyle intervention, reduced the incidence of diabetes by 31, 46, and 42% in the groups of diet, exercise and diet plus exercise, respectively (3),and benefits extended over 20 years after the intervention was discontinued (4). The Finnish Diabetes Prevention Study (DPS) and the Diabetes Prevention Program (DPP) both showed a reduction of 58% in the incidence of diabetes mellitus in individuals with impaired glucose tolerance after an average of 3 years of lifestyle interventions focusing on diet and physical activity (5, 6). A recent systematic review of 43 studies evaluating the long-term sustainability of diabetes prevention approaches showed that the superiority of lifestyle interventions over medications observed at the end of the trial persisted for many years (7). The review included 49,029 participants with mean age of 57.3 (±8.7) years, indicating that the younger age group has been little evaluated.
Of great concern, prevalence of type 2 diabetes is increasing among the young, a phenomenon potentially increasing the burden of disease owing to the longer duration of diabetes and the apparently high incidence of chronic complications of those so affected (8, 9). Thus, diabetes prevention starting earlier than the settings of most published trials is of paramount importance. Gestational diabetes mellitus (GDM) offers a unique opportunity for diabetes prevention in younger adults. First, the diagnosis of GDM confers an increased risk of diabetes and its complications which appears to be mediated at least in part by subsequent weight gain and lack of a healthy lifestyle (10). Initial studies testing the efficacy of lifestyle interventions suggest benefit (11–25), but few systematic reviews have been carried out so far (26–28), with only one attempting to assess diabetes as an outcome (26).
We aim to systematically review and summarize the benefits of lifestyle interventions in the prevention of diabetes as well as in reduction of plasma glucose levels and anthropometry measures in women with recent GDM, as evaluated in postpartum randomized controlled trials.
Methods
Protocol and Registration
This is a systematic review and meta-analysis of randomized controlled trials (RCTs), registered with the International Prospective Register of Ongoing Systematic Reviews (PROSPERO) under the number CRD42018092440, and following the recommendations of the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA Statement) (29) and the Cochrane Handbook for Systematic Reviews of Interventions.
Eligibility Criteria
The review included all RCTs involving women with previous GDM (as defined by any recognized diagnostic criteria) that compared lifestyle interventions—diet and/or physical activity and/or breastfeeding—with usual care without pharmacological treatment. We included only trials assessing the incident of diabetes mellitus (primary outcome) or glycemic levels ((mean change from baseline of fasting or 2 h glucose, or HbA1C), our surrogate outcomes. We excluded studies including women with current or previous diagnosis of type 1 or type 2 diabetes, using pharmacological interventions or having recruitment strategies that were not based on a recent diagnosis of GDM.
Literature Search
We searched PubMed, Cochrane Central Register of Controlled Trials, Web of Science and EMBASE databases in May, 2018. The search string for PubMed was: (“Diabetes, Gestational” [Mesh] OR “Diabetes, Pregnancy-Induced” OR “Diabetes, Pregnancy Induced” OR “Pregnancy-Induced Diabetes” OR “Gestational Diabetes” OR “Diabetes Mellitus, Gestational” OR “Gestational Diabetes Mellitus”) AND (“Exercise”[Mesh] OR Exercises OR “Physical Activity” OR “Activities, Physical” OR “Activity, Physical” OR “Physical Activities” OR “Exercise, Physical” OR “Exercises, Physical” OR “Physical Exercise” OR “Physical Exercises” OR “Diet”[Mesh] OR Diets OR “Body Weight”[Mesh] OR “Weight, Body” OR “Weight Loss”[Mesh] OR “Loss, Weight” OR “Losses, Weight” OR “Weight Losses” OR “Weight Reduction” OR “Reduction, Weight” OR “Reductions, Weight” OR “Weight Reductions” OR “Life Style”[Mesh] OR “Life Styles” OR Lifestyle OR Lifestyles) AND (“controlled study” OR trial*).These terms were adjusted to fit the requirements of each electronic database. We screened the list of references of the included studies and of systematic reviews to check for other possible studies to be included.
We did not include terms for the primary outcome to enhance the search sensitivity. We made no restrictions regarding language or publication date.
Data Extraction
Initially, two reviewers (DS, GL) independently analyzed titles and abstracts of each paper retrieved to identify potential eligible studies. Inconsistencies were discussed and studies not clearly meeting the inclusion criteria were excluded. Disagreements were resolved by discussion with a third reviewer (PG) whenever necessary.
A standard data form was used to extract the following information: study population, demographic data and baseline characteristics of participants, details of the intervention and the control counterpart, results, moments of measurement; and information for assessment of risk of bias.
Relevant missing information was requested from the original authors. Procedures for estimation of missing data were performed whenever possible (29). If data were still insufficient after these processes, the outcome was included in descriptive analysis only.
Outcomes
The primary outcome was incidence of diabetes mellitus. We also reported change in glycemic levels (mean fasting or 2 h glucose, or HbA1C). Secondary outcomes were changes in the anthropometric measures of weight and waist circumference.
Risk of Bias (Quality) Assessment
Three reviewers in pairs (DS, GL, PG) independently assessed the quality of the studies. The disagreements were resolved by consensus or with the consultation of an additional author (WC).
We evaluated the risk of bias as described in the Cochrane Handbook for Systematic Reviews of Interventions using the Cochrane Collaboration tool (29), with the following criteria: random sequence generation (selection bias); allocation concealment (selection bias); blinding (performance bias and detection bias) considering blinding of participants, personnel and those performing outcome assessment; incomplete outcome data (attrition bias); selective reporting (reporting bias); and other biases.
Data Analysis
We estimated relative risks for the incidence of diabetes mellitus. For continuous outcomes, we estimated mean differences from baseline. When standard deviations for changes were missing, we made imputations considering a conservator correlation equal to zero. We used random effects models with DerSimonian and Laird estimators for analyses of all outcomes. All statistical tests were two-sided and significance was defined as P < 0.05. We assessed statistical heterogeneity of treatment effects across studies using the I2 metric statistics. The statistical analyses were performed used R version 3.5.0 (R Foundation for Statistical Computing). In addition, publication bias was examined using funnel plot and the Egger test (Stata 11.0, StataCorp, College Station, TX).
Results
Study Selection and Patient Characteristics
The flowchart for the selection and exclusion of studies is presented in Figure 1. After removing duplicates, we found a total of 1,895 abstracts from where 38 articles were considered as potentially eligible and assessed through full-text reading. We then excluded 23 additional studies, remaining with a total of 15 studies. The reasons for exclusion were: not a randomized controlled trial (n = 4) (30–33), not reporting our primary outcomes (n = 13) (34–46), study population not meeting our inclusion criteria specification (n = 4) (47–50) and different reports from the same study (n = 2) (51, 52).
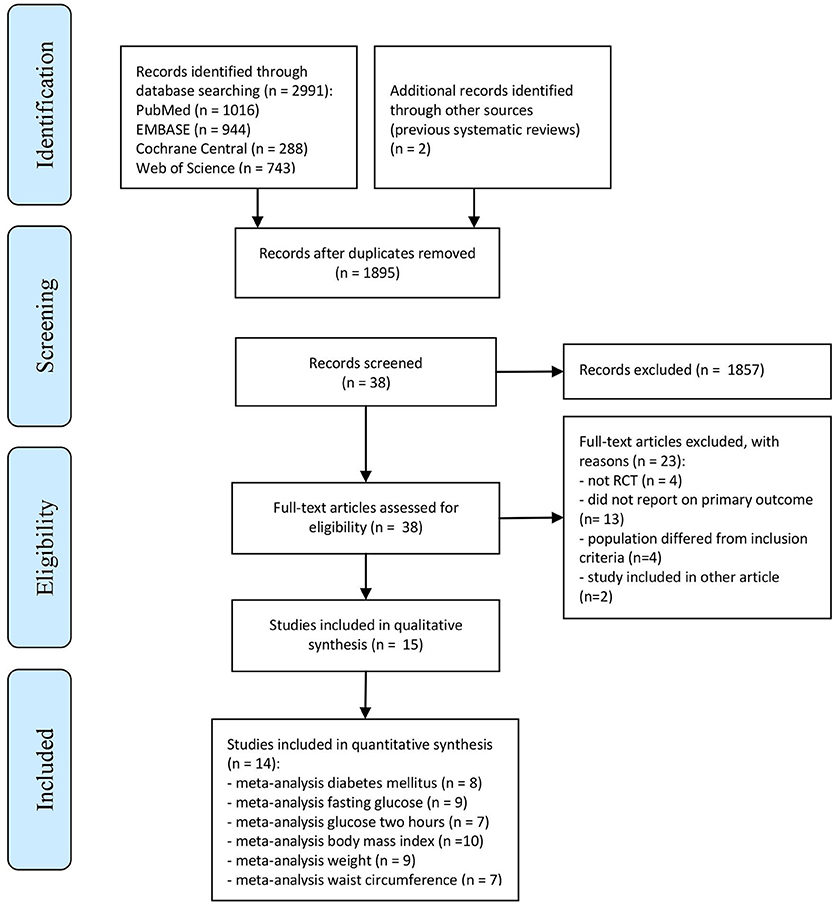
Figure 1. Flow chart summarizing the process for the identification of the eligible studies.
The 15 studies included in the systematic review are described in Table 1. All articles were published within the last 10 years, except one (11). Studies took place in the United States (11–13), Australia (14–16, 25), China (17–20), Spain (21), Malaysia (22), Israel (23), and Ireland (24). The number of women who were randomized in individual studies ranged from 28 to 573, with 8 studies including at least 100 participants (11, 16–21, 23). Ten studies specified eligibility criteria regarding the risk of diabetes: postpartum glucose intolerance (11, 17, 18, 20–22, 24), overweight or obesity (13, 22, 24), low level of physical activity (12, 25), altered lipid profile (24), high waist circumference (22, 24), family history of diabetes (22), use of insulin during pregnancy (17) or hypertension (24).
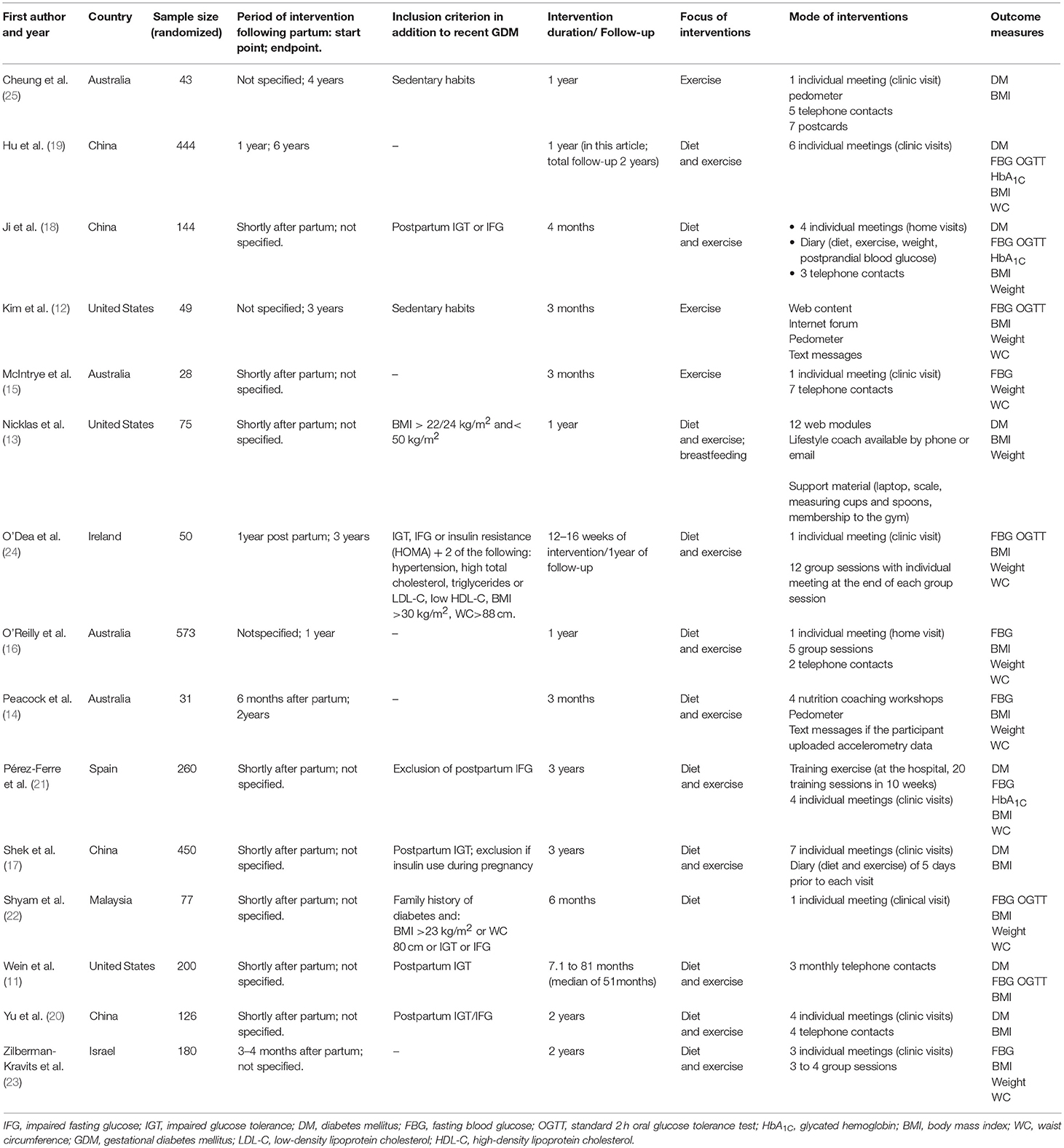
Table 1. Characteristics of the included studies.
Duration of follow-up was 6 months or less in 5 studies (12, 14, 15, 18, 22), 1 year in 5 studies (13, 16, 19, 24, 25), and 2 years or more in 5 studies (11, 17, 20, 21, 23).
Most of the interventions focused on changes in diet and physical activity. Only one study mentioned incentive to breastfeed (13). Three studies focused solely on the effectiveness of physical activity intervention (12, 15, 25) and one only on diet (22). Standard/brief advice on diet and/or exercise was considered to be comparable with usual care and accepted as the control comparison. Different ways of delivering the intervention were applied: Nine established remote contact (11–16, 18, 20, 25) (by phone, internet or postcards); four performed group sessions (14, 16, 23, 24), and eleven had individual face-to-face contacts (15–25). From those which held individual meetings, two conducted home visits (16, 18) and the others held the sessions in the clinic/hospital.
Eight trials had data to estimate incident diabetes (11, 13, 17–21, 25). Eleven trials measured glycemic control (11, 12, 14–16, 18, 19, 21–24), and all trials investigated the effect on body weight. Overall, considerable heterogeneity was evident between studies in relation to several key characteristics, namely, the method of the intervention, the time lag since the pregnancy complicated by GDM, the degree of risk beyond having GDM, and the duration of follow-up.
Quality Assessment of Included Studies
Table 2 presents items necessary to assess risk of bias in each study according to the Cochrane Collaboration risk of bias tool for RCTs. Considering all studies included, 60% described adequate random sequence generation (12–18, 22, 24) and 40% allocation concealment (13–16, 22, 24). We did not evaluate blinding of staff performing the interventions due to the nature of lifestyle interventions. Only 26% of the studies mentioned blinding of the outcome assessors (12–14, 22), and it was frequently unclear whether blinding extended to all staff involved (laboratory technicians, staff making anthropometric assessments, data analysts). About half of the studies described exclusions and losses during follow-up (12–14, 16, 17, 21, 22) and a similar proportion reported intention-to-treat analysis (13, 14, 16, 17, 21, 22, 24). Some studies (11, 19, 20) though not mentioning intention to treat analysis or reasons for losses or exclusions, presented few such events, thus minimizing the possibility of bias due to incomplete outcome data.
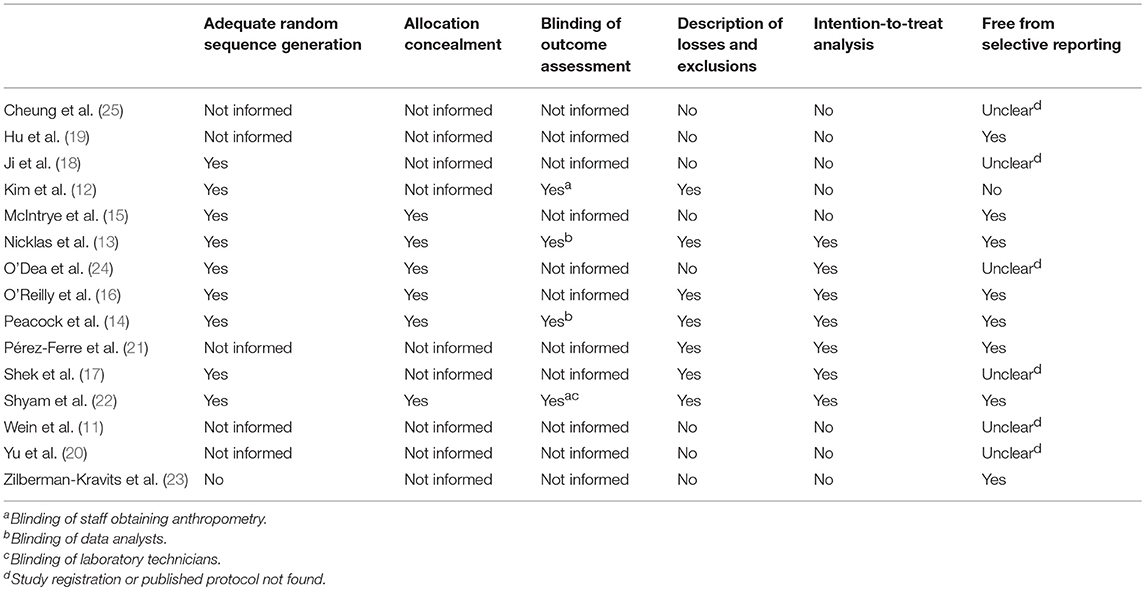
Table 2. Risk of bias among included studies.
Main Results
Meta-analysis of the 8 studies reporting incident diabetes (Figure 2) revealed a borderline statistically significant relative reduction of 25% (RR = 0.75; 95%CI: 0.55–1.03) in incidence with intervention. The results were homogeneous across studies (I2 = 10%). When stratified by time of randomization, only studies initiating earlier in the post-partum period showed a significant reduction (RR = 0.61; 95%CI: 0.40–0.94; p for subgroup comparison = 0.33). The overall absolute difference in incidence between groups was −0.04 (95%CI: −0.09; 0.01).
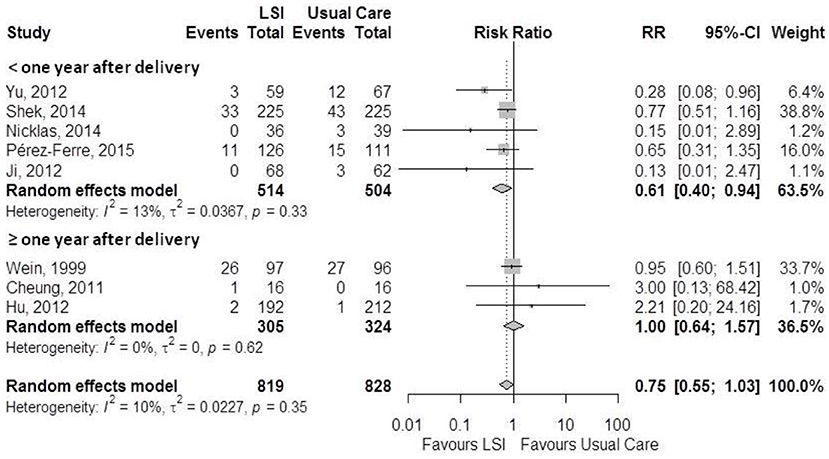
Figure 2. Meta-analysis of the effects of lifestyle interventions (LSI) in diabetes incidence according to post-partum time at randomization.
Figure 3 shows a funnel plot for the 8 studies reporting incidence of diabetes. We can observe a general funnel shape indicating that studies of lower precision were spread evenly on both sides of the average, suggesting absence of publication bias. The Egger test also indicated absence of publication bias (p = 0.47).
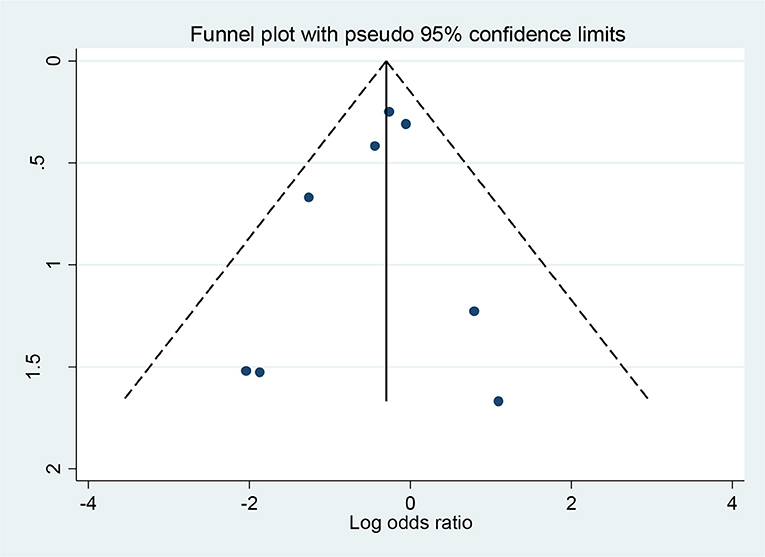
Figure 3. Funnel plot, using data from 8 trials with information for diabetes incidence. Log-odds ratios all displayed on the horizontal axis.
Figures 4, 5 showed a lack of effect of lifestyle interventions in mean fasting and 2h plasma glucose, with a non-significant difference from baseline on fasting glucose (MD = −0.13; 95%CI: −0.36; 0.09) mmol/L and on 2 h glucose (MD = −0.12; 95%CI: 0.47; 0.23) mmol/L for 2 h glucose. Only 3 studies reported HbA1c, without positive results.
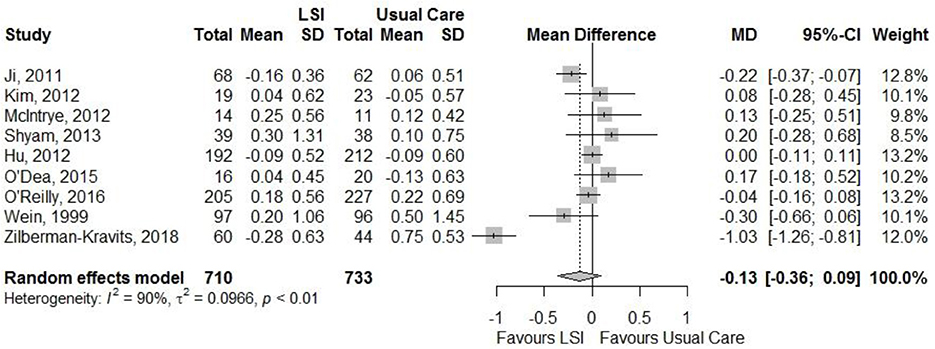
Figure 4. Meta-analysis of the effects of lifestyle interventions (LSI) in fasting glucose change (mmol/L) from baseline to the end of follow up.
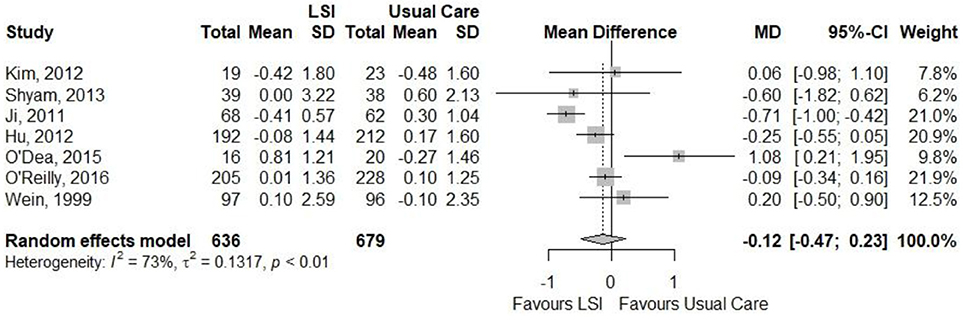
Figure 5. Meta-analysis of the effects of lifestyle interventions (LSI) in 2-h glucose change (mmol/L) from baseline to the end of follow up.
Figures 6, 7 showed that the life style intervention had a moderate statistically significant greater reductions in mean weight (MD = −1.07; 95%CI: −1.43; −0.72) kg and BMI (MD = −0.94; 95%CI: −1.79; −0.09) kg/m2, respectively, effects being larger with longer follow-up. Figure 8 also show a statistic significant greater reduction in waist circumference (MD = −0.98; 95%CI: −1.75; −0.21) cm, also larger with longer follow-up.
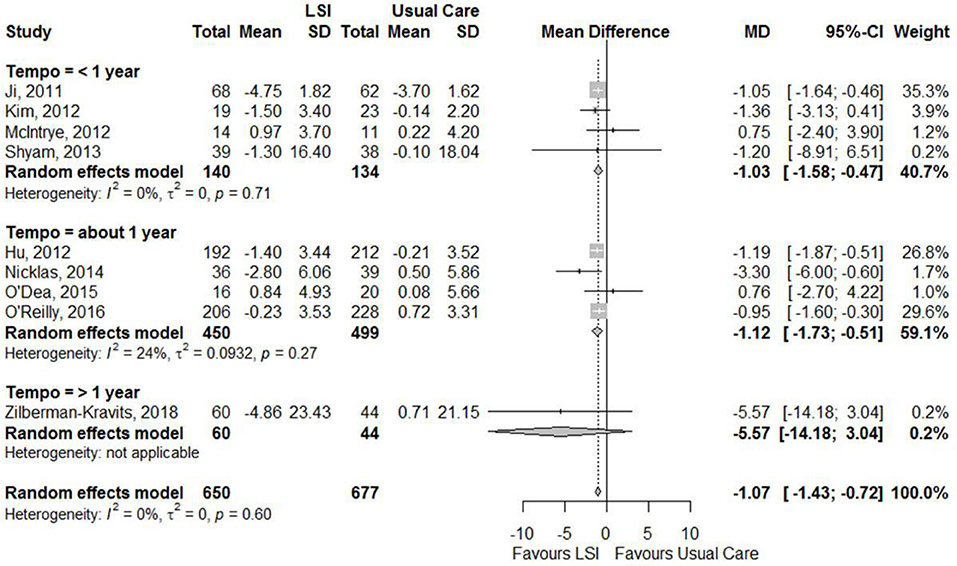
Figure 6. Meta-analysis of the effects of lifestyle interventions (LSI) in weight change (kg) from baseline to the end of follow up, according to the duration of follow-up.
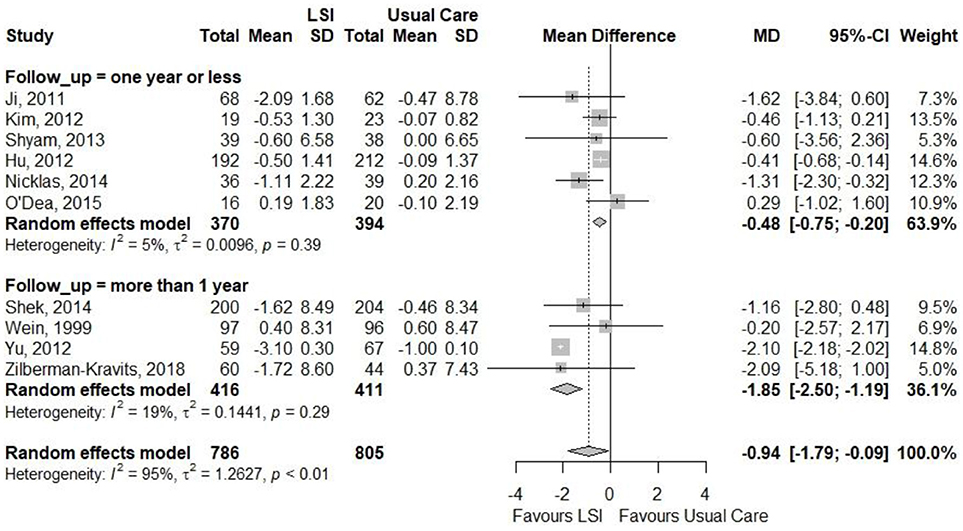
Figure 7. Meta-analysis of the effects of lifestyle interventions (LSI) in BMI change (kg/m2) from baseline to the end of follow up, according to the duration of follow-up.
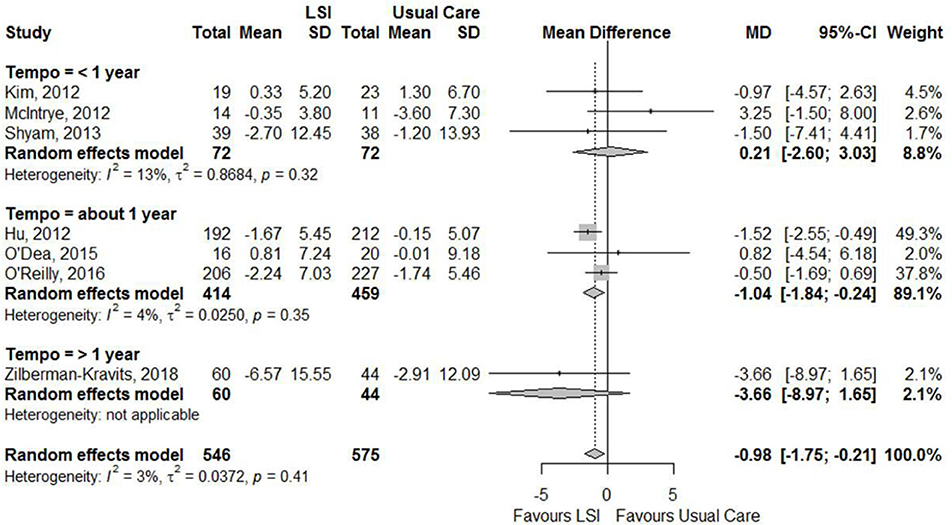
Figure 8. Meta-analysis of the effects of lifestyle interventions (LSI) in waist circumference change (cm) from baseline to the end of follow up, according to the duration of follow-up.
Discussion
Evidence here summarized reveal that lifestyle changes started after a pregnancy complicated by GDM produce a 25% (RR = 0.75; 95%CI: 0.55–1.03) reduction in diabetes risk which reaches borderline statistical significance. Effects appeared to be larger when the interventions were initiated within 6 months after birth (RR = 0.61; 95%CI: 0.40–0.94; p for subgroup comparison = 0.33). We found small but statistically significant reductions in weight, BMI and waist circumference, particularly with longer periods of intervention. In contrast, we found no change with intervention for final fasting or 2 h glucose values.
The only previous meta-analysis reporting effects on diabetes incidence among women with recent gestational diabetes (26) included four of the eight trials here summarized. It did not report relative risks but found an absolute risk difference of (RD = −5.02%; 95%CI: −9.24; −0.80), consistent with the size of the risk reduction we found. With regard to weight changes, the previous meta-analysis (27) found a similar difference mean weight reduction (MD = −1.06; 95%CI: −1.68; −0.44) kg. We found no meta-analysis reporting effects on BMI, waist circumference, 2h glucose during an oral glucose tolerance test or HbA1C. The only one reporting a summarized effect on fasting plasma glucose, like ours did not find a statistically significant difference in reduction (MD = −0.05; 95%CI: −0.21; 0.11 mmol/L).
The fact that reductions in incidence here reported were somewhat greater when the intervention initiated sooner after birth (RR = 0.61 vs. 1.00; p = 0.11) may reflect stronger motivation to initiate lifestyle changes when women are closer to their GDM treatment during pregnancy. However, the number of studies initiating later is small to reach a conclusion. We have no explanation for the small size of changes in mean glucose values, but as numbers are not large, it is possible that outliers in glucose values, once diabetes developed, could influence these glucose means. Additionally, heterogeneity across studies for these outcomes was large.
We found a consistently greater effect in studies with longer follow-up across the three anthropometric measures. In these studies, the period of intervention was also of greater duration, which suggests the importance of maintaining support for lifestyle changes for a longer period, particularly given the women's frequently overwhelming tasks of motherhood. Of note also, since breastfeeding is often being performed during the post-partum period, weight loss recommended is usually small, thus requiring a longer period than the usual weight loss programs to reach weight loss goals.
There are several ongoing trials which may complete data collection and publish their results in the next three to 4 years (53–56). Up to now, this is the most comprehensive summary reporting on the feasibility and effectiveness of lifestyle modifications soon after birth of mothers with gestational diabetes. Compared to the only previous meta-analysis reporting diabetes as an outcome (26), we have increased the number of studies involved, as well as the scope of the outcomes assessed.
Although effects are small, benefits are clinically relevant, since seemingly minimal changes in anthropometric measures over a short period translate into a 25% risk reduction of diabetes in women who are, on average, only 30 years old. We hope that these ongoing trials of longer duration and with greater support for lifestyle changes will produce larger effects, perhaps with results approaching the relative risk reduction of 53% found in post-hoc analyses focusing on women with previous gestational diabetes (47), treated about 9 to 10 years after the target pregnancy in the similarly more robust and longer DPP study.
Our study has strengths and limitations. First, the number of women randomized (1647) and the number of events (180) are still small, resulting in only borderline statistical significance. Of note however, funnel plot and Egger test indicated small chance of publication bias. The effect of 25% reduction in the incidence of diabetes is small but potentially clinical relevant. As suggested by the absolute risk difference we found, 4%, the number needed to treat is 25 women, in other words, we need to treat 25 women with GDM at postpartum with similar interventions to prevent one case of diabetes. Finally, the quality of most studies included in this review is not high and sample size often limited to less than 70 women. These limitations highlight the need for further studies to provide more accurate summary results.
In conclusion, our comprehensive meta-analysis suggests an effect of lifestyle intervention after a pregnancy complicated by gestational diabetes. The effect is smaller than those of the classic studies of lifestyle intervention to prevent diabetes in older subjects when offered more intensive interventions. Nonetheless, the benefits here reported for younger women with previous GDM suggest that interventions to prevent diabetes are feasible and may have potential clinical. Additional studies are needed to further tailor the delivery of lifestyle interventions to this particular period of life and to improve the quality of the evidence for their effectiveness when offered to women with GDM after pregnancy.
Author Contributions
MS, PG, and WC designed the study. DS, GL, PG, and RM contributed to the literature search and data extraction. PG and PZ performed data analyses. BD, MS, PG, PZ, and WC participated in the interpretation, writing, and proofreading of the manuscript.
Funding
Coordination for the Improvement of Higher Education Personnel-CAPES (grants 1680050 [PG], 156765 [DS] and 150079 [GL]).
Conflict of Interest Statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
References
1. International Diabetes Federation. IDF Diabetes Atlas, 8th ed. Brussels: International Diabetes Federation (2017). Available online at: http://www.diabetesatlas.org
2. NCD Risk Factor Collaboration (NCD-RisC). Worldwide trends in diabetes since 1980: a pooled analysis of 751 population-based studies with 4.4 million participants. Lancet (2016) 387:1513–30. doi: 10.1016/S0140-6736(16)00618-8
3. Pan XR, Li GW, Hu YH, Wang JX, Yang WY, An ZX, et al. Effects of diet and exercise in preventing NIDDM in people with impaired glucose tolerance. The Da Qing IGT and Diabetes Study. Diabetes Care (1997) 20:537–44.9096977
4. Li G, Zhang P, Wang J, Gregg EW, Yang W, Gong Q, et al. The long-term effect of lifestyle interventions to prevent diabetes in the China Da Qing Diabetes Prevention Study: a 20-year follow-up study. Lancet (2008) 371:1783–9. doi: 10.1016/S0140-6736(08)60766-7
5. Tuomilehto J, Lindström J, Eriksson JG, Valle TT, Hämäläinen H, Ilanne-Parikka P, et al. Prevention of type 2 diabetes mellitus by changes in lifestyle among subjects with impaired glucose tolerance. N Engl J Med. (2001) 344:1343–50. doi: 10.1056/NEJM200105033441801
6. Knowler WC, Barrett-Connor E, Fowler SE, Hamman RF, Lachin JM, Walker EA, et al. Reduction in the incidence of type 2 diabetes with lifestyle intervention or metformin. N Engl J Med. (2002) 346:393–403. doi: 10.1056/NEJMoa012512
7. Haw JS, Galaviz KI, Straus AN, Kowalski AJ, Magee MJ, Weber MB, et al. Long-term sustainability of diabetes prevention approaches: a systematic review and meta-analysis of randomized clinical trials. JAMA Intern Med. (2017) 177:1808–17. doi: 10.1001/jamainternmed.2017.6040
8. Mayer-Davis EJ, Lawrence JM, Dabelea D, Divers J, Isom S, Dolan L, et al. Incidence trends of type 1 and type 2 diabetes among youths, 2002-2012. N Engl J Med. (2017) 376:1419–29. doi: 10.1056/NEJMoa1610187
9. Dabelea D, Stafford JM, Mayer-Davis EJ, D'Agostino R, Dolan L, Imperatore G, et al. Association of type 1 diabetes vs type 2 diabetes diagnosed during childhood and adolescence with complications during teenage years and young adulthood. JAMA (2017) 317:825–35. doi: 10.1001/jama.2017.0686
10. Tobias DK, Stuart JJ, Li S, Chavarro J, Rimm EB, Rich-Edwards J, et al. Association of history of gestational diabetes with long-term cardiovascular disease risk in a large prospective cohort of US women. JAMA Intern Med. (2017) 177:1735–42. doi: 10.1001/jamainternmed.2017.2790
11. Wein P, Beischer N, Harris C, Permezel M. A trial of simple versus intensified dietary modification for prevention of progression to diabetes mellitus in women with impaired glucose tolerance. Aust N Z J Obstet Gynaecol. (1999) 39:162–6. doi: 10.1111/j.1479-828X.1999.tb03363.x
12. Kim C, Draska M, Hess ML, Wilson EJ, Richardson CR. A web-based pedometer programme in women with a recent history of gestational diabetes. Diabet Med. (2012) 29:278–83. doi: 10.1111/j.1464-5491.2011.03415.x
13. Nicklas JM, Zera CA, England LJ, Rosner BA, Horton E, Levkoff SE, et al. A web-based lifestyle intervention for women with recent gestational diabetes mellitus: a randomized controlled trial. Obstet Gynecol. (2014) 124:563–70. doi: 10.1097/AOG.0000000000000420
14. Peacock AS, Bogossian FE, Wilkinson SA, Gibbons KS, Kim C, McIntyre HD. A randomised controlled trial to delay or prevent type 2 diabetes after gestational diabetes: walking for exercise and nutrition to prevent diabetes for you. Int J Endocrinol. (2015) 2015:423717. doi: 10.1155/2015/423717
15. McIntyre HD, Peacock A, Miller YD, Koh D, Marshall AL. Pilot study of an individualised early postpartum intervention to increase physical activity in women with previous gestational diabetes. Int J Endocrinol. (2012) 2012:892019. doi: 10.1155/2012/892019
16. O'Reilly SL, Dunbar JA, Versace V, Janus E, Best JD, Carter R, et al. Mothers after Gestational Diabetes in Australia (MAGDA): a randomised controlled trial of a postnatal diabetes prevention program. PLoS Med. (2016) 13:e1002092. doi: 10.1371/journal.pmed.1002092
17. Shek NWM, Ngai CSW, Lee CP, Chan JYC, Lao TTH. Lifestyle modifications in the development of diabetes mellitus and metabolic syndrome in Chinese women who had gestational diabetes mellitus: a randomized interventional trial. Arch Gynecol Obstet. (2014) 289:319–27. doi: 10.1007/s00404-013-2971-0
18. Wen JW. Effects of a Lifestyle Intervention on Glycometabolism in Women Having Gestational Diabetes Mellitus and Impaired Glucose Tolerance After Delivery. Beijing: School of Nursing, PeKing Union Medical College (2011).
19. Hu G, Tian H, Zhang F, Liu H, Zhang C, Zhang S, et al. Tianjin Gestational Diabetes Mellitus Prevention Program: study design, methods, and 1-year interim report on the feasibility of lifestyle intervention program. Diabetes Res Clin Pract. (2012) 98:508–17. doi: 10.1016/j.diabres.2012.09.015
20. Yu X, Wu X, Zhang Y, Mao Y. The effects of lifestyle intervention on insulin resistance and islet β cell function in gestational diabetes patients with postpartum impaired glucose regulation. Chin J Prev Control Chronic Non-Commun Dis. (2012) 560–2. doi: 10.16386/j.cjpccd.issn.1004-6194.2012.05.037
21. Pérez-Ferre N, Del Valle L, Torrejón MJ, Barca I, Calvo MI, Matía P, et al. Diabetes mellitus and abnormal glucose tolerance development after gestational diabetes: A three-year, prospective, randomized, clinical-based, Mediterranean lifestyle interventional study with parallel groups. Clin Nutr. (2015) 34:579–85. doi: 10.1016/j.clnu.2014.09.005
22. Shyam S, Arshad F, Abdul Ghani R, Wahab NA, Safii NS, Nisak MYB, et al. Low glycaemic index diets improve glucose tolerance and body weight in women with previous history of gestational diabetes: a six months randomized trial. Nutr J. (2013) 12:68. doi: 10.1186/1475-2891-12-68
23. Zilberman-Kravits D, Meyerstein N, Abu-Rabia Y, Wiznitzer A, Harman-Boehm I. The impact of a cultural lifestyle intervention on metabolic parameters after gestational diabetes mellitus a randomized controlled trial. Matern Child Health J (2018) 22:803–11. doi: 10.1007/s10995-018-2450-0
24. O'Dea A, Tierney M, McGuire BE, Newell J, Glynn LG, Gibson I, et al. Can the Onset of type 2 diabetes be delayed by a group-based lifestyle intervention in women with prediabetes following gestational diabetes mellitus (GDM)? findings from a randomized control mixed methods trial. J Diabetes Res. (2015) 2015:798460. doi: 10.1155/2015/798460
25. Cheung NW, Smith BJ, van der Ploeg HP, Cinnadaio N, Bauman A. A pilot structured behavioural intervention trial to increase physical activity among women with recent gestational diabetes. Diabetes Res Clin Pract. (2011) 92:e27–29. doi: 10.1016/j.diabres.2011.01.013
26. Pedersen ALW, Terkildsen Maindal H, Juul L. How to prevent type 2 diabetes in women with previous gestational diabetes? A systematic review of behavioural interventions. Prim Care Diabetes (2017) 11:403–13. doi: 10.1016/j.pcd.2017.05.002
27. Gilinsky AS, Kirk AF, Hughes AR, Lindsay RS. Lifestyle interventions for type 2 diabetes prevention in women with prior gestational diabetes: a systematic review and meta-analysis of behavioural, anthropometric and metabolic outcomes. Prev Med Rep. (2015) 2:448–61. doi: 10.1016/j.pmedr.2015.05.009
28. Guo J, Chen JL, Whittemore R, Whitaker E. Postpartum lifestyle interventions to prevent type 2 diabetes among women with history of gestational diabetes: a systematic review of randomized clinical trials. J Womens Health (2016) 25:38–49. doi: 10.1089/jwh.2015.5262
29. Liberati A, Altman DG, Tetzlaff J, Mulrow C, Gøtzsche PC, Ioannidis JPA, et al. The PRISMA statement for reporting systematic reviews and meta-analyses of studies that evaluate health care interventions: explanation and elaboration. J Clin Epidemiol. (2009) 62:e1–34. doi: 10.1016/j.jclinepi.2009.06.006
30. Mukerji G, McTavish S, Glenn A, Delos-Reyes F, Price J, Wu W, et al. An innovative home-based cardiovascular lifestyle prevention program for women with recent gestational diabetes: a pilot feasibility study. Can J Diabetes (2015) 39:445–50. doi: 10.1016/j.jcjd.2015.08.002
31. Philis-Tsimikas A, Fortmann AL, Dharkar-Surber S, Euyoque JA, Ruiz M, Schultz J, et al. Dulce Mothers: an intervention to reduce diabetes and cardiovascular risk in Latinas after gestational diabetes. Transl Behav Med. (2014) 4:18–25. doi: 10.1007/s13142-014-0253-4
32. Brazeau AS, Leong A, Meltzer SJ, Cruz R, DaCosta D, Hendrickson-Nelson M, et al. Group-based activities with on-site childcare and online support improve glucose tolerance in women within 5 years of gestational diabetes pregnancy. Cardiovasc Diabetol. (2014) 13:104. doi: 10.1186/1475-2840-13-104
33. Ferrara A, Ehrlich SF, Feng J, Quesenberry CP, Moore SD, Hedderson MM. Postpartum weight loss is associated with improved glucose and insulin homeostasis in women with a history of gestational diabetes (GDM). Diabetes (2012) 61:A339.
34. Liu H, Wang L, Zhang S, Leng J, Li N, Li W, et al. One-year weight losses in the Tianjin Gestational Diabetes Mellitus Prevention Programme: a randomized clinical trial. Diabetes Obes Metab. (2018) 20:1246–55. doi: 10.1111/dom.13225
35. Liu H, Wang L, Zhang S, Leng J, Li N, Li W, et al. 1 year weight losses in the Tianjin Gestational Diabetes Mellitus Prevention Program: a randomised trial. Lancet Diabetes Endocrinol. (2016) 4:S11. doi: 10.1016/S2213-8587(16)30366-7
36. McCance DR, Draffin C, Patterson CC, Francis L, Irwin J, McConnell M, et al. Postnatal lifestyle intervention for overweight women with previous gestational diabetes mellitus (PAIGE): a pilot randomised controlled trial. Ir J Med Sci. (2016) 185:S401. doi: 10.1210/jc.2017-02654
37. McManus R, Miller D, Mottola M, Giroux I, Donovan L. Translating healthy living messages to postpartum women and their partners after gestational diabetes (GDM): body habitus, A1C, lifestyle habits, and program engagement results from the families defeating diabetes (FDD) randomized trial. Am J Health Promot. (2017) 32:1438–46. doi: 10.1177/0890117117738210
38. Reinhardt JA, van der Ploeg HP, Grzegrzulka R, Timperley JG. lmplementing lifestyle change through phone-based motivational interviewing in rural-based women with previous gestational diabetes mellitus. Health Promot J Austr. (2012) 23:5–9. doi: 10.1071/HE12005
39. Smith BJ, Cinnadaio N, Cheung NW, Bauman A, Tapsell LC, van der Ploeg HP. Investigation of a lifestyle change strategy for high-risk women with a history of gestational diabetes. Diabetes Res Clin Pract. (2014) 106:e60-63. doi: 10.1016/j.diabres.2014.09.035
40. Stuebe AM, Bonuck K, Adatorwovor R, Schwartz TA, Berry DC. A Cluster randomized trial of tailored breastfeeding support for women with gestational diabetes. Breastfeed Med. (2016) 11:504–13. doi: 10.1089/bfm.2016.0069
41. Athavale P, Thomas M, Delgadillo-Duenas AT, Leong K, Najmabadi A, Harleman E, et al. Linking high risk postpartum women with a technology enabled health coaching program to reduce diabetes risk and improve wellbeing: program description, case studies, and recommendations for community health coaching programs. J Diabetes Res. (2016) 2016:4353956. doi: 10.1155/2016/4353956
42. Brown SD, Guterman J, Gordon N, Tsai AL, Hedderson MM, Ferrara A. Evaluating a postpartum diabetes prevention program: the gestational diabetes' effects on moms (GEM) trial. Diabetes (2017) 66:A216.
43. Ferrara A, Hedderson MM, Brown SD, Albright CL, Ehrlich SF, Tsai A-L, et al. The comparative effectiveness of diabetes prevention strategies to reduce postpartum weight retention in women with gestational diabetes mellitus: the gestational diabetes' effects on moms (GEM) cluster randomized controlled trial. Diabetes Care (2016) 39:65–74. doi: 10.2337/dc15-1254
44. Ferrara A, Hedderson MM, Albright CL, Brown SD, Ehrlich SF, Mevi AA, et al. Reduced postpartum weight retention with a dpp-derived lifestyle intervention: the gestational diabetes' effects on moms (GEM) cluster randomized trial. Diabetes (2014) 63:A94–5.
45. Ferrara A, Hedderson MM, Albright CL, Ehrlich SF, Quesenberry CP, Peng T, et al. A pregnancy and postpartum lifestyle intervention in women with gestational diabetes mellitus reduces diabetes risk factors: a feasibility randomized control trial. Diabetes Care (2011) 34:1519–25. doi: 10.2337/dc10-2221
46. Jelsma JGM, van Poppel MN M, Smith BJ, Cinnadaio N, Bauman A, Tapsell L, et al. Changing psychosocial determinants of physical activity and diet in women with a history of gestational diabetes mellitus. Diabetes Metab Res Rev. (2018) 34:e2942. doi: 10.1002/dmrr.2942
47. Ratner RE, Christophi CA, Metzger BE, Dabelea D, Bennett PH, Pi-Sunyer X, et al. Prevention of diabetes in women with a history of gestational diabetes: effects of metformin and lifestyle interventions. J Clin Endocrinol Metab. (2008) 93:4774–9. doi: 10.1210/jc.2008-0772
48. Aroda VR, Christophi CA, Edelstein SL, Zhang P, Herman WH, Barrett-Connor E, et al. The effect of lifestyle intervention and metformin on preventing or delaying diabetes among women with and without gestational diabetes: the Diabetes Prevention Program outcomes study 10-year follow-up. J Clin Endocrinol Metab. (2015) 100:1646–53. doi: 10.1210/jc.2014-3761
49. Huvinen H, Koivusalo S, StachLempinen B, Kautiainen H, Eriksson J. Effects of a lifestyle intervention during pregnancy and 1-year postpartum -results from the RADIEL study. Gynecol Endocrinol. (2016) 32:161.
50. Huvinen E, Koivusalo SB, Meinilä J, Valkama A, Tiitinen A, Rönö K, et al. Effects of a lifestyle intervention during pregnancy and first postpartum year: findings from the RADIEL Study. J Clin Endocrinol Metab. (2018) 103:1669–77. doi: 10.1210/jc.2017-02477
51. Shyam S, Fatimah A, Rohana AG, Norasyikin AW, Karuthan C, Shanita N, et al. Lowering dietary glycaemic index through nutrition education among Malaysian women with a history of gestational diabetes mellitus. Malays J Nutr. (2013) 19:9–24.
52. Ghani RA, Shyam S, Arshad F, Wahab NA, Chinna K, Safii NS, et al. The influence of fasting insulin level in post-gestational diabetes mellitus women receiving low-glycaemic-index diets. Nutr Diabetes (2014) 4:e107. doi: 10.1038/nutd.2014.5
53. Schmidt MI, Duncan BB, Castilhos C, Wendland EM, Hallal PC, Schaan BD, et al. Lifestyle INtervention for Diabetes prevention After pregnancy (LINDA-Brasil): study protocol for a multicenter randomized controlled trial. BMC Pregnancy Childbirth (2016) 16:68. doi: 10.1186/s12884-016-0851-x
54. Chasan-Taber L, Marcus BH, Rosal MC, Tucker KL, Hartman SJ, Pekow P, et al. Estudio Parto: postpartum diabetes prevention program for hispanic women with abnormal glucose tolerance in pregnancy: a randomised controlled trial - study protocol. BMC Pregnancy Childbirth (2014) 14:100. doi: 10.1186/1471-2393-14-100
55. Clinical Trials,.gov. Identifier NCT03559621. Melinda Pilot Study (MELINDA). Bethesda, MD: National Library of Medicine (2018). Available online at: https://clinicaltrials.gov/ct2/show/NCT03559621?term=NCT03559621&rank=1
56. ClinicalTrials.gov. Identifier NCT02744300. Balance After Baby Intervention for Women with Recent Gestational Diabetes (BABI2). Bethesda, MD: National Library of Medicine (2016). Available online at: https://clinicaltrials.gov/ct2/show/NCT02744300?term=NCT02744300&rank=1
Keywords: diabetes, gestational, diabetes mellitus, life style, primary prevention, women
Citation: Goveia P, Cañon-Montañez W, Santos DP, Lopes GW, Ma RCW, Duncan BB, Ziegelman PK and Schmidt MI (2018) Lifestyle Intervention for the Prevention of Diabetes in Women With Previous Gestational Diabetes Mellitus: A Systematic Review and Meta-Analysis. Front. Endocrinol. 9:583. doi: 10.3389/fendo.2018.00583
Received: 29 June 2018; Accepted: 14 September 2018;
Published: 05 October 2018.
Edited by:
Wei Bao, University of Iowa, United StatesReviewed by:
Aaron Hanukoglu, Tel Aviv University, IsraelJoseph Aloi, Wake Forest Baptist Medical Center, United States
Copyright © 2018 Goveia, Cañon-Montañez, Santos, Lopes, Ma, Duncan, Ziegelman and Schmidt. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Pâmella Goveia, cGFtZWxsYWdvdmVpYUBnbWFpbC5jb20=