
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
REVIEW article
Front. Cardiovasc. Med. , 06 November 2019
Sec. Structural Interventional Cardiology
Volume 6 - 2019 | https://doi.org/10.3389/fcvm.2019.00161
This article is part of the Research Topic Percutaneous Mitral Valve Interventions (Repair): Current Indications and Future Perspectives View all 10 articles
 Antonio Mangieri1*Alessandra Laricchia1Francesco Giannini1Francesco Gallo1Faraj Kargoli2Annamaria Ladanyi2,3Luca Testa4Antonio Colombo1Azeem Latib2,5
Antonio Mangieri1*Alessandra Laricchia1Francesco Giannini1Francesco Gallo1Faraj Kargoli2Annamaria Ladanyi2,3Luca Testa4Antonio Colombo1Azeem Latib2,5Mitral regurgitation (MR) is a common disease affecting more than 4 million people in the United States and the European Union. A significant number of percutaneous valves have been developed recently, specifically designed for the mitral anatomy, and with a promising evidence of good procedural and echocardiographic outcomes. However, even if transcatheter mitral valve replacement (TMVR) will have a role in the future of percutaneous treatment of both functional and degenerative mitral regurgitation, percutaneous mitral valve repair will always play a vital role in the treatment of MR because of the favorable safety profile and the fact that it respects the native anatomy. In this review, we will discuss the new emerging technologies under development to treat mitral regurgitation focusing on different devices that aim to target different components of the mitral anatomy.
Mitral regurgitation (MR) affects more than 4 million people in the United States and the European Union and its prevalence increases with age, reaching up to 1 in 10 adults aged 75 years or older (1, 2). Degenerative MR (DMR) accounts for approximately one-third of all MR cases (3). Today, surgical mitral valve repair (MVr) is a robust and effective procedure to correct MR, with years of clinical experience and validated evidence. However, surgical mitral intervention in high risk patients is still a challenging procedure, with 30-day mortality approaching 3.1% (4). Furthermore, the mortality rate is even higher in patients with functional mitral regurgitation (FMR), where a concomitant impairment of the left ventricular ejection fraction (LVEF) is often observed (5).
For these reasons, emerging low risk percutaneous strategies are needed to treat MR in both degenerative and functional anatomies, and to minimize the potential complications associated with open-heart surgery. Percutaneous MVr technologies are required to replicate surgical mitral valve reconstruction, without disrupting the normal valve and ventricular physiology. In this review, we will discuss the potential future role of percutaneous MVr, offering an overview on the emerging technologies that are currently under investigation.
A variety of repair techniques (including mitral leaflet devices, implantation of neochords and percutaneous mitral annuloplasty) has been introduced since the first MitraClip procedure in 2003. However, in most of these cases, emerging technologies have been dismissed because of suboptimal pre-clinical results, complicated implants, and difficult reproducibility of their results. The development of transcatheter MVr systems is facing the following challenges:
1) The degree of MR reduction with percutaneous repair technologies is not fully predictable, and a complete resolution is rarely guaranteed.
2) Mitral valve anatomy is complex and different mechanisms can contribute to regurgitation. As a consequence, a single repair device addressing a single target will unlikely achieve optimal results. For example, a certain degree of mitral annular dilatation is always present in patients suffering from severe MR. Surgical MVr usually combines various types of leaflet-plasty with annular reduction in order to minimize the risk of progressive annular enlargement and MR recurrence (6). On the contrary, percutaneous MVr procedures are often based on a single repair technique and are consequently considered “incomplete.” The lack of knowledge on the long-term outcomes in these circumstances gives rise to concerns about the durability of MR reduction. Isolated published case reports show the feasibility of simultaneous implantation of MitraClip (Abbott Laboratories, Abbott Park, IL) and Cardioband (Edwards Lifesciences Corp., Irvine, CA, USA) as well as “rescue” percutaneous annuloplasty to treat MR recurrence after Mitraclip (7, 8). However, these still remain anecdotal cases and more data are needed.
3) The mitral annulus is a highly dynamic, asymmetrical structure, with a saddle-shape conformation that poses difficulties in the positioning and sizing of these devices. Therefore, the development of percutaneous annuloplasty systems has to overcome major design obstacles due to the aforementioned complex mitral annular structure. A circular prosthetic ring runs the risk of not matching the asymmetrical anatomy of the native mitral valve annulus, thus increasing the tension between the device and the mitral structure. This limitation along with the method of fixation (screws) could translate into an increased risk of late device detachment, which has already been observed in the early cases of percutaneous mitral annuloplasty (9).
4) A certain proportion of mitral anatomies are not the ideal candidates for repair and sometimes TMVR can be an alternative treatment option. Nevertheless, calcific and rheumatic MR still represent important unmet needs in transcatheter mitral intervention that may be associated with suboptimal results, both for repair (increased risk of post-procedural gradients) and replacement (due to the increased risk of para-valvular leakage and left ventricular outflow tract obstruction).
Taking into consideration the aforementioned challenges, a significant number of percutaneous valves have been recently developed, specifically designed for the mitral anatomy, and with promising evidence of good procedural and echocardiographic outcomes. However, even if TMVR will have a definite role in the future of percutaneous treatment of both FMR and DMR, percutaneous MVr will always play a vital role in the treatment of MR due to the following:
1) Technical aspects: Transcatheter valves and percutaneous annuloplasty devices have to adapt to the mitral annulus that, conversely to the fibrous ring of the aortic valve, does not provide a rigid anchor for sealing. Moreover, the mitral annulus is posteriorly embedded in the junction of the left atrium and left ventricle, while the anterior portion consists of the aorto-mitral curtain, a dynamic structure with limited rigidity. This poses multiple challenges for securing a device and bares the risk of compression and interference with the aortic valve apparatus. Data from the preliminary experience of these devices demonstrates that the risk of complications like valve erosion, migration, malposition at 1-year follow-up is around 4% (10). These complications theoretically do not exist in the case of MVr.
The close proximity of the left ventricular outflow tract (LVOT) places it at a higher risk for obstruction, especially with high-profile valves. In one study on the early experience with TMVR, the rate of acute LVOT obstruction was 8.2% with transcatheter mitral valve-in-ring (ViR) procedures, and 9.3% following TMVR in the presence of severe mitral annular calcification (MAC) (11, 12). Acute LVOT obstruction has a negative impact on both, procedural and post-procedural outcomes. A neo-LVOT area of <1.7 cm2 is highly predictive of obstruction, and patients with this anatomy should be considered for MVr rather than replacement (13). LVOT obstruction is not a problem with percutaneous MVr, since the devices implemented for percutaneous mitral valve plasty are much smaller in size, and have a favorable profile that respects the mitral valve anatomy.
Lastly, the anatomical position of the mitral valve apparatus can be easily reached through a transapical approach. However, in sick patients with low ejection fraction, the presence of apical scar, and thinning of the apical wall are deleterious, thus an alternative access would be preferable to minimize the risk of complications. A fully percutaneous transfemoral trans-septal venous approach would be desirable but, in comparison to MVr, it would imply larger iatrogenic interatrial defects and it would require a highly flexible delivery system to coaxially reach the mitral valve plane (14).
2) Durability: Although no long-term durability data exist for TMVR, we know from surgery that structural valve degeneration occurs more frequently in mitral bioprosthetic valves than in the aortic valves, and in younger individuals (15). From our clinical experience we also learned that patients undergoing TMVR are younger and have a longer life expectancy compared to transcatheter aortic valve implantation (TAVI) patients. All these reasons raise the alarms regarding the long-term durability of these valves. Conversely, the devices used for MVr can potentially last for decades without a concrete risk of erosion or degeneration.
3) Device thrombosis: TMVR prostheses are potentially more prone to thrombosis due to the larger size, the high profile and the huge amount of “foreign” material of which they are made. Moreover, the atrial aspect of the mitral prostheses is exposed to low atrial pressures that can contribute to blood stasis, and subsequently to valve thrombosis. The early experience in 100 patients reported a device thrombosis rate of 6% at 1-year (16). Conversely, percutaneous MVr is more physiological as the implanted device is not as bulky as TMVR and the smaller surface area can mitigate the risk of device thrombosis.
4) Paravalvular Leak (PVL): Paravalvular leak (PVL) is a common complication of mitral valve replacement (15). Although most PVLs have unknown clinical significance, ~3% of patients will have signs and symptoms of hemolysis, heart failure or a combination of the two (17). Significant PVL is relatively rare in cases of TMVR in non-calcified mitral annuli, while in cases of TMVR in MAC, the rate of moderate to severe PVL at 30 days can reach up to 13.8% (18). In MVr the risk of PVL leading to hemolysis is theoretically non-existent.
MR is the most frequent valve disease in the population and it's prevalence increases with age (19). Open-heart surgery is considered the gold standard for the treatment of severe MR, with excellent outcomes achievable in most patients. However, more than 50% of patients with severe MR are excluded from surgery due to an increased perioperative risk related to comorbidities (20). In particular, patients with FMR, have a high perioperative mortality ranging between 6.6 and 11.4% (21). Whereas, the use of an effective percutaneous MVr system can result in a lower perioperative risk with similar clinical benefits compared to surgery at follow-up. Lastly, we hypothesize that the number of future percutaneous mitral valve procedures will be influenced by the following factors:
- The results of the recently published COAPT and MITRA-FR trials have demonstrated that moderate to severe FMR has a clear clinical impact on prognosis, and a successful treatment of FMR with the MitraClip system in selected patients can significantly reduce the rate of rehospitalization, and all-cause mortality at 2-years follow-up (22, 23).
- The prevalence of heart failure will increase by ~50% between 2012 and 2030, resulting in more than 8 million people older than 18 years-old with heart failure. This daunting future reflects the increased prevalence of heart failure as the population ages, and the improved survival of patients with acute myocardial infarction and heart failure itself. In parallel, this progressive increase of heart failure prevalence will translate into a higher rate of MR. Hence, percutaneous treatments to fix MR will be necessary given the high surgical risk profile of this population (24).
- In the near future, the threshold for percutaneous treatment of multiple valvular diseases will be lowered. TAVI has already been demonstrated to be non-inferior or even superior to surgical aortic valve replacement in low risk patients. Percutaneous treatment of concomitant significant MR in this population will be considered a desirable option (25, 26).
- The armamentarium of devices for the treatment of MR will expand, offering a wide number of percutaneous options that will be able to accommodate a larger variety of anatomies.
A wide number of MVr systems are currently under development (Figure 1). The following section provides a brief overview of these devices and of the ongoing clinical studies on transcatheter mitral valve repair (Table 1).
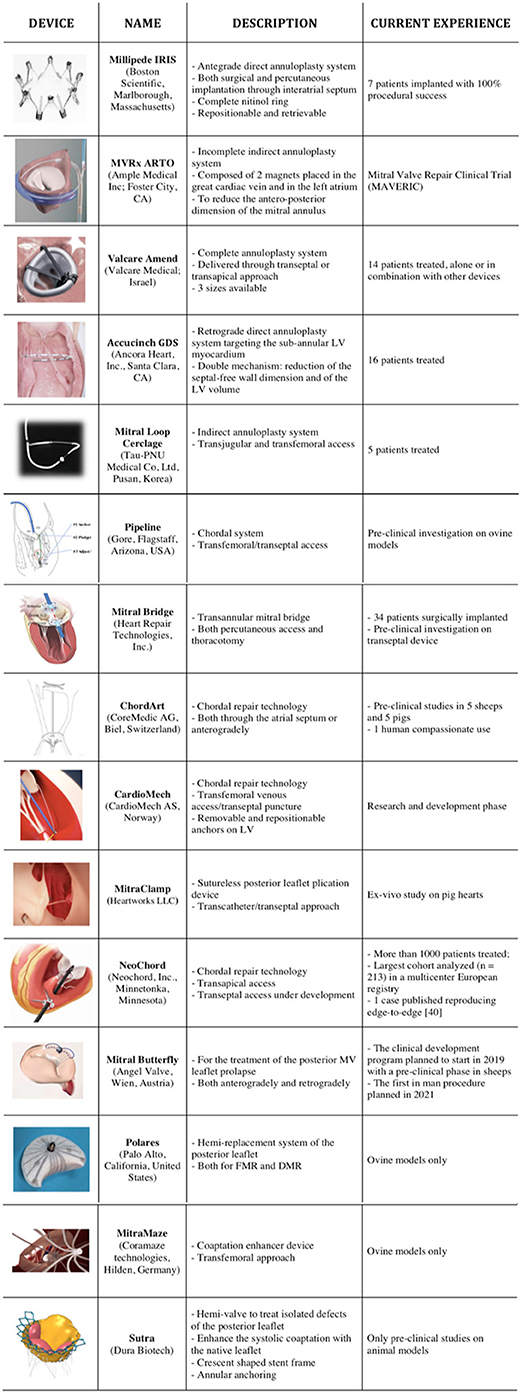
Figure 1. List of the emerging repair technologies available for mitral valve.
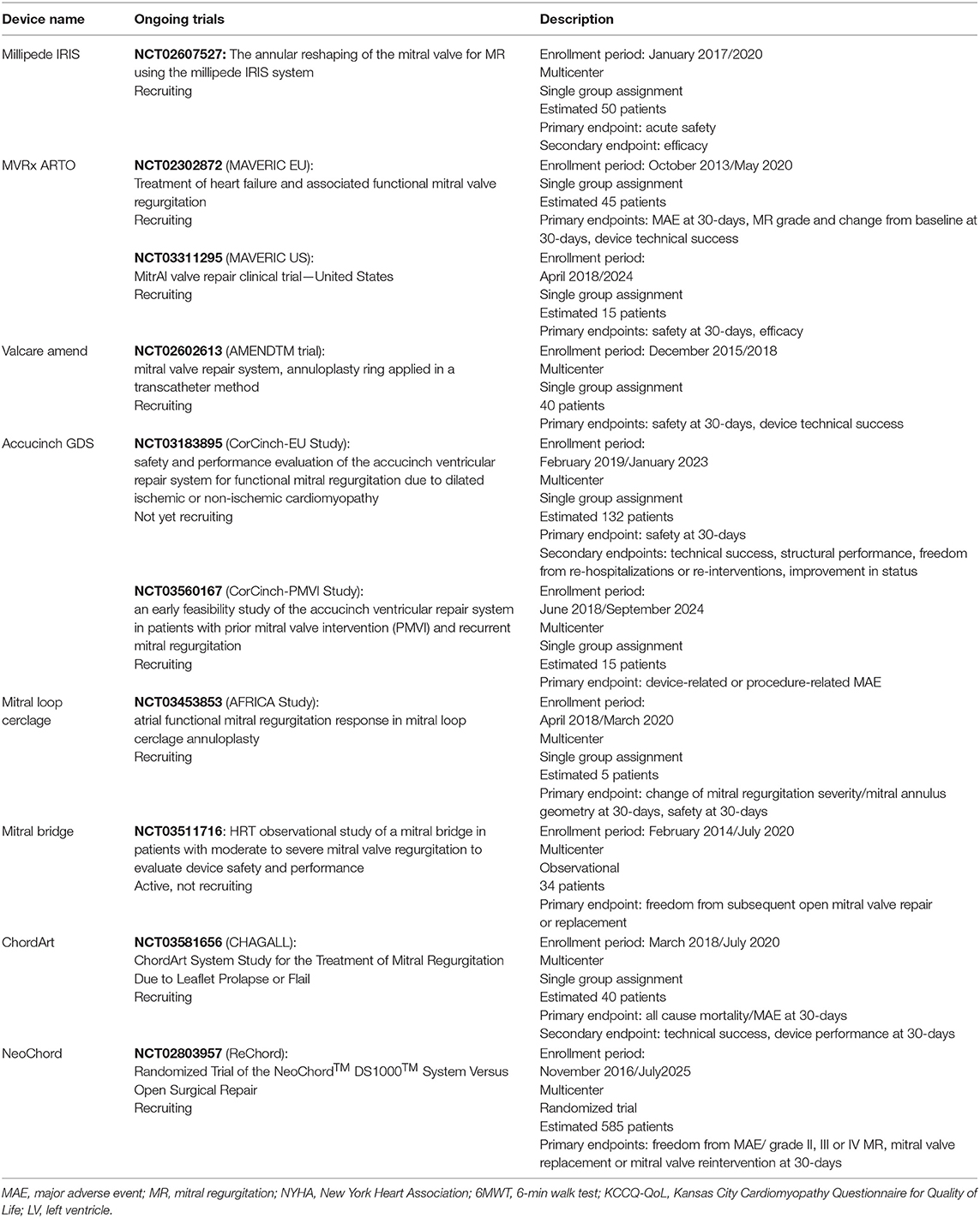
Table 1. Ongoing trials for each mitral valve repair system.
The Millipede IRIS is a complete, semi-rigid annuloplasty ring (Boston Scientific, Marlborough, Massachusetts). The system is composed of eight stainless-steel anchors that are connected by sliding collars and nitinol frames, located in the upper position of the device. Each anchor can be independently and reversibly fixed to the mitral tissue in order to customize the size and the site of anchoring. The Millipede IRIS has been implanted both surgically, using a trans-atrial approach, and percutaneously, with a 24 French steerable catheter delivered trans-septally. The first clinical experience with IRIS included seven patients: four were treated using a conventional surgical approach, while three patients were treated percutaneously. The percutaneous implant of the device was monitored under fluoroscopy and using both transesophageal and intracardial ultrasound (ICE) monitoring. The adjunctive use of ICE allowed a direct visualization of the mitral annulus and a detailed placement of the IRIS anchors. All the iatrogenic atrial septal defects were closed with a 10 mm Amplatzer septal occluders (Abbott, Santa Clara, CA). The authors reported no major adverse events and a procedural success obtained in all the cases. The implant resulted in a significant reduction in the septo-lateral diameter (from 38.0 ± 4.1 to 25.9 ± 4.9 mm), and in a significant reverse remodeling of the left ventricle, with a decrease in diastolic left ventricular volumes from 182.4 ± 54.3 to 115.3 ± 98.8 mL at 30 days. Every patient demonstrated reduction of MR, with all patients showing a decline from a baseline of 3 or 4+ MR to 0 or 1+ MR at 30 days (27). One of the patients who received a surgical implantation of the IRIS Millipede in combination with an A2/P2 Alfieri leaflet repair, performed in standard fashion, experienced a relapse of MR at 12 months follow-up due to a newly ruptured chordae tendineae, just lateral to the original Alfieri stitch. In this patient, an adjunctive MitraClip was placed with a residual trivial MR (28).
The Annular Reshaping of the Mitral Valve for MR Using the Millipede IRIS System (NCT02607527) is an early feasibility clinical trial with the aim of enrolling 50 patients with symptomatic severe MR treated percutaneously with the IRIS device.
The MVRx ARTO (Ample Medical Inc.; Foster City, CA) is an incomplete and indirect annuloplasty system. The system is composed of two magnets (MagneCath) that are placed in the great cardiac vein and in the left atrium at the level of A2/P2 scallops. Once the two magnets are close to each-other, a specific guidewire is passed through the two MagneCath from the great cardiac vein to the left atrium, aligning the two catheters. After using an exchange catheter, the loop guidewire is placed across left atrium. This guidewire directs the placement of the great cardiac vein anchor (T-bar) and septal anchor. Once in place, an appropriate tension is applied to reduce the antero-posterior dimension of the mitral annulus. The results of the Mitral Valve Repair Clinical Trial (MAVERIC) have been published, where the authors reported the 30-days outcome of 11 patients that were treated with the MVRx ARTO system. Effective regurgitant orifice area decreased from 30.3 ± 11.1 to 13.5 ± 7.1 mm2, and regurgitant volumes from 45.4 ± 15.0 to 19.5 ± 10.2 ml. The mitral annular anteroposterior diameter decreased from 45.0 ± 3.3 to 38.7 ± 3.0 mm. One patient had pericardial effusion, and one asymptomatic device dislodgment were reported at 30-days, with no other major adverse events (29). To evaluate the safety and efficacy of this system in patients with MR secondary to annular dilatation, the MAVERIC EU (NCT02302872) and the MAVERIC US (NCT03311295) clinical trials are recruiting 45 and 15 patients in Europe and the United States, respectively. A total of 45 patients have been recruited in both trials with 1-year echocardiographic follow-up available in 35 patients. The authors report a significant reduction of the mitral annular dimensions from 41.4 to 35.3 mm, sustained at 1-year, with a freedom from residual moderate MR obtained in 92% of patients. At the follow-up, 11.4% of patients died for cardiovascular reasons, with no device malfunctioning reported (30).
Valcare Amend system (Valcare Medical; Israel) is a complete, semi-rigid D-shaped percutaneous annuloplasty system. The ring is available in three sizes to fit a wide range of mitral annular dimensions (29–50 mm). Once in place, the ring is delivered starting from the posterior part of the annulus. The annuloplasty ring is designed to be delivered through a transseptal or a trans-apical approach. This annuloplasty system has been tested in different scenarios and in combination with other therapies. A total of 14 patients have been treated in the first clinical experience: eight patients with FMR have received Valcare Amend as a single therapy. Whereas, two patients with DMR have received Valcare Amend as a single therapy. In another four patients, the system has been utilized in combination with MitraClip (three patients) and with NeoChord (one patient). The implant resulted in a 74% reduction of the jet area and in a 20% reduction in the antero-posterior diameter (31). In a single case, an unplanned MitraClip was implanted to treat significant residual mitral regurgitation. The Mitral Valve Repair System, Annuloplasty Ring Applied in a Transcatheter Method (AMENDTM trial, NCT02602613) is currently recruiting with a target sample size of 40 patients to evaluate the efficacy and safety of the device.
The Accucinch GDS device (Ancora Heart, Inc., Santa Clara, CA) is a direct ventriculoplasty system targeting the sub-annular left ventricular myocardium. The system includes a delivery catheter, a modular guide tunnel (MGT), an anchor delivery catheter and 12–16 nitinol anchors, connected by an ultra-high molecular weight polyethylene cinch cable to exercise tension over them. Proximal and distal anchors are interspaced with nitinol force distribution members. The system is implanted retrogradely using an 18 French guiding catheter delivered through the aortic valve. The Accucinch GDS implant can be customized according to the sub-annular space anatomy and to the thickness of the left ventricular wall. Anchors are delivered from commissure to commissure through an arch beneath the posterior leaflet of the MV in the ventricular free wall. Once the system has reached the sub-annular space, the MGT is oriented in direction of the myocardium and gradually withdrawn to facilitate anchor delivery through an inner tunnel with a single window. Once all the anchors have been released, tension is applied to the cinch cable using the cinch and lock catheter. A cut catheter is then utilized to cut the cinch cable before removing the MGT and the guide catheter (32). Thanks to the implantation site, the Accucinch GDS device acts with a double mechanism; it reduces the septal-free wall dimension, drawing the papillary muscles and the mitral leaflets in close proximity, and reduces the left ventricle volume without extracting muscle. Compared to the first implants, the latest version of the device is more flexible. Moreover, to achieve a greater volumetric reduction, the target zone now includes a wider part of left ventricular free wall. The Accucinch GDS has been attempted in 16 patients with two failures due to anatomical constraints and impossibility to achieve an adequate position of the delivery catheter. Among 14 successful implants, one procedure was complicated by pericardial effusion and stroke, that lead to the patient's demise. The 6 month echocardiographic data showed a significant reduction of the mitral regurgitant volume (from 60 to 37 ml) together with a sustained reduction of the left ventricular end-systolic volume (from 119 to 72 ml), with a continuous trend toward a progressive reverse remodeling of the left ventricle. The efficacy and safety of the device is under investigation in different scenarios (33). TheCorCinch-EU Study (NCT03183895) is an international multicenter, non-randomized, prospective safety study, designed to evaluate the AccuCinch Ventricular Repair System for the treatment of heart failure, with or without FMR due to dilated ischemic or non-ischemic cardiomyopathy. The Early Feasibility Study of the AccuCinch Ventricular Repair System in Patients With Prior Mitral Valve Intervention (PMVI) and Recurrent Mitral Regurgitation (The CorCinch-PMVI Study, NCT03560167) is actively recruiting, with target sample size of 15 patients with recurrent MR after failure of the previous valve intervention.
The Transmural System Transcatheter Mitral Cerclage Annuloplasty (Tau-PNU Medical Co. Ltd., Pusan, Korea) is an indirect annuloplasty system composed of a stainless steel tension element with a coronary artery protection system. The two extremities of the tension element are connected using a bridge device that extends to the left subclavian vein. An adjustable extravascular lock is fixed subcutaneously in the subclavicular fossa and has the function to connect the tension element and the bridge, thus allowing a modulation of the tension under echocardiographic monitoring (34).
The procedure is performed using both the transjugular and transfemoral approach. Once the coronary sinus has been engaged, a pressurized venogram is performed to identify a perforator vein suitable for the intervention. A guidewire is then advanced in the perforator vein and externalized into the right ventricular outflow tract, passing through the interventricular septum. The externalized guidewire is then snared and pulled back into the inferior vein cava. The guidewire is subsequently exchanged with the Mitral Loop Tension device that is deployed with a protection device, to prevent the extrinsic compression of the circumflex artery. Once the tension device is in situ, the bifid coronary sinus tricuspid valve bridge is placed to prevent any damage of the septal tricuspid leaflet and of the conduction system. The first in human experience with the mitral loop cerclage annuloplasty was successful in 4 of 5 attempts. The mitral regurgitant volume and the septo-lateral mitral annular diameter were significantly reduced at 6 months (54 ± 8–18.5 ± 4.1 ml and 41.5–34.2 mm, respectively). The implantation of the mitral Cerclage also lead to a reduction of the left ventricular end diastolic volume (140 ± 62.5–102.6 ± 35.7 ml) (35). The Atrial Functional Mitral Regurgitation Response In Mitral Loop Cerclage Annuloplasty (AFRICA Study, NCT03453853) is a prospective, single-center, open label, feasibility study to assess the safety and efficacy of the Mitral Loop Cerclage Annuloplasty in treating FMR associated with heart failure and atrial fibrillation.
The Pipeline system (Gore, Flagstaff, Arizona, USA) is a newly developed system that targets the sub-annular apparatus, and acts as a chordal system that can be implanted using a transfemoral trans-septal approach. Once the delivery catheter reaches the left ventricle, a ventricular anchor is deployed from the catheter and fixed to the free wall, leaving a ventricular suture attached to the ventricular anchor. A leaflet pledget is deployed to secure the mitral valve leaflet to the ventricular anchor. The leaflet suture is secured to the ventricular anchor to limit the excursion the leaflet. This technology is currently under pre-clinical investigation with mid-term ovine models showing the feasibility of the procedure.
Mitral Bridge (Heart Repair Technologies, Morgan Hill, CA, USA) is a newly developed technology that consists in a curvilinear nitinol band covered by a silicone overmold with velour pads at either extremity. The Mitral Bridge is positioned transversely across the mitral valve, linking the anterior and the posterior leaflets at the level of A2-P2 segments, thus reducing the antero-posterior annular dimensions. A delivery handle, preattached to the implant, assists in positioning the bridge on the annulus with the curvature facing the ventricular cavity. Five septal-laterally oriented sizes of the mitral bridge (22, 24, 26, 28, and 30 mm) are available. The initial experience included 34 patients enrolled in the observational study of the Heart Repair Technologies Mitral Bridge in Treating Mitral Valve Regurgitation (NCT03511716), who received a surgical implant of the Mitral Bridge. At 2 years, no strokes or device-related adverse events were noted, and the MR was reduced from 3.32 ± 0.47 to 0.50 ± 0.83 (P < 0.001), with <1+ MR in 33/34 patients (including four reinterventions for periprosthetic recurrent MR ≥3 without mitral bridge explants or conventional mitral repair or replacement). At 2 years, the mean mitral gradient was 2.15 ± 0.82 mmHg, and the mitral annular septo-lateral dimension decreased from 40.4 ± 2.91 to 28.9 ± 1.55 mm (36).
The ChordArt (CoreMedic AG, Biel, Switzerland) is a fully percutaneous transcatheter mitral chordae implantation system, which can be delivered through the transtrially or transfemorally via the trans-septal approach. ChordArt uses a dedicated delivery catheter that grasps the mitral leaflet in the target area that needs to be treated. Once grasped, the delivery system is passed through the punctured leaflet until it reaches the papillary muscle. Once at the level of the papillary muscle, an anchor located at the distal tip of the catheter is fixed into the muscle. After this maneuver, the delivery system is retrieved leaving a suture that connects the grasped leaflet and the subvalvular apparatus. Pre-clinical studies have evaluated the safety and the efficacy of the system, surgically implanted in the beating heart of five sheep with acute chordal rupture; all procedures were successful and all of the five animal models were alive at 6 months follow-up, with no evidence of disruption or malfunction of the device. The ChordArt system has been subsequently implanted also in five pigs with acute mitral valve chordal rupture. The device has been implanted under fluoroscopy and echocardiographic guidance using left thoracotomy, with direct access through the left atrium on a beating heart. After the positive first in human experience for compassionate use, the device performance and the technical efficacy of ChordArt is currently under investigation in the ChordArt System for Mitral Regurgitation trial (CHAGALL, NCT03581656) with the planned enrollment of 40 patients suffering from a flail or prolapsed mitral valve leaflet (37).
CardioMech (CardioMech AS, Norway) is a transcatheter mitral valve chordal repair technology designed for the treatment of DMR due to prolapsed or flail leaflets. It is still in the research and developmental phase. It requires a transfemoral venous access and a transseptal puncture to reach the left atrium. The device is advanced through a 24Fr steerable delivery catheter to grip the prolapsing leaflet, then the new chordae is attached from the leaflet to the ventricular wall, where an anchor fixes it. Anchors are removable and repositionable. Studies to assess safety and feasibility are needed.
MitraClamp (Heartworks LLC) is a new sutureless leaflet plication device designed for treating patients with mitral leaflet prolapse through a transcatheter approach. The U-shape arms are able to rotate around a common axis. Following leaflet grasping, leaflet plication is performed by rotating the two arms in two opposite ways. Pre-clinical study on the application of the MitraClamp in six fresh pig hearts demonstrated a dramatic reduction of the regurgitant volume during hydrodynamic tests. Device anchorage to leaflets was also found to be stable after device locking (38).
The NeoChord Artificial Chordae Delivery System (Neochord, Inc., Minnetonka, Minnesota) is a transcatheter MVr technology performed through a transapical access (a transseptal access system is still under development). Under general anesthesia and transesophageal echo guidance, it allows the placement of expanded polytetrafluoroethylene (e-PTFE) sutures as replacement neochordae on a beating heart, without the need for cardiopulmonary bypass (39).
A relatively short learning curve is needed to achieve expertise in performing the NeoChord procedure safely (40). This contributed to the successful European experience and to the diffusion of the procedure so that, since its first application, more than 1,000 patients have been treated (41, 42). As for conventional surgery, the ideal candidates for NeoChord implantation are patients with isolated central posterior leaflet prolapse or flail, and patients with posterior multi-segment involvement. On the contrary, treating more complex lesions, such as those involving the anterior leaflet and paracommissural or calcified leaflets, has worse outcomes (43). Another predictor of success after NeoChord implantation is the Leaflet-to-Annulus Index (LAI), which is the ratio between the sum of the anterior leaflet length and the posterior leaflet length over the antero-posterior length. LAI values of ≤1.35, 1.30, and 1.25 are a positive prognostic predictor of residual regurgitation at 3, 6 months, and 1 year, respectively (44). According to these measurements, it is estimated that ~25–30% of patients presenting with DMR can be effectively treated with the NeoChord procedure (40). To expand its application, one possibility is the synergic combination of this device with other transcatheter MVr systems, mimicking what already currently occurs with surgery. Otherwise, the group of Colli described another interesting application of the technique, as they reproduced the edge-to-edge intervention directly through transapical neochordal implantation with satisfactory results (45).
A currently ongoing multicenter, randomized trial (NCT02803957) comparing the NeoChord procedure with conventional surgical MVr in the United States will help provide further insights on the procedure.
The mitral Butterfly system (Angel Valve, Wien, Austria) aims to reproduce the butterfly repair technique for the treatment of the posterior MV leaflet prolapse. The butterfly repair consists of the combination of a triangular resection from the prolapsing edge, with a reverse triangular resection to the annulus to remove redundancy (46). The Butterfly system consists of a nitinol stent with PTFE yarns and a swing arm that mimics an artificial papillary muscle. The implant can be performed both anterogradely and retrogradely using a steerable catheter. Once released, the Butterfly system contains the prolapsing posterior segment through the PTFE yarns; the position is stabilized thanks to the swing arm. The clinical development program (cOntaining prolapsing Segments to Correct mitral Regurgitation–OSCAR) is planned to start in 2019, and contemplate a first pre-clinical phase in sheep with the first in man procedure is planned in 2021 (47).
The Polares (Palo Alto, CA, USA) solution is a new concept in the vast armamentarium of mitral valve transcatheter technologies, it is a halfway between repair and replacement. It consists of the implantation of a posterior ePTFE neoleaflet to restore coaptation with the valve's native anterior leaflet. The development of this technology still needs to undergo clinical testing. To this date, implantation has been only performed in animal models.
The MitraMaze system (Coramaze Technologies, Hilden, Germany) is a coaptation enhancer device composed of a flexible spacer, a nitinol crown and a customized delivery catheter system, which is specifically designed for the transfemoral approach. Upon release on site in the beating heart, the self-expanding implant design allows for an atraumatic anchoring in the left atrium, without the need to include adjacent myocardial tissue structures. A nitinol crown is left in the atrium and the spacer can be filled to reduce the coaptation gap between the mitral leaflets. In ovine models, the MitraMaze has demonstrated a significant reduction of the regurgitant volume (48).
The Sutra (Dura Biotech) hemi-valve has been studied to specifically treat MR secondary to an isolated defect of the posterior mitral valve leaflet. The hemi-valve is composed of a tri-leaflet valve mounted on a crescent shaped stent frame. The hemi-valve is designed to enhance the systolic coaptation with the native leaflets, thus reducing the regurgitation. The hemi-valve is fixed to the posterior annulus through anchors that can be adjusted, thus allowing the possibility to cinch the native valve annulus. The first generation device has been surgically implanted in animals due to the lack of an anchoring system. However, the latest version of the device has been implanted in animals using the anchoring system. The device has demonstrated good safety and efficacy in reducing the regurgitant volume under hydrostatic testing (49).
Percutaneous MVr is a rapidly growing field, with several devices at different stages of development. Due to their capacity to preserve the complex inner anatomy of the mitral valve, these repair systems will have an important role in the treatment of MR. Large clinical cohort studies will help identify the right patient population that would benefit the most from transcatheter MVr. This breakthrough of new repair devices will enlarge the percutaneous armamentarium of MVr, offering a wide possibility of treatments customizable to specific anatomical features.
AM, ALar, FGi, and FGa produced a first draft of the manuscript. FK, ALad, and LT did a review of the literature. AC and ALat reviewed the article and gave their intellectual contribution to the manuscript.
AM received an institutional grant (unrestricted grant) from Boston Scientific; he received a research grant from Innovative Cardiac Solution. FGi serves as proctor for Neovasc, ALat has served on advisory boards for Medtronic and Abbott; and has been a consultant to Edwards Lifesciences.
The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
MVr, mitral valve repair; MR, mitral regurgitation; FMR, functional mitral regurgitation; DMR, degenerative mitral regurgitation; TMVR, transcatheter mitral valve replacement; LVEF, left ventricular ejection fraction; MAC, mitral annular calcification.
1. Nishimura RA, Vahanian A, Eleid MF, Mack MJ. Mitral valve disease–current management and future challenges. Lancet. (2016) 387:1324–34. doi: 10.1016/S0140-6736(16)00558-4
2. De Bonis M, Lapenna E, La Canna G, Ficarra E, Pagliaro M, Torracca L, et al. Mitral valve repair for functional mitral regurgitation in end-stage dilated cardiomyopathy: role of the ‘edge-to-edge' technique. Circulation. (2005) 112(Suppl):I402–8. doi: 10.1161/CIRCULATIONAHA.104.525188
3. Enriquez-Sarano M, Akins C W. Vahanian A. Mitral regurgitation. Lancet. (2009) 373:1382–94. doi: 10.1016/S0140-6736(09)60692-9
4. Seeburger J, Raschpichler M, Garbade J, Davierwala P, Pfannmueller B, Borger MA, et al. Minimally invasive mitral valve surgery in octogenarians-a brief report. Ann Cardiothorac Surg. (2013) 2:765–7. doi: 10.3978/j.issn.2225-319X.2013.10.13
5. Acker MA, Parides MK, Perrault LP, Moskowitz AJ, Gelijns AC, Voisine P, et al. Mitral-valve repair versus replacement for severe ischemic mitral regurgitation. N Engl J Med. (2014) 370:23–32. doi: 10.1056/NEJMoa1312808
6. Maisano F, Caldarola A, Blasio A, De Bonis M, La Canna G, Alfieri O. Midterm results of edge-to-edge mitral valve repair without annuloplasty. J Thorac Cardiovasc Surg. (2003) 126:1987–97. doi: 10.1016/S0022-5223(03)01291-1
7. Mangieri A, Colombo A, Demir OM, Agricola E, Ancona F, Regazzoli D, et al. Percutaneous direct annuloplasty with edge-to-edge technique for mitral regurgitation: replicating a complete surgical mitral repair in a one-step procedure. Can J Cardiol. (2018) 34:1088.e1–e2. doi: 10.1016/j.cjca.2018.04.003
8. Latib A, Ancona MB, Ferri L, Montorfano M, Mangieri A, Regazzoli D, et al. Percutaneous direct annuloplasty with cardioband to treat recurrent mitral regurgitation after mitraclip implantation. JACC Cardiovasc Interv. (2016) 9:e191–2. doi: 10.1016/j.jcin.2016.06.028
9. Messika-Zeitoun D, Nickenig G, Latib A, Kuck KH, Baldus S, Schueler R, et al. Transcatheter mitral valve repair for functional mitral regurgitation using the cardioband system: 1 year outcomes. Eur Heart J. (2019) 40:466–72. doi: 10.1093/eurheartj/ehy424
10. Sorajja P, Moat N, Badhwar V, Walters D, Paone G, Bethea B, et al. Initial feasibility study of a new transcatheter mitral prosthesis. J Am Coll Cardiol. (2019) 73:1250–60. doi: 10.1016/j.jacc.2018.12.066
11. Paradis JM, Del Trigo M, Puri R, Rodés-Cabau J. Transcatheter valve-in-valve and valve-in-ring for treating aortic and mitral surgical prosthetic dysfunction. J Am Coll Cardiol. (2015) 66:2019–37. doi: 10.1016/j.jacc.2015.09.015
12. Guerrero M, Dvir D, Himbert D, Urena M, Eleid M, Wang DD, et al. Transcatheter mitral valve replacement in native mitral valve disease with severe mitral annular calcification. JACC Cardiovasc Interv. (2016) 9:1361–71. doi: 10.1016/j.jcin.2016.09.042
13. Yoon SH, Bleiziffer S, Latib A, Eschenbach L, Ancona M, Vincent F, et al. Predictors of left ventricular outflow tract obstruction after transcatheter mitral valve replacement. JACC Cardiovasc Interv. (2019) 12:182–93. doi: 10.1016/j.jcin.2018.12.001
14. Miura M, Zuber M, Gavazzoni M, Lin SI, Pozzoli A, Taramasso M, et al. Possible left circumflex artery obstruction in a cardioband transcatheter mitral annuloplasty caused by coronary kinking during cinching. JACC Cardiovasc Interv. (2019) 12:600–1. doi: 10.1016/j.jcin.2018.12.039
15. Bloch G, Vouhe PR, Menu P, Poulain H, Cachera JP, Aubry P, et al. Long-term evaluation of bioprosthetic valves: 615 consecutive cases. Euro Heart J. (1984) 5(Suppl D):73–80. doi: 10.1093/eurheartj/5.suppl_D.73
16. Pibarot P, Dumesnil JG. Prosthetic heart valves: selection of the optimal prosthesis and long-term management. Circulation. (2009) 119:1034–48. doi: 10.1161/CIRCULATIONAHA.108.778886
17. Taramasso M, Maisano F, Denti P, Guidotti A, Sticchi A, Pozzoli A, et al. Surgical treatment of paravalvular leak: long-term results in a single-center experience (up to 14 years). J Thorac Cardiovasc Surg. (2015) 149:1270–5. doi: 10.1016/j.jtcvs.2014.12.041
18. Yoon SH, Whisenant BK, Bleiziffer S, Delgado V, Dhoble A, Schofer N, et al. Outcomes of transcatheter mitral valve replacement for degenerated bioprostheses, failed annuloplasty rings, and mitral annular calcification. Euro Heart J. (2019) 40:441–51. doi: 10.1093/eurheartj/ehy590
19. Nkomo VT, Gardin JM, Skelton TN, Gottdiener JS, Scott CG, Enriquez-Sarano M. Burden of valvular heart diseases: a population-based study. Lancet. (2006) 368:1005–11. doi: 10.1016/S0140-6736(06)69208-8
20. Mirabel M, Iung B, Baron G, Messika-Zeitoun D, Détaint D, Vanoverschelde JL, et al. What are the characteristics of patients with severe, symptomatic, mitral regurgitation who are denied surgery? Eur Heart J. (2007) 28:1358–65. doi: 10.1093/eurheartj/ehm001
21. Virk SA, Sriravindrarajah A, Dunn D, Liou K, Wolfenden H, Tan G, et al. A meta-analysis of mitral valve repair versus replacement for ischemic mitral regurgitation. Ann Cardiothorac Surg. (2015) 4:400–10. doi: 10.3978/j.issn.2225-319X.2015.09.06
22. Stone GW, Lindenfeld J, Abraham WT, Kar S, Lim DS, Mishell JM, et al. Transcatheter mitral-valve repair in patients with heart failure. N Engl J Med. (2018) 379:2307–18. doi: 10.1056/NEJMoa1806640
23. Obadia JF, Messika-Zeitoun D, Leurent G, Iung B, Bonnet G, Piriou N, et al. Percutaneous repair or medical treatment for secondary mitral regurgitation. N Engl J Med. (2018) 379:2297–306. doi: 10.1056/NEJMoa1805374
24. Udelson JE, Stevenson LW. The future of heart failure diagnosis, therapy, and management. Circulation. (2016) 133:2671–86. doi: 10.1161/CIRCULATIONAHA.116.023518
25. Mack MJ, Leon MB, Thourani VH, Makkar R, Kodali SK, Russo M, et al. Transcatheter aortic-valve replacement with a balloon-expandable valve in low-risk patients. N Engl J Med. (2019) 380:1695–705. doi: 10.1056/NEJMoa1814052
26. Popma JJ, Deeb GM, Yakubov SJ, Mumtaz M, Gada H, O'Hair D, et al. Transcatheter aortic-valve replacement with a self-expanding valve in low-risk patients. N Engl J Med. (2019) 380:1706–15. doi: 10.1056/NEJMoa1816885
27. Rogers JH, Boyd WD, Smith TW. Early experience with Millipede IRIS transcatheter mitral annuloplasty. Ann Cardiothorac Surg. (2018) 7:780–6. doi: 10.21037/acs.2018.10.05
28. Rogers JH, Boyd WD, Smith TWR, Ebner AA, Bolling SF. Combined mitraclip edge-to-edge repair with millipede iris mitral annuloplasty. JACC Cardiovasc Interv. (2018) 11:323–4. doi: 10.1016/j.jcin.2017.11.007
29. Rogers JH, Thomas M, Morice MC, Narbute I, Zabunova M, Hovasse T, et al. Treatment of heart failure with associated functional mitral regurgitation using the ARTO system: initial results of the first-in-human MAVERIC trial (Mitral Valve Repair Clinical Trial). JACC Cardiovasc Interv. (2015) 8:1095–104. doi: 10.1016/j.jcin.2015.04.012
30. Worthey S. MVRx ARTO System of FMR: Update and Case Presentation. Present Transcatheter Valve Ther 2018. Chicago, IL (2018).
31. Meerkin D. The AMEND Mitral Repair System: Technology and Clinical Updates. Present. CRT 2019. Chicago, IL (2019).
32. Robert G, Meredith IT. The Accucinch transcatheter direct mitral valve annuloplasty. EuroIntervention. (2015) 11:W60–1. doi: 10.4244/EIJV11SWA16
33. Reisman M. AccuCinch Basale Ventricular Repair for Functional MR and Heart Failure: Device, Procedure and Updated Outcomes. Present. Transcatheter Valve Ther 2018. Chicago, IL (2018).
34. Kim JH, Sung SC, Chon MK, Kim JO, Lee SH, Lee SY, et al. Mitral loop cerclage as a variant form of mitral cerclage annuloplasty that adds a device (CSTV) for preventing potential complications: a preclinical proof of concept and feasibility study. EuroIntervention. (2016) 11:e1669–79. doi: 10.4244/EIJV11I14A319
35. Park YH, Chon MK, Lederman RJ, Sung SC, Je HG, Choo KS, et al. Mitral loop cerclage annuloplasty for secondary mitral regurgitation: first human results. JACC Cardiovasc Interv. (2017) 10:597–610. doi: 10.1016/j.jcin.2016.12.282
36. Cerny S, Benesova M, Skalsky I, Patel NC, Subramanian VA. Persistent reduction of mitral regurgitation by implantation of a transannular mitral bridge: durability and effectiveness of the repair at 2 years—results of a prospective trial. Eur J Cardio-Thoracic Surg. (2019) 55:867–73. doi: 10.1093/ejcts/ezy423
37. Weber A. Transcatheter Mitral Chordal Replacement CHORDART. Present Transcatheter Valve Ther 2016. Chicago, IL (2016).
38. Zegdi R. TCT-842 mitraclamp - a new promising device for transcatheter treatment of mitral valve prolapse. J Am Coll Cardiol. (2016) 68:B340. doi: 10.1016/j.jacc.2016.09.871
39. Colli A, Adams D, Fiocco A, Pradegan N, Longinotti L, Nadali M, et al. Transapical NeoChord mitral valve repair. Ann Cardiothorac Surg. (2018) 7:812–20. doi: 10.21037/acs.2018.11.04
40. Holzhey DM, Seeburger J, Misfeld M, Borger MA, Mohr FW. Learning minimally invasive mitral valve surgery: a cumulative sum sequential probability analysis of 3895 operations from a single high-volume center. Circulation. (2013) 128:483–91. doi: 10.1161/CIRCULATIONAHA.112.001402
41. Colli A, Manzan E, Aidietis A, Rucinskas K, Bizzotto E, Besola L, et al. An early European experience with transapical off-pump mitral valve repair with NeoChord implantation. Eur J Cardio-Thoracic Surg. (2018) 54:460–6. doi: 10.1093/ejcts/ezy064
42. Seeburger J, Borger MA, Tschernich H, Leontjev S, Holzhey D, Noack T, et al. Transapical beating heart mitral valve repair. Circ Cardiovasc Interv. (2010) 3:611–2. doi: 10.1161/CIRCINTERVENTIONS.110.957944
43. Colli A, Manzan E, Besola L, Bizzotto E, Fiocco A, Zucchetta F, et al. One-year outcomes after transapical echocardiography-guided mitral valve repair. Circulation. (2018) 138:843–5. doi: 10.1161/CIRCULATIONAHA.118.033509
44. Colli A, Besola L, Montagner M, Azzolina D, Soriani N, Manzan E, et al. Prognostic impact of leaflet-to-annulus index in patients treated with transapical off-pump echo-guided mitral valve repair with NeoChord implantation. Int J Cardiol. (2018) 257:235–7. doi: 10.1016/j.ijcard.2018.01.049
45. Colli A, Besola L, Bizzotto E, Peruzzo P, Pittarello D, Gerosa G. Edge-to-edge mitral valve repair with transapical neochord implantation. J Thorac Cardiovasc Surg. (2018) 156:144–8. doi: 10.1016/j.jtcvs.2018.02.008
46. Asai T, Kinoshita T, Hosoba S, Takashima N, Kambara A, Suzuki T, et al. Butterfly resection is safe and avoids systolic anterior motion in posterior leaflet prolapse repair. Ann Thorac Surg. (2011) 92:2097–03. doi: 10.1016/j.athoracsur.2011.07.087
47. Mohl W. Angel Valve advancing Transcatheter Mitral Valve Repair. Present. PCR Innovators Day 2018. Paris (2018).
Keywords: mitral regurgitation, heart failure, mitral valve, transcatheter mitral valve replacement, mitral annulus
Citation: Mangieri A, Laricchia A, Giannini F, Gallo F, Kargoli F, Ladanyi A, Testa L, Colombo A and Latib A (2019) Emerging Technologies for Percutaneous Mitral Valve Repair. Front. Cardiovasc. Med. 6:161. doi: 10.3389/fcvm.2019.00161
Received: 26 June 2019; Accepted: 21 October 2019;
Published: 06 November 2019.
Edited by:
Maurizio Taramasso, University Hospital Zürich, SwitzerlandReviewed by:
Neil P. Fam, St. Michael's Hospital, CanadaCopyright © 2019 Mangieri, Laricchia, Giannini, Gallo, Kargoli, Ladanyi, Testa, Colombo and Latib. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Antonio Mangieri, antonio.mangieri@gmail.com
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.