
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Cardiovasc. Med. , 05 June 2018
Sec. Structural Interventional Cardiology
Volume 5 - 2018 | https://doi.org/10.3389/fcvm.2018.00063
This article is part of the Research Topic TAVI and The Challenges Ahead View all 13 articles
 Crochan J. O'Sullivan1*
Crochan J. O'Sullivan1* Matteo Montalbetti2Rainer Zbinden1David J. Kurz1Alain M. Bernheim1
Matteo Montalbetti2Rainer Zbinden1David J. Kurz1Alain M. Bernheim1 Aaron Liew3Matthias R. Meyer1David Tüller1Franz R. Eberli1
Aaron Liew3Matthias R. Meyer1David Tüller1Franz R. Eberli1Aim: To assess the accuracy of multi-detector computed tomography (MDCT) derived pulmonary vessel measurements in predicting pulmonary hypertension (PH) among patients with severe symptomatic aortic stenosis (AS) undergoing transcatheter aortic valve implantation (TAVI).
Background: PH is common among patients with severe AS undergoing TAVI and is associated with adverse outcomes. MDCT is the imaging modality of choice to assess anatomical dimensions among patients selected for TAVI.
Methods: One hundred and thirty-nine patients with severe AS undergoing TAVI with both CT scans and right heart catheterizations (RHC) were included. CT diameters of the main pulmonary artery (MPA), right (RPA) and left (LPA), and ascending aorta (AA) were measured. The relationship between CT measurements and PA pressures assessing using RHC was tested with linear regression.
Results: The CT derived ratio of the diameter of the MPA to the diameter of the AA (PA/AAratio) correlated best with mean PA pressure (R2 = 0.48) and PA systolic pressure (R2 = 0.50). Receiver operating characteristic curve analysis showed that the PA/AAratio is a moderate predictor of PH (AUC 0.74, 95% CI 0.65–0.83, p < 0.0001) and that the optimal cut off point is 0.80 (sensitivity 56%, specificity 88%, positive predictive value 95.5%, negative predictive value 30.6% for PH).
Conclusions: Elderly patients with severe AS and PA/AAratio values ≥ 0.80 on MDCT are more likely to have PH but PH cannot be reliably excluded among such patients with lower PA/AAratio values.
Transcatheter aortic valve implantation (TAVI) is a less invasive alternative treatment option to surgical aortic valve replacement (SAVR) among patients with symptomatic severe aortic stenosis (AS) (1). Patients selected for TAVI tend to be inoperable or high risk for conventional SAVR and typically have a high prevalence of co-morbidities including coronary artery disease, atrial fibrillation, concomitant valvular heart disease, and chronic renal failure (2). In addition, pulmonary hypertension (PH) is common among patients with severe AS undergoing TAVI and is associated with worse clinical outcomes as compared with patients without PH (3). The identification of PH prior to TAVI is therefore important for appropriate risk stratification and may help in determining which patients should be selected for TAVI vs. SAVR. Right heart catheterization is the gold standard method for diagnosing PH, which is defined as a mean pulmonary artery pressure ≥25 mmHg (4). However, right heart catheterization is an invasive procedure and is not routinely performed prior to TAVI. Transthoracic echocardiography can provide an estimate of the pulmonary artery systolic pressure but cannot reliably detect whether PH is present or not (5). Multi-detector computed tomography (MDCT) is recommended as the imaging modality of choice prior to TAVI to determine annular and aortic root dimensions as well as iliofemoral anatomy prior to TAVI (6). Whether or not MDCT measurements of the pulmonary vasculature provide a reliable estimate of the presence of PH among patients with severe AS selected for TAVI is unknown. Therefore, the aim of this study was to assess the accuracy of MDCT derived pulmonary vessel measurements in predicting the presence of PH among patients with severe symptomatic AS undergoing TAVI.
This is a retrospective analysis of prospectively collected data within a database that includes all patients with severe AS, who underwent TAVI at our institution between August 2011 and September 2015 (n = 184). All patients were deemed inoperable or at high risk for surgery by a multidisciplinary team consisting of invasive cardiologists and surgeons. Included in the present analysis were all patients with symptomatic severe AS, a full preprocedural right and left heart catheterization and a pre-procedural multidetector computed tomography (MDCT). Data collection was facilitated by using the nation-side prospective TAVI registry (SWISS TAVI Registry) into which all patients from our institution are prospectively enrolled. The cohort study complies with the Declaration of Helsinki, was approved by the local Ethics Committee, and all patients provided informed written consent.
All included patients underwent coronary angiography and right and left heart catheterization for haemodynamic assessment prior to TAVI. Intracardiac pressures were recorded with fluid filled catheters connected to pressure transducers as previously described (7).
(PH) was defined as a mean pulmonary artery pressure ≥ 25 mmHg and was subdivide into pre-capillary PH (left-ventricular end-diastolic pressure ≤ 15 mmHg) and post-capillary PH (LVEDP >15 mmHg). Furthermore, post-capillary PH was further subdivided into isolated post-capillary PH (diastolic pulmonary gradient ≤ 7 mmHg) and combined post- and pre-capillary PH (diastolic pulmonary gradient > 7 mmHg).
TAVI was performed as previously described (7). Vascular access was transfemoral using the Edwards Sapien Valve XT/S3 (ESV, Edwards Lifesciences, Irvine, CA, USA), the Medtronic CoreValve Revalveing System, the Medtronic Evolut R (MCRS; Medtronic Inc., Minneapolis, MN, USA), and the Lotus Valve (Boston Scientific) and transapical for the ESV.
All included patients underwent CT for preinterventional assessment of aortic annulus size and evaluation of vascular access using a second-generation, multidetector 128-slice dual source CT (Somatom Definition Flash, Siements Healthcare, Forchheim, Germany). Images were reviewed on a stationary workstation by an investigator who had no knowledge of any clinical information or the RHC results. Calipers were set for measuring the widest short-axis diameter of the main pulmonary artery within 3 cm of the bifurcation, the right pulmonary artery and left pulmonary artery and the ascending aorta, respectively on axial sections. The diameter of the AA was measured at the level of the MPA.
Continuous data are presented as means ± standard deviations (SD), and categorical variables are depicted as percentages and numbers. Categorical variables were compared by means of the χ2 test (or Fisher's test for two group comparisons), and continuous variables were compared using the unpaired t-test for two groups or ANOVA for 3 or more groups. ROC analysis were performed to assess the AUC and to compare sensitivity and specificity for different cut-off values using the Youden Index. Sensitivity, specificity, negative predictive value (NPV), and positive predictive value (PPV) were calculated and shown in percentages. Time-to-event data are presented using Kaplan-Meier curves, with incidence rates calculated from life-tables at 2-year follow-up. Log-rank test was used to declare significance. A p-value < 0.05 were considered statistically significant. All analyses were performed with SPSS 22, Release 22.0.0.1 or STATA (version 12, StataCorp, College Station, TX, USA).
Baseline characteristics are given in Table 1. A total of 139 patients with symptomatic severe AS undergoing TAVI had complete MDCT and RHC data and were included in the present analysis. Eighty-Two percentage (n = 114) patients had PH defined as a mean PA pressure ≥ 25 mmHg. PH patients comprised 12 patients with precapillary PH, 86 patients with isolated post-capillary PH and 16 patients with combined precapillary and post-capillary PH (Figure 1). Patients with PH were significantly older, had a higher body mass index and had significantly higher surgical risk scores at baseline. In addition, NT-pro-BNP values at baseline were significantly higher among PH patients as compared with no PH patients (Table 1) (p < 0.0001).
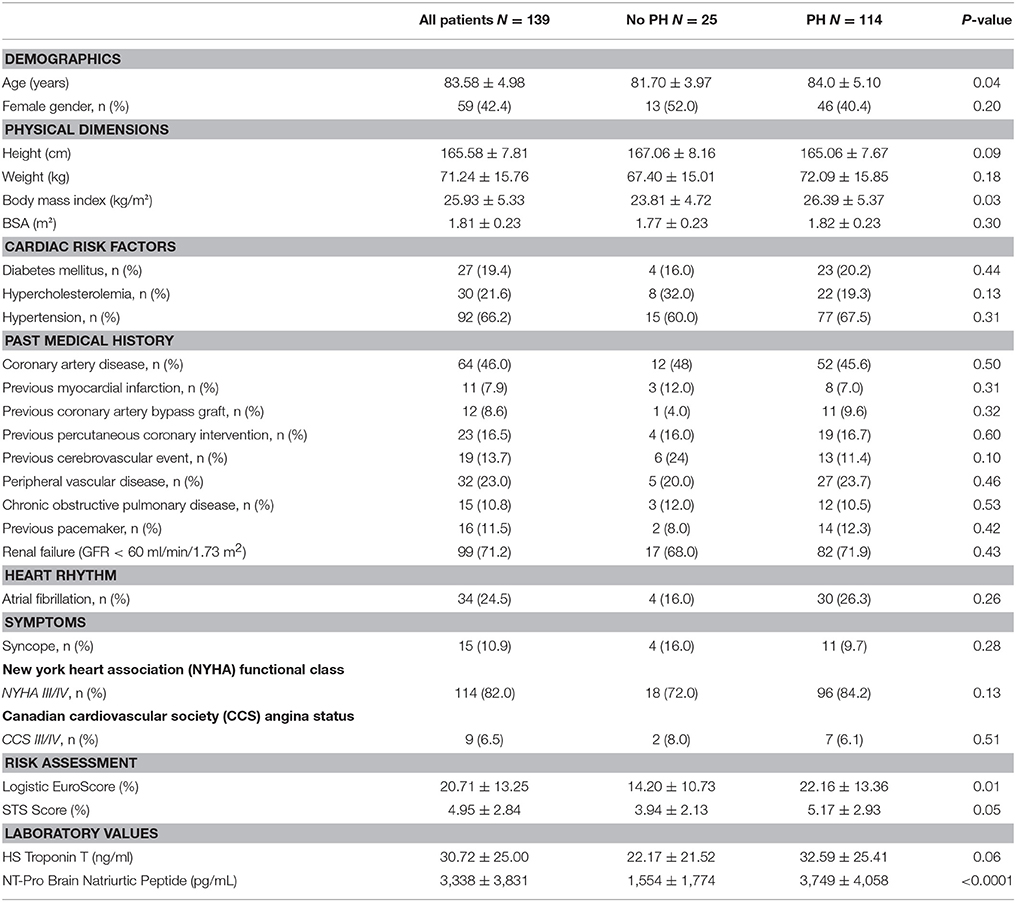
Table 1. Baseline characteristics.
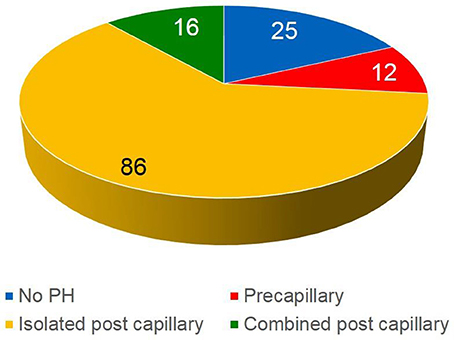
Figure 1. Classification of the patient population (n = 139).
Baseline echocardiographic and invasive haemodynamic characteristics are shown in Tables 2, 3, respectively. As compared with no PH, patients with PH had significantly larger left ventricular end-diastolic diameters (p = 0.026), higher non-invasive right ventricular/right atrial gradients (p = 0.026), higher left ventricular end-diastolic pressures (p = 0.005), higher pulmonary and right ventricular pressures (p < 0.0001) and lower pulmonary artery saturation measurements (p = 0.026).
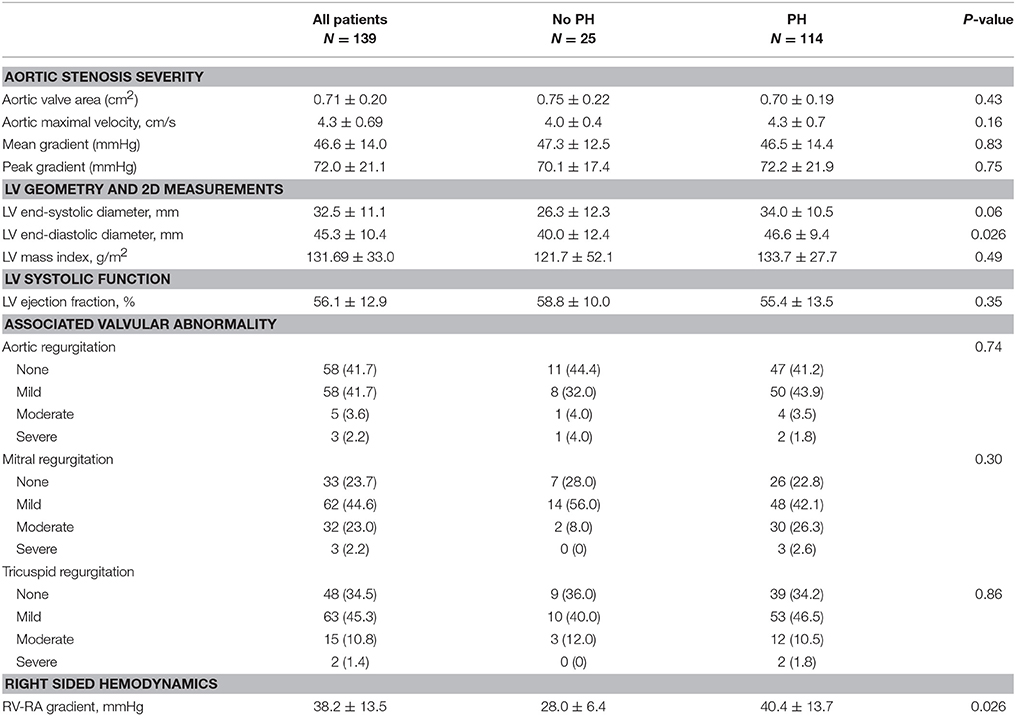
Table 2. Baseline echocardiography characteristics.
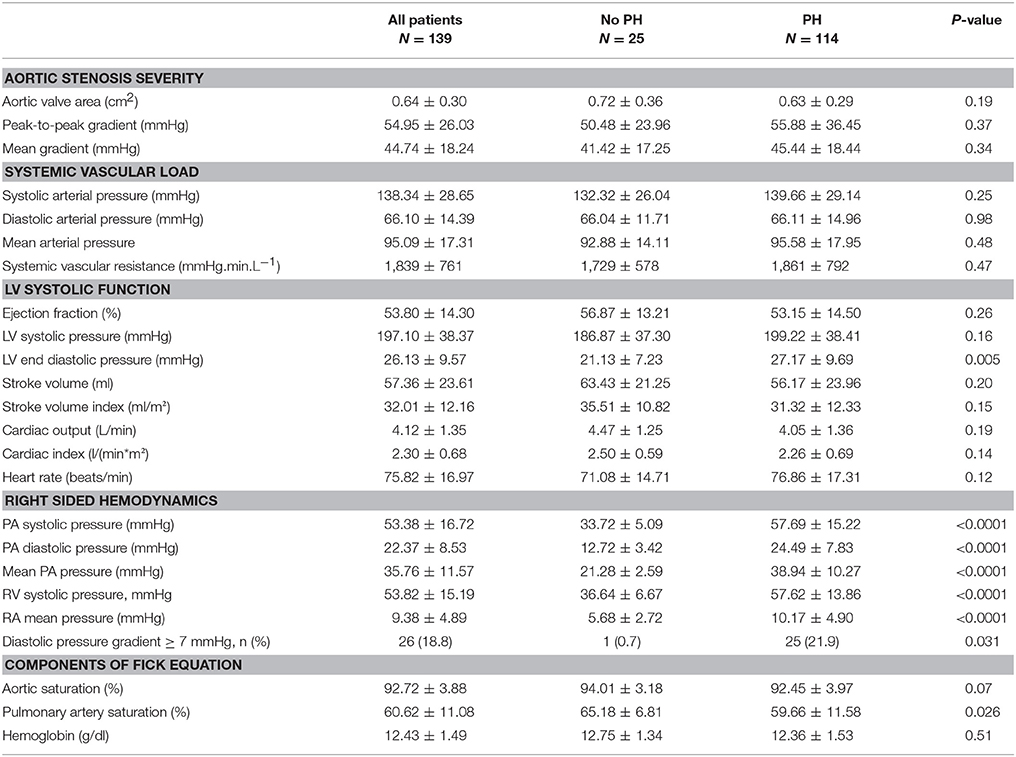
Table 3. Invasive haemodynamic characteristics.
Procedural characteristics are shown in Table 4. The majority of patients underwent TAVI via the transfemoral route (78%) under general anesthesia (91%) with the Edwards SAPIEN 3 valve (35%). Balloon predilatation was performed in most cases (86%) and only a minority of patients underwent concomitant revascularization.
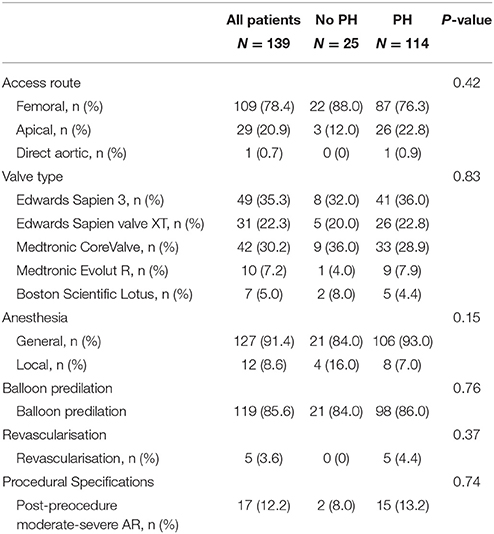
Table 4. Procedural characteristics.
MDCT measurements of the pulmonary and aortic vasculature are shown in Tables 5, 6. As compared with no PH, patients with PH had significantly larger diameters of MPA (p = 0.001), RPA (p = 0.004), LPA (p = 0.029), and PA/AAratio (p < 0.0001). No significant differences in ascending aorta or aortic annular measurements were observed between groups. As compared with no PH, patients with combined post-capillary PH had significantly larger MPA (p = 0.006), RPA (p = 0.011) diameters and PA/AAratio (p < 0.0001) (Supplementary Table 1). In addition, patients with precapillary PH had significantly larger LPA and RPA diameters as compared with patients without PH (supplementary Table 1).
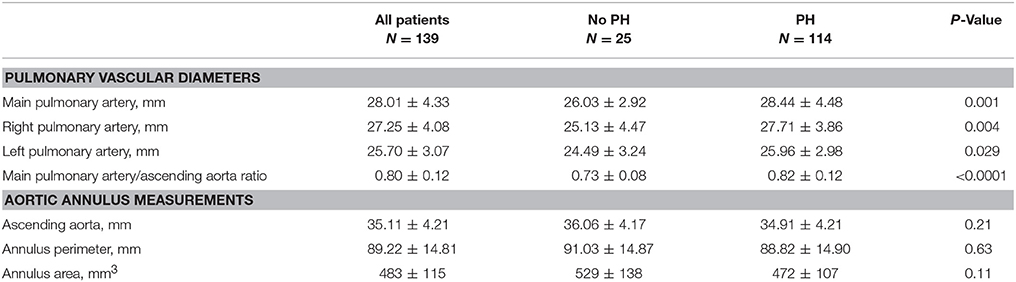
Table 5. Computer Tomography characteristics.
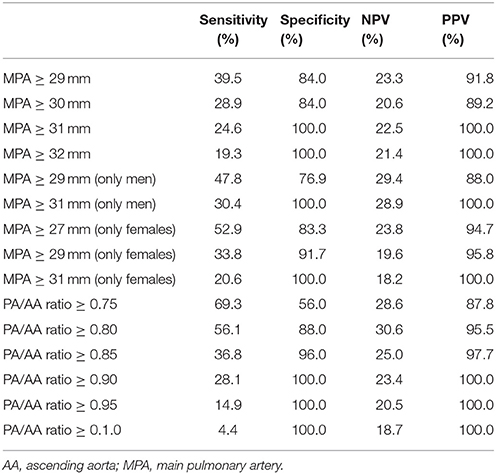
Table 6. Diagnostic accuracy of computed tomography for detecting pulmonary hypertension.
The PA/AAratio exhibited the best correlation with PA pressures (Figure 2) (r2 0.48 for mean PA, p < 0.0001; r2 0.50 for PA systolic pressure, p < 0.0001; r2 0.41 for diastolic PA pressure, p < 0.0001). Using Receiver Operating Characteristic Curves, the PA/AAratio correlated best with PH (AUC 0.74), whereas MPA (AUC 0.65), RPA (AUC 0.67), and LPA (AUC 0.64) exhibited lower sensitivity and specificity (Figure 3). The optimal cut-off point of the PA/AAratio in predicting the presence of PH defined as an invasive mean PA pressure is 0.80 with a sensitivity of 56%, specificity of 88%, negative predictive value of 30.6%, and positive predictive value of 95.5% (Figure 4).
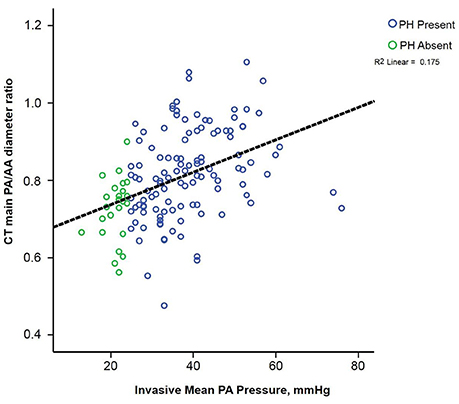
Figure 2. Scatterplot illustrating the correlation between the CT derived pulmonary artery/ascending aorta ratio.
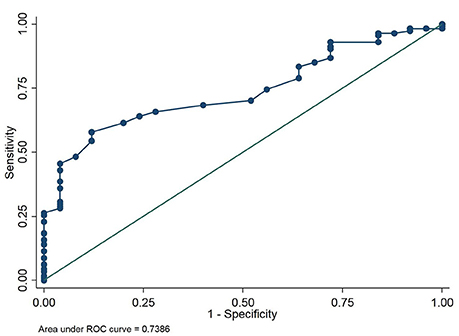
Figure 3. Receiver operating characteristic curve testing the ability of the CT derived pulmonary artery/ascending aorta ratio to detect PH defined as a mean pulmonary artery pressure ≥ 25 mmHg.
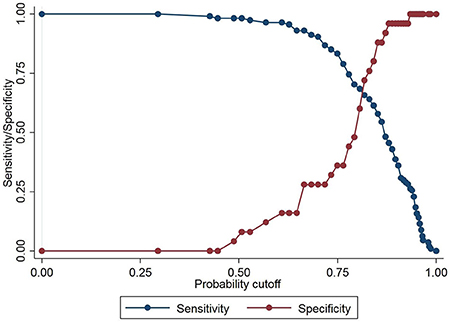
Figure 4. Graph illustrating the best cut-off point for the CT derived pulmonary artery/ascending aorta ratio to detect PH. The best cutoff derived from the Youden index was 0.80.
Clinical outcomes at 30-days and 2-years are shown in Table 7. As compared with no PH, no significant differences in all-cause mortality (Hazard Ratio 0.80, 95% confidence interval 0.18–3.60, p = 0.77) or cardiovascular mortality (HR 4.29, 95% CI 0.60–30.45, p = 0.11) were observed at 2 years among patients with PH (Figure 5). In addition, no significant differences in other VARC-2 endpoints (cerebrovascular accidents, major bleeding, vascular complications, acute renal failure, and permanent pacemaker implantation) were observed between groups at 30-days or 2 years (Table 7).
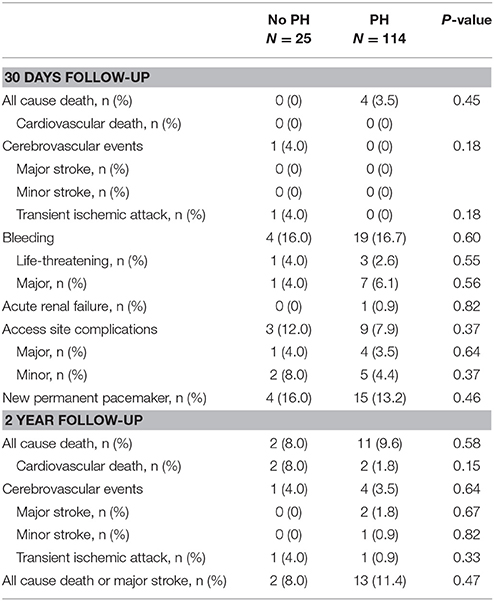
Table 7. Clinical outcomes.
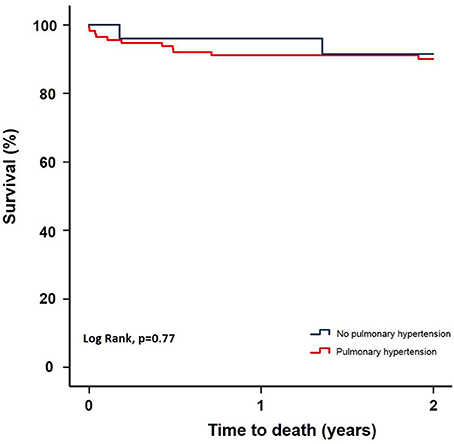
Figure 5. Kaplan-Meier survival curve for patients with and without PH.
In the present study we sought to assess the reliability of screening for PH using MDCT derived measurements of the pulmonary arteries as compared with gold standard pulmonary artery pressure measurements derived from right heart catheterization among patients with severe AS undergoing TAVI. The key finding was that PA/AAratio was the most useful parameter to use to screen for PH among patients with severe AS undergoing TAVI with moderate to high specificity but relatively low sensitivity. We found that the best PA/AAratio cutoff for screening for PH is 0.80. Therefore, patients with a larger PA/AAratio on CT are more likely to have PH (high positive predictive value) but PH cannot be reliably ruled out among patients with smaller PA/AAratio values (low negative predictive value). PH is common among patients with severe AS selected for TAVI and is associated with worse clinical outcomes as compared with patients without PH (3, 8–10). Right heart catheterization is the gold standard method for diagnosing PH but is not routinely performed prior to TAVI. Conversely, MDCT is almost always performed prior to TAVI in order to assess aortic annular and vascular dimensions for procedural planning (6). Consequently, MDCT may serve as a useful screening tool for the presence of PH among patients selected to undergo TAVI and help with risk stratification.
Truong et al. determined the age and sex specific distribution and normal reference values for main pulmonary artery diameter and the PA/AAratio by CT in an asymptomatic community-based population (n = 3,171, mean age 51 ± 10 years) (11). The investigators observed the 90th percentile cutoff value for PA/AAratio was 0.90 for both males and females but that the PA/AAratio was inversely proportional to age (11). The authors observed that that the PA/AAratio was smaller in older participants owing to progressive aortic enlargement with increasing age (11). In the present study, the mean age of the study sample was 84 ± 5 years and this may account for the fact that we observed a smaller PA/AAratio of 0.80 to be the optimal predictor of PH. Prior studies in younger patients with more heterogeneous diseases have suggested that a PA/AAratio ≥ 1.0 is the optimal cutoff point to diagnose PH on CT. A small retrospective study (n = 50, median age 47.5 years) found that a PA/AAratio > 1.0 was the best predictor of chronic pulmonary arterial hypertension with a sensitivity, specificity and positive and negative predictive values for PH of 70, 92, 96, and 52% (12). Similary, Sanal et al. observed in a retrospective study among patients with pulmonary embolism (mean age 59 ± 15 years) that a PA/AAratio ≥ 1.0 had a 59% sensitivity, 82% specificity, a 55% positive predictive value, and a 84% negative predictive value for diagnosing moderate to severe PH defined as a pulmonary artery systolic pressure ≥ 50 mmHg on Doppler Echo (13). Mohamed Hoesein et al. (14) assessed the accuracy of CT PA diameter and PA/AAratio for PH in end-stage COPD among 92 patients (mean age 55 years) and found that a PA/AAratio >1 had a negative predictive value of 77.9% and a positive predictive value of 63.1%. However, the results of the present study would suggest that in an elderly patient population, such as those selected to undergo TAVI, a PA/AAratio ≥ 1.0 would not be sensitive enough as we observed a sensitivity of just 4.4% when PA/AAratio ≥ 1.0 was used to predict the presence of PH. Therefore, the key observation of this study is that a lower PA/AAratio value is required to screen for PH among TAVI patients. To date only one other study assessed the value of CT pulmonary vascular measurements as a predictor of PH and mortality in symptomatic severe AS (15). In contrast to the present study, the authors did not observe that PA/AAratio was any better at predicting PH as compared with MPA. The reasons for this are unclear but may relate to the fact that the pulmonary artery measurements may have been made during end-systole rather than end-diastole. The investigators also did not find any significant differences between MPA diameters of patients with combined post-and pre-capillary PH and no PH, whereas we observed significant differences between these groups (15).
The present study is a single center retrospective study with several limitations. Although we observed no significant differences in adverse clinical outcomes between patients with and without PH no definitive conclusions on the effect of PH on mortality can be drawn from this study as too few events occured. However, the main aim of this study was not to compare clinical outcomes between patients with and without PH, but rather to assess the accuracy of CT measurements of the pulmonary vessels in predicting the presence of PH. The presented conclusions are preliminary and only hypothesis generating and that further research is needed. Further studies should test whether we are able to diagnose different severities of PH, since the implications of severe PH are completely different from mild.
In the present study we found that PA/AAratio demonstrates the strongest correlation with mean PA and PA systolic pressures and that the optimal cutoff is 0.80 in predicting the presence of PH with high specificity but moderate to low sensitivity.
CO, MM, RZ, DK, and FE: conception and design of the study. CO and MM: analysis and interpretation of data. CO: drafting of the manuscript. All authors revising the manuscript critically for important intellectual content and final approval of the manuscript submitted.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fcvm.2018.00063/full#supplementary-material
1. Mack MJ, Leon MB, Smith CR, Miller DC, Moses JW, Tuzcu EM, et al. PARTNER 1 trial investigators. Lancet (2015) 385:2477–84. doi: 10.1016/S0140-6736(15)60308-7
2. O'Sullivan CJ, Wenaweser P. Optimizing clinical outcomes of transcatheter aortic valve implantation patients with comorbidities. Expert Rev Cardiovasc Ther. (2015) 13:1419–32. doi: 10.1586/14779072.2015.1102056
3. O'Sullivan CJ, Wenaweser P, Ceylan O, Rat-Wirtzler J, Stortecky S, Heg D, et al. Effect of pulmonary hypertension hemodynamic presentation on clinical outcomes in patients with severe symptomatic aortic valve stenosis undergoing transcatheter aortic valve implantation. Circ Cardiovasc Interv. (2015) 8:e002358. doi: 10.1161/CIRCINTERVENTIONS.114.002358
4. Vachiery JL, Adir Y, Barbera JA, Champion H, Coghlan JG, Cottin V, et al. Pulmonary hypertension due to left heart diseases. J Am Coll Cardiol. (2013) 62(25 Suppl.):D100–08. doi: 10.1016/j.jacc.2013.10.033
5. Simonneau G, Gatzoulis MA, Adatia I, Celermajer D, Denton C, Ghofrani A, et al. Updated clinical classification of pulmonary hypertension. J Am Coll Cardiol. (2013) 62(25 Suppl.):D34–41. doi: 10.1016/j.jacc.2013.10.029
6. O'Sullivan CJ, Stortecky S, Buellesfeld L, Wenaweser P, Windecker S. Preinterventional screening of the TAVI patient: how to choose the suitable patient and the best procedure. Clin Res Cardiol. (2014) 103:259–74. doi: 10.1007/s00392-014-0676-4
7. O'Sullivan CJ, Stortecky S, Heg D, Pilgrim T, Hosek N, Buellesfeld L, et al. Clinical outcomes of patients with low-flow, low-gradient, severe aortic stenosis and either preserved or reduced ejection fraction undergoing transcatheter aortic valve implantation. Eur Heart J. (2013) 34:3437–50. doi: 10.1093/eurheartj/eht408
8. Lucon A, Oger E, Bedossa M, Bolulmier D, Verhoye JP, Eltchaninoff H, et al. Prognostic implications of pulmonary hypertension in patients with severe aortic stenosis undergoing transcatheter aortic valve implantation: study from the FRANCE 2 Registry. Circ Cardiovasc Interv. (2014) 7:240–7. doi: 10.1161/CIRCINTERVENTIONS.113.000482
9. Ben-Dor I, Goldstein SA, Pichard AD, Satler LF, Maluenda G, Li Y, et al. Clinical profile, prognostic implication, and response to treatment of pulmonary hypertension in patients with severe aortic stenosis. Am J Cardiol. (2011) 107:1046–51. doi: 10.1016/j.amjcard.2010.11.031
10. Tamburino C, Capodanno D, Ramondo A, Petronio AS, Ettori F, Santoro G, et al. Incidence and predictors of early and late mortality after transcatheter aortic valve implantation in 663 patients with severe aortic stenosis. Circulation (2011) 123:299–08. doi: 10.1161/CIRCULATIONAHA.110.946533
11. Truong QA, Massaro JM, Rogers IS, Mahabadi AA, Kriegel MF, Fox CS, et al. Reference values for normal pulmonary artery dimensions by noncontrast cardiac computed tomography: the Framingham heart study. Circ Cardiovasc Imaging (2012) 5:147–54. doi: 10.1161/CIRCIMAGING.111.968610
12. Ng CS, Wells AU, Padley SPG. A CT sign of chronic pulmonary arterial hypertension: the ratio of main pulmonary artery to aortic diameter. J Thor Imaging (1999) 14:270–78.
13. Sanal S, Aronow SW, Ravipati G, Maguire GP, Belkin RN, Lehrman SG. Prediction of moderate or severe pulmonary hypertension by main pulmonary artery diameter and main pulmonary artery diameter/ascending aorta diameter in pulmonary embolism. Cardiol Rev. (2006) 14:213–14. doi: 10.1097/01.crd.0000181619.87084.8b
14. Mohamed Hoesein FA, Besselink T, Pompe E, Oudijk EJ, de Graaf EA, Kwakkel-van Erp JM, et al. Accuracy of CT pulmonary artery diameter for pulmonary hypertension in end-stage COPD. Lung (2016) 194:813–19. doi: 10.1007/s00408-016-9926-8
15. Eberhard M, Mastalerz M, Pavicevic J, Frauenfelder T, Nietlispach F, Maisano F, et al. Value of CT signs and measurements as a predictor of pulmonary hypertension and mortality in symptomatic severe aortic valve stenosis. Int J Cardiovasc Imaging (2017) 33:1637–51. doi: 10.1007/s10554-017-1180-5
Keywords: aortic stenosis, pulmonary hypertension, computed tomography, right heart catheterization, hemodynamics, transcatheter aortic valve implantation
Citation: O'Sullivan CJ, Montalbetti M, Zbinden R, Kurz DJ, Bernheim AM, Liew A, Meyer MR, Tüller D and Eberli FR (2018) Screening For Pulmonary Hypertension With Multidetector Computed Tomography Among Patients With Severe Aortic Stenosis Undergoing Transcatheter Aortic Valve Implantation. Front. Cardiovasc. Med. 5:63. doi: 10.3389/fcvm.2018.00063
Received: 15 February 2018; Accepted: 16 May 2018;
Published: 05 June 2018.
Edited by:
Fabien Praz, Universitätsspital Bern, SwitzerlandReviewed by:
Pablo Codner, Rabin Medical Center, IsraelCopyright © 2018 O'Sullivan, Montalbetti, Zbinden, Kurz, Bernheim, Liew, Meyer, Tüller and Eberli. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Crochan J. O'Sullivan, Y3Jvc3VsbGl2YW5AaG90bWFpbC5jb20=
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.