 Andrea Martinez Gonzalez
Andrea Martinez Gonzalez Tobias Reynolds-Tylus
Tobias Reynolds-Tylus Diana Galarreta-Aima
Diana Galarreta-Aima Carlos G. Alemán
Carlos G. Alemán- 1School of Communication Studies, James Madison University, Harrisonburg, VA, United States
- 2Department of Foreign Languages, Literatures, and Cultures, James Madison University, Harrisonburg, VA, United States
Introduction: COVID-19 disproportionally affects U.S. Hispanic and Latinx individuals. Guided by the Health Belief Model, we examined COVID-19 beliefs among Hispanic and Latinx adults in Virginia.
Method: Respondents (n = 414) were Hispanic and/or Latinx adults in Virginia recruited via Qualtrics panel between May and September 2021. Approximately two-thirds completed the survey in English (63.0%), and one-third completed the survey in Spanish (37.0%).
Results: Most respondents self-reported as vaccinated (72%). Vaccinated respondents reported greater perceived severity and susceptibility to COVID-19 than unvaccinated respondents. Perceived benefits and barriers to vaccination were identified among vaccinated and unvaccinated respondents, respectively. Among unvaccinated respondents, self-efficacy was greater for individuals who planned to get vaccinated compared with those who did not or were unsure. For cues-to-action, vaccinated and unvaccinated respondents identified credible sources and channels for COVID-19 information.
Conclusion: Our results highlight several opportunities and challenges to promoting COVID-19 awareness and vaccination among Hispanic and Latinx adults.
Despite their ethnic diversity, U.S. Hispanic and Latinx individuals are disproportionally affected by COVID-19, revealing deeply rooted health disparities (Macias Gil et al., 2020; Obinna, 2021). The risk of morbidity, mortality, and hospitalization is higher among Hispanic Americans than non-Hispanic Whites (Centers for Disease Control Prevention, 2021) due to such social determinants of health as low socioeconomic status, more limited health care access, language barriers, and occupational exposure (Macias Gil et al., 2020; Obinna, 2021). Given these disparities and the emergence of new COVID-19 variants, there is a need to better understand COVID-19 beliefs among U.S. Hispanic and Latinx populations.
Guided by the Health Belief Model (HBM; Rosenstock, 1974), the current study examined COVID-19 beliefs among Hispanic and Latinx adults in Virginia. The HBM is one of the most widely used theories for understanding health beliefs and behavior (Skinner et al., 2015), including COVID-19 (Wong et al., 2020; Mercadante and Law, 2021). The HBM assumes that to take protective action from a health-related threat (e.g., COVID-19). Individuals must believe they are at risk for a condition with potentially serious consequences, and that a recommended course of action provides some benefit and is feasible to do (Skinner et al., 2015). Below, we review the major components of the HBM and the research questions examined in the current study.
The Health Belief Model
The HBM consists of six major constructs: (a) perceived susceptibility, (b) perceived severity, (c) perceived benefits, (d) perceived barriers, (e) self-efficacy, and (f) cues-to-action (Skinner et al., 2015). Perceived susceptibility refers to an individual's perception that they are personally at risk for experiencing a disease or condition. Perceived severity refers to an individual's perception that the disease or condition could have serious consequences. The current study asked Hispanic and Latinx adults about their perceived susceptibility (i.e., perceived risk of contracting COVID-19) and perceived severity (i.e., perceived negative consequences of contracting COVID-19). We also examined differences in perceptions of severity and susceptibility among vaccinated vs. unvaccinated individuals.
Perceived benefits refer to beliefs about the positive aspects of a recommended action. For example, commonly cited reasons for getting vaccinated include the desire to protect loved ones and vulnerable populations (African American Research Collaborative, 2021). Perceived barriers refer to perceptions of possible obstacles to action, including negative consequences of the recommended action. For example, commonly cited barriers against COVID-19 vaccination include concerns about vaccine safety and efficacy (Wong et al., 2020). In the current study, we asked Hispanic and Latinx adults who had been vaccinated why they decided to get vaccinated (i.e., perceived benefits). Among those who had not yet been vaccinated, we asked their perceptions of the obstacles and negative consequences of vaccination (i.e., perceived barriers).
Self-efficacy refers to an individual's perceived confidence that they can perform a recommended action (Bandura, 1977). Self-efficacy is a critical determinant of health behavior (Sheeran et al., 2016). We asked unvaccinated Hispanic and Latinx adults about their perceptions of self-efficacy (i.e., how confident they felt in getting vaccinated). We also examined differences in self-efficacy among those unvaccinated respondents who said they planned to get vaccinated, those who did not, and those who were unsure.
Finally, cues-to-action refer to internal or external factors that can promote a health behavior. Cues-to-action can be internal (e.g., personally experiencing COVID-19) or external (e.g., media campaigns, verbal persuasion from a family member). Following past research (Williamson et al., 2017), we focused on asking what sources and channels do Hispanic and Latinx adults view as credible for COVID-19 information? We also examined differences between vaccinated and unvaccinated respondents on which sources and channels they found credible.
Altogether, our main research question asked what HBM variables are associated with Hispanic and Latinx adults' COVID-19 vaccination decisions? See Table 1 for a list of HBM constructs defined and operationalized for our study, as well as a list of research questions related to each HBM variable.
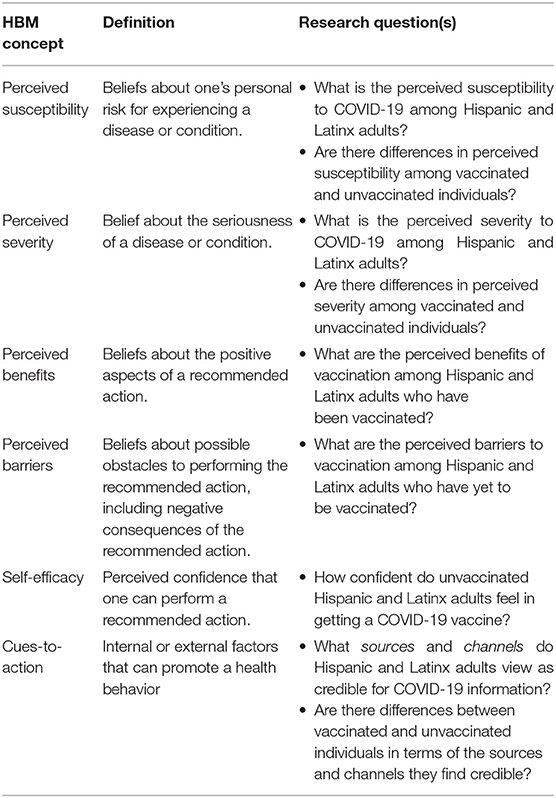
Table 1. Health belief model concepts, definitions, and study research questions.
Method
After receiving approval from the James Madison University Institutional Review Board (IRB), adult respondents (n = 414) in Virginia were recruited via a Qualtrics panel to take one 15-min online Qualtrics survey (including demographic, vaccine status, and health belief questions) between May and September 2021. Sampling was purposive and consisted of respondents who were 18 years of age or older, Virginia residents, and individuals who identified as Hispanic and/or Latinx. Respondents self-identified along several categories of racial background and ethnic heritage. For this reason, we use both “Hispanic” and “Latinx” throughout this report to denote the diversity of heritage and inclusivity of respondent identities. The cost per respondent was $11.
Respondents ranged in age from 18 to 79. Their mean (M) age was 31.35 years (standard deviation [SD] = 12.57 years). Most respondents identified as female (54.6%), followed by male (43.7%), and non-binary (1.7%). Approximately two-thirds completed the survey in English (63.0%), and one-third completed it in Spanish (37.0%). For most respondents, the primary language spoken inside the home was English (58.5%), followed by Spanish (41.5%). Most self-reported as vaccinated (72%). Among the 28% who self-reported as unvaccinated, roughly equal amounts said they planned to get vaccinated (31.9%), did not plan to get vaccinated (33.6%), or were unsure (34.5%).
Measures
The way the survey flow was designed, respondents first self-identified their vaccinated status (if they were vaccinated or unvaccinated). Respondents who said they were unvaccinated were additionally asked if they intended to get vaccinated (yes, no, unsure). Respondents' vaccination status determined which questions they saw in the survey flow. All vaccinated respondents were presented with a list of perceived benefits and asked to select all that applied. All unvaccinated respondents were presented with a list of perceived barriers and were asked to select all that applied. For severity, susceptibility, cues-to-action, and demographics, respondents all viewed the same questions. All measures were adapted from previous studies and CDC guides, and all demographic questions were adapted from the U.S. Census or developed internally for the study's purpose.
Perceived Susceptibility
Perceived susceptibility was measured on a 5-point (1 = strongly disagree to 5 = strongly agree) Likert scale with four items (e.g., “I am at risk for contracting COVID-19;” α = 0.84; M = 3.43, SD = 1.03) adapted from Paek (2016).
Perceived Severity
Perceived severity was measured on a 5-point (1 = strongly disagree to 5 = strongly agree) Likert scale with four items (e.g., “I believe COVID-19 is a serious issue;” α = 0.90; M = 4.21, SD = 1.00) adapted from Paek (2016).
Perceived Benefits
Vaccinated respondents (n = 298) were asked the following question: “Which of the following are reasons why you decided to get a COVID-19 vaccine? Select all that apply.” See Table 2 for a complete list of response options adapted from the CDC's Reasons to Vaccinate guide (Centers for Disease Control Prevention, 2016).
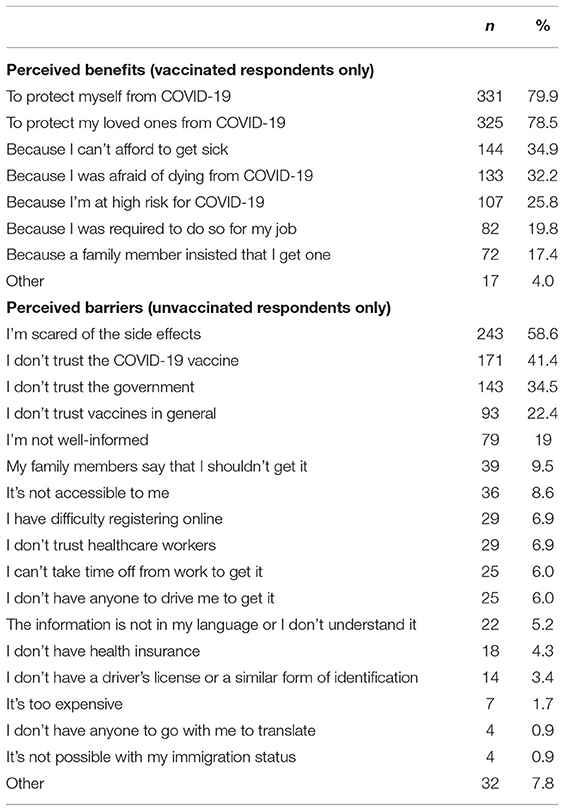
Table 2. Perceived benefits and barriers of vaccination.
Perceived Barriers
Unvaccinated respondents (n = 116) were asked the following question: “Which of the following do you think could make it difficult for you to get a COVID- 19 vaccine? Select all that apply.” See Table 2 for a complete list of response options adapted from Fisk (2021).
Self-Efficacy
Self-efficacy was assessed among unvaccinated respondents on a 5-point (1 = strongly disagree to 5 = strongly agree) Likert scale with three items (“Getting a COVID-19 vaccine is something I am able to do;” α = 0.84; M = 3.53, SD = 1.04) adapted from Witte (1994).
Cues-to-Action
Cues-to-action were conceptualized as credible sources and channels for COVID-19 information (Williamson et al., 2017). For credible sources, respondents were asked: “Who do you think is a credible source on the topic of COVID-19? Select all that apply” For channels, respondents were asked: “Where do you tend to get most of your COVID-19 information from? Select all that apply.” See Table 3 for a complete list of response options.
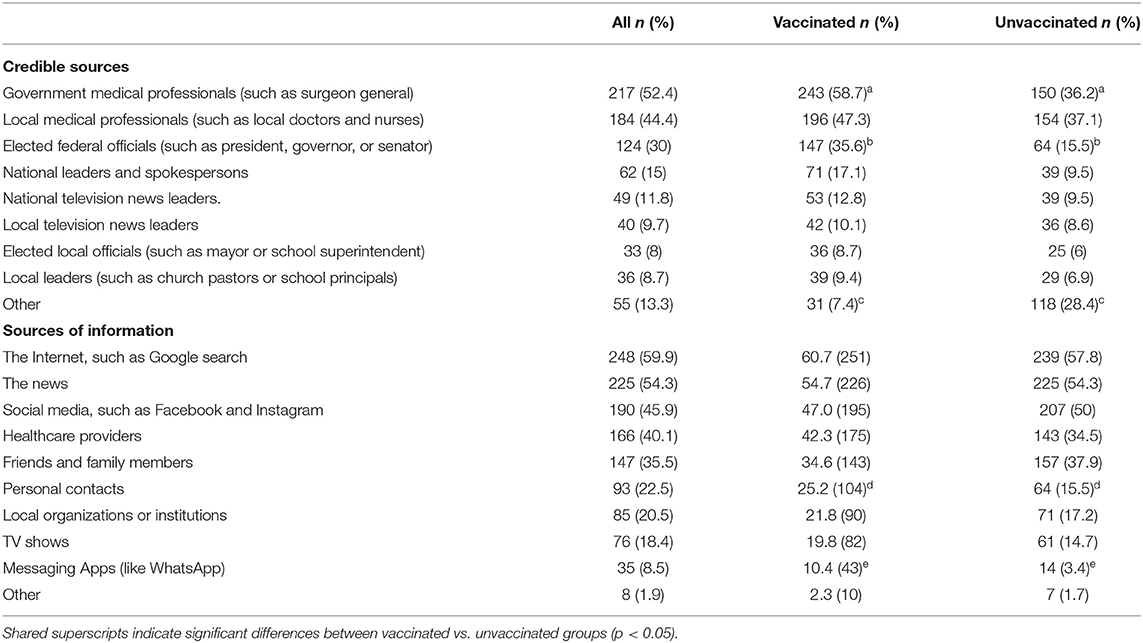
Table 3. Cues-to-action (source and channel).
Demographics
Demographic questions included age, gender, ethnicity, language spoken in and outside the home, vaccination status, and vaccination plans.
Data Analysis
Study analyses were primarily descriptive with use of inferential tests to examine differences between vaccinated and unvaccinated respondents. To answer study research questions, we report descriptive statistics (e.g., frequencies or M and SD) for susceptibility, severity, barriers, benefits, self-efficacy, and cues-to-action. Perceived benefits were reported only for vaccinated respondents. Perceived barriers and self-efficacy were reported only for unvaccinated respondents. Inferential tests between vaccinated and unvaccinated respondents were conducted to examine differences in perceived susceptibility and severity (independent samples t-tests) and for cues-to-action (chi-square analysis).
Results
Results revealed that vaccinated respondents had greater perceived susceptibility (M = 3.56, SD = 1.01) than unvaccinated (M = 3.12, SD = 1.00), t(1, 411) = 3.99, p < 0.001, d = 0.44. Likewise, vaccinated respondents had greater perceived severity (M = 4.39, SD = 0.80) than unvaccinated respondents (M = 3.72, SD = 1.28), t(1, 412) = 6.38, p < 0.001, d = 0.70.
Among vaccinated respondents, common perceived benefits were protecting oneself from COVID-19 (79.9%), protecting loved ones from COVID-19 (78.5%), and concerns about getting sick (34.9%) or dying (32.2%). Among unvaccinated respondents, common perceived barriers included fear of vaccine side effects (58.6%), vaccine distrust (41.4%), and government distrust (34.5%). See Table 2 for a complete list of perceived benefits and barriers.
Among unvaccinated respondents, significant differences arose between those who said they planned to get vaccinated (n = 37), those who did not (n = 39), and those who were unsure (n = 40), F(2, 116) = 14.37, p < 0.001, η2 = 0.20. Post hoc tests revealed that those who planned to get vaccinated had significantly higher self-efficacy (M = 4.14, SD = 0.79) than those did not (M = 2.99, SD = 1.17, p < 0.001) and those who were unsure (M = 3.49, SD = 1.04, p = 0.008).
For cues-to-action, all respondents identified credible sources and channels for COVID-19 information. Credible sources included government medical professionals (52.4%), local medical professionals (44.4%), and elected federal officials (30%). Popular channels for information were the Internet (59.9%), news (54.3%), and social media (45.9%). See Table 3 for a complete list of cues-to-action.
Vaccinated respondents were more likely than unvaccinated respondents to view government medical professionals, χ2(1, 414) = 16.98, p < 0.001, and elected federal officials, χ2(1, 414) = 16.00, p < 0.001, as credible. Among unvaccinated respondents were also more likely than unvaccinated respondents to identify personal contacts, χ2(1, 414) = 4.47, p = 0.035, and messaging apps (like WhatsApp), χ2(1, 414) = 5.22, p < 0.001 as credible channels for COVID-19 information (see Table 3).
Discussion
The current study examined COVID-19 beliefs among Hispanic and Latinx adults using the HBM. Consistent with the HBM, results revealed vaccinated respondents reported greater perceived severity and susceptibility to COVID-19 than unvaccinated respondents. Notably, perceptions of susceptibility were relatively moderate (mean of 3.43 on a 5-point scale), suggesting continued effort is needed in raising awareness among Hispanic and Latinx adults about the risks of COVID-19 transmission. In contrast, perceptions of severity were more robust (mean of 4.21), suggesting many Hispanic and Latinx adults see the consequences of contracting COVID-19 as severe.
Among vaccinated, nearly 4 out of 5 respondents viewed self-protection (“To protect myself from COVID-19;” 79.9%) and protection for loved ones (“To protect my loved ones from COVID-19;” 78.5%) as a benefit of vaccination. These findings align with research conducted by the African American Research Collaborative (2021), which found that the most effective message promoting vaccination—among all racial/ethnic groups—was “Getting a COVID-19 vaccine can protect the lives of my family, friends, and those I love.” The argument that getting vaccinated helps protect yourself and others may resonate with Hispanic and Latinx individuals due to the concept of familismo, a cultural value for family and kinship closeness and protection that has been shown to impact health beliefs and behaviors (Garcia et al., 2021). Our findings suggest the utility of this “protection” messaging in COVID-19 vaccination efforts among Hispanic and Latinx adults.
Among unvaccinated, two-thirds reported they did not plan to get vaccinated or were unsure. The major barriers to vaccination among unvaccinated responses were fear of vaccine side effects (58.6%), distrust in the vaccine (41.4%), distrust in the government (34.5%), and distrust of vaccines in general (22.4%). Furthermore, approximately 1 in 5 unvaccinated respondents (19.0%) cited “not feeling well-enough informed” as a barrier to vaccination. These findings align with previous research (Garcia et al., 2021), which found vaccine hesitancy for Latinos to be rooted in concerns about side effects, mistrust, and fear of being treated like “guinea pigs.” Together, these findings affirm the importance of informing Hispanic and Latinx adults about the safety and efficacy of the COVID-19 vaccines while addressing vaccine misinformation and disinformation.
Overall, perceptions of self-efficacy among unvaccinated respondents were relatively moderate (mean of 3.53). In line with the HBM, self-efficacy was greater among those who planned to get vaccinated compared to those who did not or were unsure. Research using the HBM (Williamson et al., 2017) has found that individuals face self-efficacy challenges not only in performing a task (i.e., getting vaccinated) but also in the decision-making leading up to the task (i.e., deciding whether one should get vaccinated). Future work could examine the role of task-related and decision-related self-efficacy among Hispanic and Latinx adults.
Consistent with previous research (Garcia et al., 2021), respondents reported consuming COVID-19 information through multiple media channels, including the Internet, news, and social media. Surprisingly, national sources were viewed as more credible than local sources (e.g., community leaders, elected officials, television personalities; see Table 3). While channel use was similar among vaccinated and non-vaccinated respondents, unvaccinated respondents viewed very few of the listed sources to be credible for information on COVID-19. These findings highlight the challenge of reaching unvaccinated Hispanic and Latinx adults with credible messengers. Future research should more closely examine perceptions of credible sources and messengers among unvaccinated Hispanic and Latinx adults.
Limitations and Future Directions
This study was limited in several ways. First, given the changing nature of the pandemic, our cross-sectional survey represents a limited snapshot of Hispanic and Latinx adults' beliefs about COVID-19. Second, our survey included a large number of items for perceived barriers (eighteen items), perceived benefits (eight items), and cues-to-action (seventeen items). Therefore, we opted to use a list-style “check all that apply” rather than a Likert-style measure in order to reduce participant fatigue. Our rationale for doing so was to include more items at the cost of precision (which a Likert-style measure would have provided). Third, our sample was diverse in age, gender, and language, but our reach was limited to respondents with access to the Internet residing within the Commonwealth of Virginia. Responses were undoubtedly impacted by the state of the pandemic during the period of data collection. Despite these limitations, we believe these data are timely and relevant for practitioners working to promote COVID-19 awareness and vaccination among Hispanic and Latinx adults.
Conclusion
Our results highlight several opportunities and challenges for efforts to promote COVID-19 awareness and vaccination among Hispanic and Latinx adults. Given the changing nature of the pandemic, continued research on this diverse population is essential.
Data Availability Statement
The datasets presented in this article are not readily available because the study is active. Requests to access the datasets should be directed to marti8ax@jmu.edu.
Ethics Statement
Our research protocol was approved by the James Madison University IRB, Protocol # 21-2622. The patients/participants provided their written informed consent to participate in this study.
Author Contributions
All authors listed have made a substantial, direct, and intellectual contribution to the work and approved it for publication.
Funding
This research was funded by 4-VA, a collaborative partnership for advancing the Commonwealth of Virginia.
Conflict of Interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher's Note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
African American Research Collaborative, (2021). American COVID-19 Vaccine Poll. Available online at: https://covidvaccinepoll.com/app/aarc/covid-19-vaccine-messaging/
Bandura, A. (1977). Self-efficacy: Toward a unifying theory of behavioral change. Psychol. Rev. 84, 191–215. doi: 10.1037/0033-295X.84.2.191
Centers for Disease Control Prevention (2016). Reasons to Vaccinate. Available online at: https://www.cdc.gov/vaccines/adults/reasons-to-vaccinate.html
Centers for Disease Control Prevention (2021). Hospitalization and Death by Race/Ethnicity. Available online at: https://www.cdc.gov/coronavirus/2019-ncov/covid-data/investigations-discovery/hospitalization-death-by-race-ethnicity.html#footnote01
Fisk, R. J. (2021). Barriers to vaccination for coronavirus disease 2019 (COVID-19) control: experience from the United States. Global Health J. 5, 51–55. doi: 10.1016/j.glohj.2021.02.005
Garcia, J., Vargas, N., de la Torre, C., Magana Alvarez, M., and Clark, J. L. (2021). Engaging Latino families about COVID-19 vaccines: A qualitative study conducted in Oregon, USA. Health Educ. Behav. 48, 747–757. doi: 10.1177/10901981211045937
Macias Gil, R., Marcelin, J. R., Zuniga-Blanco, B., Marquez, C., Mathew, T., and Piggott, D. A. (2020). COVID-19 pandemic: Disparate health impact on the Hispanic/Latinx population in the United States. J. Infect. Dis. 222, 1592–1595. doi: 10.1093/infdis/jiaa474
Mercadante, A. R., and Law, A. V. (2021). Will they, or won't they? Examining patients' vaccine intention for flu and COVID-19 using the health belief model. Res. Soc. Administ. Pharmacy 17, 1596–1605. doi: 10.1016/j.sapharm.2020.12.012
Obinna, D. N. (2021). Confronting disparities: Race, ethnicity, and immigrant status as intersectional determinants in the COVID-19 era. Health Educ. Behav. 48, 397–403. doi: 10.1177/10901981211011581
Paek, H.-J. (2016). “Health belief model,” in Health Communication Research Measures, eds J. W. Dearing and D. K. Kim (Peter Lang).
Rosenstock, I. M. (1974). The health belief model and preventive health behavior. Health Educ. Monogr. 2, 354–386. doi: 10.1177/109019817400200405
Sheeran, P., Maki, A., Montanaro, E., Avishai-Yitshak, A., Bryan, A., Klein, W. M. P., et al. (2016). The impact of changing attitudes, norms, and self-efficacy on health-related intentions and behavior: A meta-analysis. Health Psychol. 35, 1178–1188. doi: 10.1037/hea0000387
Skinner, C. S., Tiro, J., and Champion, V. L. (2015). “The health belief model,” in Health Behavior: Theory, Research, and Practice, eds K. Glanz, B. K. Rimer, and K. Viswanath (Jossey-Bass).
Williamson, L. D., Reynolds-Tylus, T., Quick, B. L., and Shuck, M. (2017). African-Americans' perceptions of organ donation: “Simply boils down to mistrust!” J. Appl. Commun. Res. 45, 199–217. doi: 10.1080/00909882.2017.1288293
Witte, K. (1994). Fear control and danger control: A test of the extended parallel process model (EPPM). Commun. Monogr. 61, 113–134. doi: 10.1080/03637759409376328
Keywords: COVID-19, Hispanic (demographic), Latinx, vaccination, Health Belief Model (HBM)
Citation: Martinez Gonzalez A, Reynolds-Tylus T, Galarreta-Aima D and Alemán CG (2022) COVID-19 Beliefs Among Hispanic and Latinx Virginians: An Application of the Health Belief Model. Front. Commun. 7:876656. doi: 10.3389/fcomm.2022.876656
Received: 15 February 2022; Accepted: 28 March 2022;
Published: 29 April 2022.
Edited by:
Seow Ting Lee, University of Colorado Boulder, United StatesReviewed by:
Tony Kuo, University of California, Los Angeles, United StatesHeather Carmack, University of Alabama, United States
Copyright © 2022 Martinez Gonzalez, Reynolds-Tylus, Galarreta-Aima and Alemán. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Andrea Martinez Gonzalez, marti8ax@jmu.edu