
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Commun. , 02 June 2020
Sec. Health Communication
Volume 5 - 2020 | https://doi.org/10.3389/fcomm.2020.00029
 Suruchi Sood1*
Suruchi Sood1* Kelli Kostizak1
Kelli Kostizak1 Charlotte Lapsansky3
Charlotte Lapsansky3 Carmen Cronin2
Carmen Cronin2 Sarah Stevens1Mar Jubero3Theresa Kilbane3
Sarah Stevens1Mar Jubero3Theresa Kilbane3 Rafael Obregon3
Rafael Obregon3Female genital mutilation (FGM) is a complex harmful traditional practice associated with prevalent social norms. Yet, there is a lack of social norms focused conceptual and measurement frameworks to assess the impact of social and behavior change communication-based interventions toward ending the practice of FGM. This manuscript describes the development of an evidence-based macro framework to measure FGM behavior and social norms change over time. ACT is an acronym for the different sections of the framework: (1) Assess What People Know, Feel, and Do; (2) Ascertain Normative Factors; (3) Consider the Context, Especially Gender and Power; (4) Collect Information on Social Networks and Support; (5) Track Individual and Social Change Over Time; and (6) Triangulate All Data Analysis. ACT takes a social-ecological perspective to change and was constructed using various social norms theories, both in general and specific to FGM. Subsequently, meetings were held with social norms and FGM field experts across the world to further refine the framework. The ACT framework includes a menu of constructs, indicators, methods, and tools that can be adapted according to available resources, the local context, and research limitations. Both qualitative and participatory quantitative methods are described. Descriptions of the steps necessary to measure social norms change with regard to FGM through monitoring and evaluation are included. The ACT framework allows for change to be directly linked to the communication approaches used by interventions through attribution and contribution using indicators to measure outputs, short-term outcomes, and exposure. Triangulation is built into the ACT framework to facilitate validation, enrichment, and holistic interpretation of data, as well as creating a feedback loop. ACT is currently being validated in two countries in Africa in which FGM is practiced to different extents. Next steps are discussed.
Female genital mutilation (FGM), also known as female circumcision, is a harmful traditional practice involving the partial or complete removal of the external female genitalia. There are four types of FGM: (1) clitoridectomy: where the clitoris is partially or totally removed (sometimes this is referred to as sunna); (2) excision: where the clitoris and labia are partially or totally removed; (3) infibulation: where the vaginal opening is narrowed by sewing the labia together; and (4) other: all other forms types of FGM procedures including “pricking, piercing, incising, scraping, and cauterizing the genital area” (World Health Organization, 2012). FGM is prevalent throughout much of Africa, parts of the Middle East, and Asia, and is an emerging public health issue in the United States, United Kingdom, and other countries where immigrant communities continue the practice (World Health Organization, 2012). The prevalence of FGM among practicing countries varies between 1 and 98% of the female population (UNICEF, 2013). Worldwide, more than 125 million girls and women have undergone FGM (UNICEF, 2013). FGM is considered a harmful traditional practice because it has no health benefits and is associated with a variety of negative health implications, including bleeding, infection, cyst formation, painful sexual intercourse, and issues during childbirth (World Health Organization, 2012; UNICEF, 2013).
To accelerate the abandonment of FGM, UNFPA and UNICEF have implemented a Joint Program providing financial and technical support to 17 countries and using human rights-based and culturally sensitive approaches to eliminate the social norms that perpetuate FGM [United Nations Population Fund and United Nations Children's Fund, 2015]. A critical component of the Joint Program is the development of a macro-level monitoring and evaluation (M&E) framework to examine how communication approaches can change social norms around FGM. The framework is grounded within social norms theory broadly, as well as existing literature on addressing social norms specifically related to FGM.
The term used to describe the set of practices comprising FGM is debated. Female circumcision was commonly used when FGM first gained international attention (UNFPA, 2019). However, this term was abandoned beginning in 1970 to emphasize the difference between the health risks of male circumcision and FGM (UNFPA, 2019). Since 1994, the United Nations (UN) uses “FGM” in conference documentation and publications where the term is viewed as an advocacy tool (UNFPA, 2019). UN Member States made it clear that “FGM” should be the term used to describe this set of practices in UN Resolution 65/170 (UNFPA, 2019). Around this time, the term “female genital cutting (FGC)” started to be used by some groups because they felt “FGM” has negative and demeaning connotations which could interrupt and undo programmatic efforts to end the practice (Gillespie, 2013; UNFPA, 2019). In the first phases of the UNICEF-UNFPA Joint Program (2008–2017), “female genital mutilation/cutting (FGM/C)” was used to encompass both terms. The decision was made at the start of phase 3 to use “FGM” instead of “FGM/C.” This choice was guided by the desire to emphasize the harmful nature of the practice and the human rights violation it represents for women and girls as well as to align with the UN's use of FGM (UNFPA, 2019).
Social norms can be thought of as the unwritten rules guiding behavior; in essence, they encompass what we do, what we think others do, and what we think others believe that we should do (World Health Organization, 2010). Social norms literature and theorizing can be consolidated around two main approaches. The first approach considers social norms an intrinsic characteristic of individuals embedded within a broader social system (Cialdini and Melanie, 1998; Bicchieri, 2006, 2017; Mackie et al., 2015). The second approach takes a social ecological perspective, with norms as one element of a larger framework (Rogers, 1995; Kincaid, 2000; Kincaid and Figueroa, 2004; Kincaid et al., 2006, 2007; Storey and Figueroa, 2012).
When considering the first approach, norms are defined as rules or expectations held by social groups that guide behaviors (Mackie et al., 2015). From this perspective, two conditions must be satisfied for a norm to exist. First, individuals must have awareness of the norm and believe that it pertains to them. Second, individuals conform to the norm if: (1) they expect that a majority of their social network will conform to the norm (empirical expectations) and (2) they believe that a sufficiently large part of their social network thinks they ought to conform and may sanction them if they do not (normative expectations) (Mackie et al., 2015). These expectations are what keep people from “cheating” due to concerns about what others will think or may do for non-compliance (Bicchieri and Muldoon, 2014). In contrast, normative expectations also include the rewards and social acceptance that individuals expect to reap for conforming to norms. Reciprocal expectations (norm of reciprocity) dictate that rewards and benefits received should also be returned, establishing an interdependence that continually impacts the behavior of individuals within the social system (Mackie et al., 2015).
In the context of FGM interventions, this first approach has resulted in work at the community-level to foster discussion with the aim of sparking collective decisions and public pledges to abandon the practice (Gillespie and Melching, 2010; Cislaghi et al., 2016). Discussion is fruitful for combating pluralistic ignorance, the phenomena where people personally do not approve of a norm but adhere to it anyways because they falsely believe others approve (Miller et al., 2000; Yanovitzky and Rimal, 2006). Normative behaviors continue to prosper in an environment of pluralistic ignorance unless attitudes around the norm are revealed, allowing them to be challenged and reconsidered (Miller et al., 2000). Interpersonal communication provides an avenue to uncover what others “really” think; as such, norms are essentially a communication phenomenon (Yanovitzky and Rimal, 2006).
Another key aspect of this school of thought is that norms support each other and are also supported by associated beliefs (Mackie et al., 2015). For example, in the case of FGM, an associated belief might be that FGM is required by religious doctrine (World Health Organization, 2012). Similarly, the practice of FGM is closely intertwined with gender dynamics and indicative of societal discrimination against girls (World Health Organization, 2012). Therefore, action to rethink supporting beliefs individually and collectively is needed for change to be achieved.
The second set of theorizing about social norms has been central in communication field, with several key models/theories including social norms as part of a larger equation of behavior and social change. For example: theory of planned behavior, theory of normative social behavior, ideation, and the theory of bounded normative influence, among others (Ajzen and Fishbein, 1980; Ajzen, 1991; Kincaid, 2004; Kincaid and Figueroa, 2004; Kincaid et al., 2007; Storey and Figueroa, 2012; Rimal and Lapinski, 2015). From this point of view, social norms are an intermediate step that must change to accomplish behavioral outcomes. Here, the use of a social-ecological perspective situates individuals within their broader environment and allows for analysis at different levels of influence as well as the development of strategies to impact various levels (Kincaid et al., 2007). Building upon the human rights-based approach, the social ecological model encourages a focus on intersectional issues such as gender and religion (Kincaid et al., 2007). Such models are critical to consider when examining norms from a practical standpoint of applied research to design, monitor, and evaluate the effectiveness of specific interventions aiming for long-term and sustainable change in normative behaviors like FGM.
Different theoretical positions use different terminology. However, the underlying premise across social norms theorizing is that norms influence behavior and vice versa. If normative beliefs can be changed, behavioral change will ensue, and if behavior change occurs then norms will likewise change. Table 1 summarizes these overlapping social norms constructs and provides key citations from where these constructs were selected.
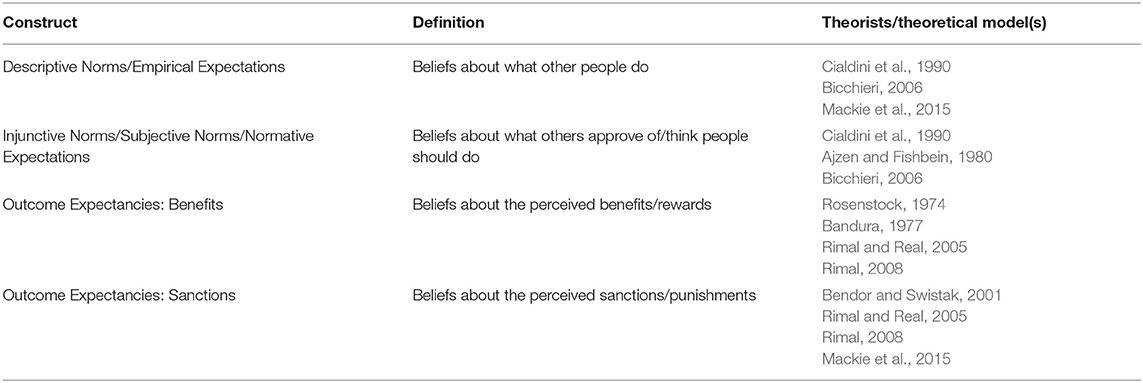
Table 1. Summary of social norms constructs.
Across both approaches, a social norm entails both positive and negative outcomes for members of groups (Mackie et al., 2015). Compliance with a norm may yield simultaneous positive and negative payoffs for an individual which may be aligned with, or contrary to, the positive and negative outcomes for communities (Mackie et al., 2015). The role of rewards and sanctions as they relate to individual and community outcomes are summarized in Table 2.

Table 2. Role of rewards and sanctions on FGM.
Recent and growing interest in social norms interventions has resulted in social norms-specific conceptual models. The Flower for Sustained Health is one such conceptual model created by the Learning Collaborative (Cislaghi and Heise, 2017; Institute for Reproductive Health, 2019). The Flower Model illustrates the how resources, and individual, social, and institutional factors shape the social and gender norms at play, all of which determine the level of power individuals hold. The Everybody Wants to Belong model takes a broad approach, illustrating how environmental factors, context, personal characteristics, and sociological factors affect psychological factors like attitudes, cognitive bias, and self-efficacy, and in turn the adoption of a new behavior (Petit and Zalk, 2019). Here, multiple social norms components are grouped into the sociological factors construct which is affected by the context and environmental factors at play, all of which affect the psychology of the individual and ultimately their choice whether to adopt a behavior (Petit and Zalk, 2019).
The FGM literature is diverse in its theorizing on social norms. Three predominant approaches come to the fore when examining this literature. First, social convention theory emerges as the leading approach to understanding FGM within a social norms perspective (Mackie, 1996, 2000). Mackie argues that when a sufficient number of people perform FGM, the practice becomes locked in place; those who do not practice FGM then fail to marry and reproduce (Mackie, 1996, 2000). Creating a sustainable shift in FGM prevalence requires a critical mass of people to not only abandon the practice, but to also allow their children to marry uncut women (Mackie, 1996, 2000). Research conducted by Shell-Duncan et al. (2011) expands upon Mackie's work and suggests that FGM in Senegal and The Gambia operates as an intergenerational peer convention more so than a marriage convention. In this line of thinking, FGM is a convention facilitating entry into a social network, in turn granting individuals access to social support, social capital, and power (Shell-Duncan et al., 2011). Efforts to promote abandonment of FGM then need to work across generations and actively involve as many members of women's social networks as feasible. Regardless of the type of convention at play (marriage, intergenerational, or peer), discerning the nature of these conventions is key to social norms change.
A second strand of theorizing focuses on identifying the economic and social benefits families attribute to cutting (Bellemare et al., 2015; Efferson et al., 2015). These theorists argue that factors other than conventions are at play when it comes to norms associated with FGM (Bellemare et al., 2015; Efferson et al., 2015). They state that for the convention argument to hold true in the context of FGM, cutting rates would be coordinated within relatively homogeneous communities, i.e., either be very high or very low (with attitudes matching the norm) (Bellemare et al., 2015; Efferson et al., 2015). If cutting practices and attitudes vary, then cutting and non-cutting communities should be clearly different from one another (Bellemare et al., 2015; Efferson et al., 2015). Recent research conducted by these authors in Sudan revealed that estimated cutting rates vary substantially within and across communities (Bellemare et al., 2015; Efferson et al., 2015). Additional data from a representative survey of adults in Sudan indicated that families would not refuse marriage with other families in the communities for FGM reasons (Bellemare et al., 2015; Efferson et al., 2015). Together these findings suggest that there is unlikely to be a single critical threshold at which the conventional practice of FGM is either abandoned or replaced by an alternative practice. As such, perhaps the mixed results regarding public declarations to reduce FGM (which aim to address FGM as a convention) signal a need to focus efforts elsewhere, such as identifying the benefits families attribute to cutting. Meaning, social norms change requires homing in on and altering the exchange of incentives, transaction costs, and social welfare benefits associated with the practice.
The third type of theorizing construes FGM as a complex issue that persists in the face of contradictory and complementary legal, moral, religious, gender, and social norms. For example, government institutions enforce legal norms. As of 2012, 24 countries in Africa have legislation in place banning FGM with penalties ranging from a minimum of 6 months to a maximum of life in prison, with some penalties imposing monetary fines (UNFPA, 2016). Limited knowledge and poor enforcement make it difficult for legal norms to be used as an effective tool (Shell-Duncan et al., 2013; Kandala and Komba, 2015). Shell-Duncan, Wander, Hernlund and Moreau found that knowledge of the ban in Senegal was high but superficial as few people knew of instances where the ban was actually enforced (Shell-Duncan et al., 2013). Legislative action criminalizing FGM alone does not appear to be a sufficient deterrent to the practice. However, for communities that abandon the practice, such legislative action can render support for new social norms in lieu of FGM and provide ammunition and guidance as communities change their attitudes and behaviors (Shell-Duncan et al., 2013). It is in these instances that legal norms and social norms are in harmony.
On the other hand, moral norms (inner convictions of right and wrong) are motivated by conscience rather than by social expectations (Mackie et al., 2015). Those who have more strongly internalized messaging on the potential health risks linked to FGM are more likely to support ending the practice (Shell-Duncan et al., 2010). As research by Cislaghi et al. (2016) shows, value deliberations have the potential to establish new understandings of peace, security, and equality within a community that could in turn help to flip the “moral norm” from one that used to accept FGM to one that rejects the practice.
Due to the fact that FGM continues to persist in the presence of legal sanctions (though weakly imposed) and un-supportive moral norms, FGM can be construed as something the population feels is a social obligation (i.e., it continues to exist due to social norms supportive of FGM) (LeJeune and Mackie, 2008). This being said, it is essential to keep a broader perspective of social stratification in mind by focusing on issues of gender and power that in many ways result in the codification of social norms around FGM (CARE, 2017). Gender norms refer to informal rules and shared social expectations that distinguish expected behavior on the basis of gender (Marcus and Harper, 2015). Discriminatory gender norms cut across all domains of the social ecological model (Marcus and Harper, 2015). For example, they manifest themselves as negative gender role attitudes toward girls and women at the individual level, restrictions on mobility and educational opportunities at the family and community levels, and at the social level include restrictions like age of marriage, emphasis on virginity, and sexual control (Berg and Denison, 2012). Pervasive negative gender norms across all the levels, likely underpin FGM practices (CARE, 2017). Therefore, attempts to address FGM have to account for the individual, social and structural silencing of women's voices (CARE, 2017). As such, any measurement of social norm change associated with FGM must specifically consider gender normative determinants (CARE, 2017).
Religious norms “are distinctive because of their reference to divine command, but otherwise they function as social, legal, or moral norms” (Mackie et al., 2015). Some supporters of FGM abide by the practice on religious grounds; populations in several countries believe FGM is supported by (as a sunna) or even required (as a farata) in Islam (Shell-Duncan et al., 2010). Although it is not a religious requirement in the Qur'an, some Sunni Muslims legitimatize FGM by quoting controversial hadiths (a saying attributed to the Prophet Mohammed) (Shell-Duncan et al., 2010). Thus, in many countries, the Qur'an is interpreted as implying that FGM facilitates the cleanliness and purification necessary for religious prayer and participation of women (Shell-Duncan et al., 2010; El-Damanhoury, 2013). In a few cases, FGM is also considered to be supported by Jewish and Christian beliefs (El-Damanhoury, 2013).
In summary, FGM can largely be construed to exist due to a myriad of factors, including conventions associated with future marital prospects, traditions that have withstood time, traditions that reinforce power structures and afford social capital, and peer pressure. FGM persists largely because it provides economic and social benefits and due to the lack of harmonization between legal, moral, gender, and religious imperatives around the practice.
Regardless of framing, communication approaches targeting social norms related to FGM can use two approaches. One is the norm-abandonment approach, in which monitoring and evaluation consists of maintaining its absence and preventing re-emergence. The other is the norm replacement approach, in which an innovative alternative associated with a separate set of practices is introduced (Kincaid, 2004; Population Council, 2016-2017). In this case, monitoring and evaluation consists of measuring the uptake of the innovation (Kincaid, 2004; Population Council, 2016-2017).
Concrete data on how to operationalize social norms, as well as the effectiveness of social norms approaches within communication-based initiatives, is limited. A World Health Organization (2010) report concluded that social norms approaches in public health have rarely been evaluated, providing a weak evidence base of their effectiveness. A meta-analysis of programs targeting FGM, including those using a social norms approach, also came to a similar conclusion (Berg and Denison, 2012). More recently, Mackie et al. (2015) found that only 14% of published manuscripts discussing social norms and global development mentioned measurement methods of any kind.
To fill this gap, a macro-level M&E framework was developed based on a literature review conducted using two databases: PubMed and Google Scholar. Two separate searches were undertaken. The first was to identify research articles on social and behavior change interventions designed specifically to address FGM and the second sought publications examining the theoretical underpinnings of social norms approaches. Relevant articles were used to compose a list of social norms, communications, and FGM experts who were then contacted to gather additional work they had done as well as resources they found useful in their work. Therefore, the review was not systematic but was rather based on expert feedback to form an evidence base of resources critical to developing a macro-level M&E framework for FGM social norms change.
Results from the literature review were presented at a 2-day consultative workshop with experts from several institutions including: George Washington University, Johns Hopkins University, University of Pennsylvania, Columbia University, Georgetown University, London School of Hygiene and Tropical Medicine, the Population Council, ITAD, the Overseas Development Institute, and the Bill and Melinda Gates Foundation. In addition to presenting the review findings, the workshop served to conceptualize the practice of FGM and examine existing measurement tools and programming for FGM specifically and social norms broadly.
Following the review and expert's workshop, a conceptual model and draft M&E framework (including measurement tools) were developed. Tools were gathered from the literature and the expert's recommendations when possible. Tools were then created to fill gaps as needed to examine all constructs of the conceptual model and individual indicators adequately. The draft framework was then presented at the Joint Program's Annual Meeting on FGM in Kampala, Uganda [United Nations Population Fund and United Nations Children's Fund, 2015] followed by several webinars in June and September of 2017 with Joint Program staff based in Africa and the Middle East. Through these activities, the ACT framework was further refined and developed using an interactive and iterative process.
A conceptual model (Figure 1) outlining how the key constructs/concepts of the ACT framework work together was developed. Social norms are at the heart of the conceptual model, surrounded by their components: descriptive norms (beliefs about what others do), injunctive norms (beliefs about what others think), and outcome expectancies (rewards and sanctions) (Mackie et al., 2015). This placement signifies that social norms are an intermediary step between what people know and feel as well as their social networks and levels of social support (on the right) and individual and social change (on the left).
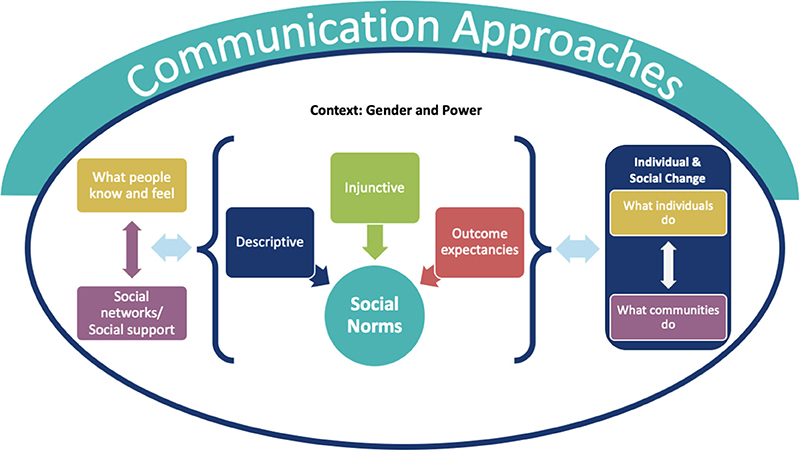
Figure 1. Conceptual model for ACT framework.
The dynamic relationship between knowledge and affective factors and social networks and social support is signified using two-way arrows. The same is shown for the relationship between individual and community-level behaviors, which interact with one another to determine individual and social change. In this way, the model incorporates a social-ecological perspective that situates individuals within their broader environment (e.g., interpersonal, community, institutional, societal, etc.) by taking into account the different levels of influence at play. For instance, the model acknowledges how what people know and feel shapes, and is shaped, by who they talk to (i.e., interpersonal communication and social networks) and the social support received. Similarly, what individuals do is influenced by what happens within a community, and vice versa.
The model is placed within an oval labeled “Context: Gender and Power” because the relationships in the conceptual model are mitigated by these contextual factors. Social norms cannot change if contextual factors such as power and gender are not adequately addressed (Mackie et al., 2015). Likewise, what people know and feel, social networks and support, and the level of individual and social change achieved are all affected by, but also can affect, the contextual factors of gender and power.
Communication approaches are depicted just outside the context oval, depicting the direct influence that communication approaches have on individual and social change, as well as the indirect ways that communication approaches affect change by impacting knowledge, affective factors, social networks, social support, social norms, and contextual factors. Linking the communication approaches to individual and social change allows for claims about attribution and contribution to be made and provides key insights into how change occurs.
ACT is an acronym for the different constructs of the framework and steps necessary to measure social norms change relative to FGM. The constructs within the ACT framework were created to assess the elements of the conceptual model. Both the “A” and “C” cover the specific constructs that must be measured to examine social norms change. The “A” focuses on (1) knowledge, affective, and behavioral factors; and (2) the normative factors, including descriptive and injunctive norms and outcome expectancies. The “C” encompasses (1) the context, especially gender and power; and (2) collecting data on social networks and social support. For each construct of the “A” and “C” of the ACT framework, indicators and means of verification (quantitative structured interview tool, qualitative and participatory focus group discussion and in-depth interview guides) are provided. Each indicator is associated with a specific set of questions and qualitative activities. Researchers can select the indicators they want to use depending on their programmatic goals, resource constraints and evaluation needs, thus a “menu” approach can be used.
The “T” of the ACT framework refers specifically to the larger M&E process the ACT framework is couched within. This section includes: (1) information on how to track change over time including sample indicators and quantitative items in the structured interview tool; and (2) how to triangulate the data using a mixed-methods approach to improve validity, enrich data, allow for holistic interpretation, and foster and capitalize upon the feedback loop between the monitoring and evaluation stages.
Tables 3–5 illustrate the linkages between the ACT framework constructs, and aggregated and disaggregated indicators. The details of all indicators and measurement tools are outside of the scope of this paper, but a summary of indicators and a sample of qualitative and quantitative means of verification is provided below.
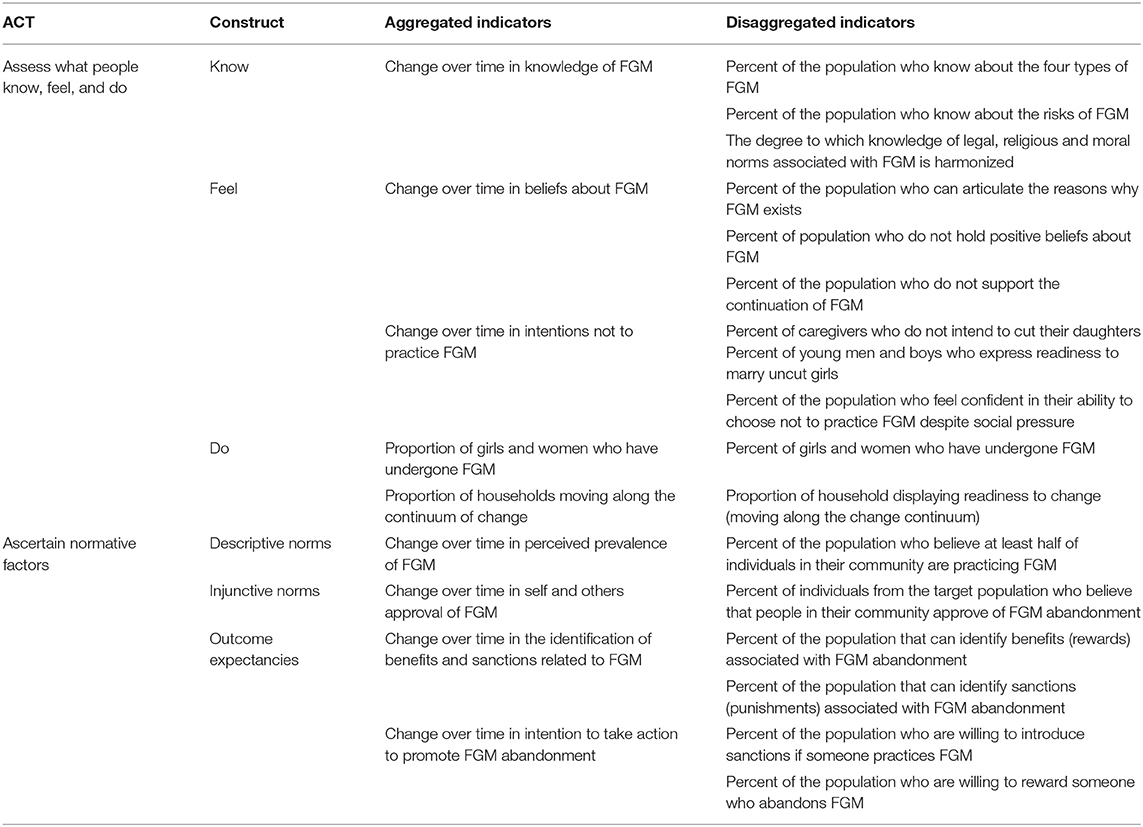
Table 3. “A” ACT indicators.
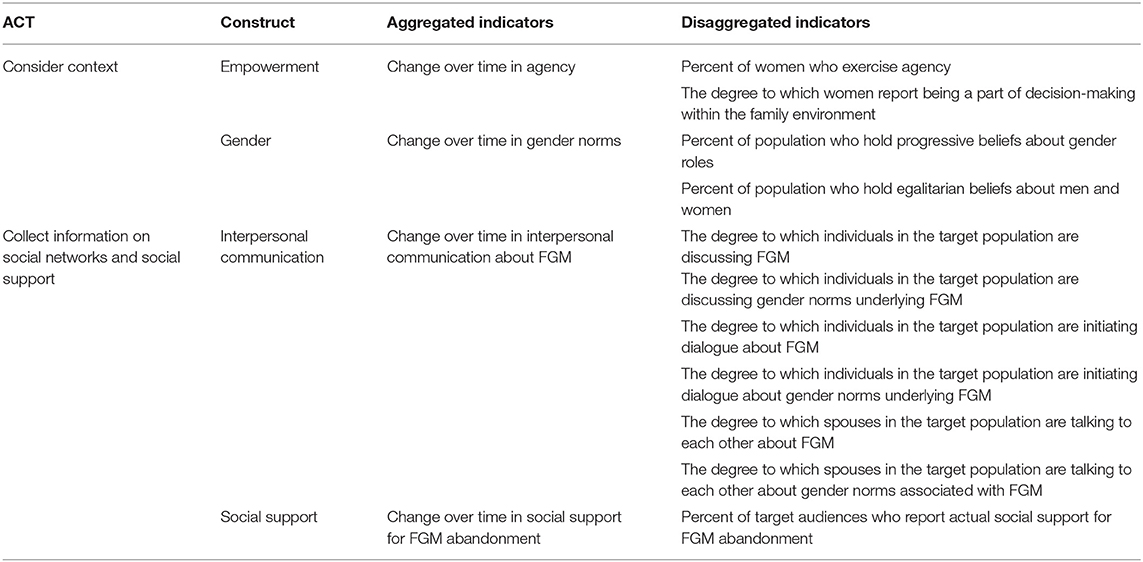
Table 4. “C” ACT indicators.
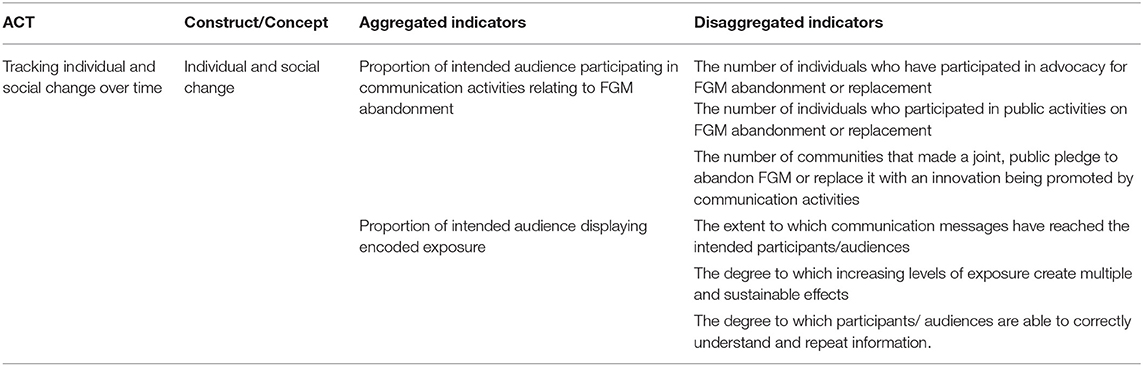
Table 5. “T” ACT indicator.
Measuring what people know, feel, and do provides data on where individuals fall along the continuum of change. Cultivating awareness while dispelling myths is critical to bringing an end to FGM.
In the Assess What People Know section, the indicators focus on measuring the level of correct, factual knowledge concerning FGM among the population (see Table 3). The key topic areas are: (1) the types of FGM; (2) the risks of FGM; and (3) the degree to which knowledge of legal, moral, and religious norms is harmonized.
In the structured interview tool, respondents are asked to list the types of FGM that they believe exist, both in general and specific to their community, in order to quantitatively assess knowledge of the types of FGM. Diagrams that depict the external female genitalia and images depicting the four types of FGM are included. These visual aids can help prompt participants. The image of the external female genitalia can be used to see how many types of FGM participants think there are and what they entail. The diagrams of the different types of FGM can be used to directly ask participants if they can identify the type of cutting shown in each image.
Knowledge of the risks of FGM encompasses both the physical and psychosocial risks associated with the practice. The structured interview tool includes items that directly ask the participant to name the physical, psychological, and social risks associated with FGM in an open-ended format. Participants are then probed about which of the risks they named they believe are the most severe. This allows for an understanding of not only what is considered a risk by the population, but how they weigh these risks. Further, participants are then asked about the likelihood that various risks will occur to measure perceived risk. The focus group discussion guide includes a participatory, qualitative method to measure knowledge of risks associated with FGM using body maps containing an image a girl. Body maps are a visual technique that incorporates diagrams representing part or all of the body to examine knowledge about anatomy as well as perceived health risks (Gastaldo et al., 2012). Using the body map, participants are asked to describe or write/draw what the different parts of the body, the heart, and the mind experience when undergoing FGM, allowing researchers to examine both physical and psychosocial effects of FGM. Participants can complete the body maps at different time points: before, during, and after undergoing FGM. They can then describe the differences and similarities between time points, in turn eliciting a more nuanced description of the impacts of FGM.
Comparison of the level of knowledge concerning legal, religious, and moral norms associated with FGM can help researchers identify misinformation among the different domains where programs can focus more effort. This section focuses on whether participants are aware of these types of norms in the community, not perceived and personal approval (injunctive norms) and practice (descriptive norms), which are measured in the Ascertain Normative Factors section. Legal norms are assessed quantitatively through asking whether participants know any laws pertaining to FGM at the local, national, and international levels. Participants are then probed about the degree to which the laws have been implemented and enforced by asking whether or not they have witnessed families face legal repercussions for practicing FGM. Moral and religious norms are assessed using a series of questions asking whether participants agree with statements about FGM as a religious requirement and FGM as “the right thing to do.” Responses are in a scale format from strongly disagree to strongly agree. These moral and religious statements were identified based on common moral and religious norms around FGM from the literature review and feedback from the expert's workshop. The percentage of the population who know the laws about FGM, believe FGM is a religious requirement, and believe FGM is “the right thing to do” is then compared to assess harmonization of knowledge between norms.
How individuals and communities feel is a critical middle step between having knowledge and actually practicing FGM or taking part in social change by abandoning the practice. The indicator topics of the Assess What People Feel construct are: (1) reasons why participants feel FGM exists; (2) negative beliefs toward FGM; (3) support of FGM abandonment; (4) intention not to cut daughters; (5) intention to marry uncut women; and (6) self-efficacy to abandon FGM in the face of social pressure (see Table 3). Three of the six indicators are discussed in more detail here.
Examining why participants believe FGM exists allows researchers to understand the motivations behind FGM, but also allows participants to reflect on the issue which is a key process in paving the way for behavior and social change. The structured interview questions used for the harmonization of knowledge of legal, moral, and religious norms above serve as a proxy for reasons why FGM exists. The focus group discussion guide includes the free listing participatory activity to measure this indicator qualitatively. Free listing prompts participants to reflect on a domain by stating the first thing that comes to their mind when given a certain term or set of terms (Weller and Romney, 1988; Brewer, 2002; Ulin et al., 2005). In the focus group discussion guide, participants are asked to free list reasons why FGM exists. These responses are then categorized by the group as legal, moral, religious, gender, and social reasons, and/or personal beliefs to illustrate how participants conceptualize reasons behind FGM. Participants are then asked which they think are the most important/influential reasons and why to show which reasons are perceived as critical to upholding the practice.
A series of semantic differential scales with dichotomous terms are included in the structured interview guide to qualitatively assess the proportion of the population who hold negative beliefs toward FGM. The terms were selected based on the literature review and expert feedback as ideas and attitudes commonly associated with FGM. For example, “impure” and “pure” are included in the structured interview because FGM is commonly associated with purity in order to pray among Muslims in some communities (Ibrahim et al., 2018). The same set of semantic differential items are used to examine attitudes toward cut and uncut girls, as well as communities who practice and do not practice FGM. This facilitates comparison of data among the uncut and cut categories on both the individual and community levels to allow for a deeper understanding of the degree to which participants hold negative beliefs about FGM. The in-depth interview guide includes the empathy mapping activity to measure negative beliefs toward FGM. Empathy mapping is a visual technique used in business and marketing to understand what customers think, feel, see, say, do, and hear in a given context (Osterwalder and Pigneur, 2010). Here participants draw and describe what they and other people would see, think, feel, say and do in an FGM-free community. They are then probed for what motivating factors and obstacles exist toward establishing such a community.
The structured interview guide includes items that ask participants directly whether they think FGM should continue to measure support for FGM abandonment using a binary format. Participants are then probed for who is responsible for ending FGM in their community as an open-ended question. Qualitative methods allow for an indirect approach to these questions. The complete the story activity, included in the in-depth interview guide, uses a hypothetical vignettes (either pictorial or verbal stories/scenarios) that participants react to or resolve (Bicchieri, 2017). These vignettes allow researchers to: (1) study what specific actions or behaviors a participant would take in a given situation; (2) explore beliefs, attitudes, and opinions; and (3) bring up sensitive issues (like FGM) without having the participant speaking directly from their personal experiences, but rather projecting onto a third party (Bicchieri, 2017). Participants are read a short story about a family deciding whether to cut their daughter. They then respond to questions about what advice they would give, how the family's decision will affect their lives, and how the family's decision effects the community as a whole. The complete the story data measures support for FGM abandonment as well as negative beliefs toward FGM.
The Assess What People Do section examines actual behavior by measuring the prevalence of FGM as well as where households fall on the continuum of change. The latter indicator is measured using a composite index (described in the ACT framework package) created from all know, feel, and do indicators.
Self-reports, such as those used in large population-based surveys like the Demographic and Health Surveys (DHS) and the Multiple Indicator Cluster Survey (MICS) are one way to quantitatively determine FGM prevalence (Banks et al., 2006; Bellemare et al., 2015). The structured interview tool includes several prevalence questions that use a binary “yes/no” format including asking the participant themselves if they have been cut (for women and girls), asking whether their youngest daughter has been cut, whether their oldest daughter has been cut, and whether any girl or woman in their household has been cut. Health records and gynecological examinations can be used to verify these self-reports, but they are costly and invasive (Morison et al., 2001). Cultural markers are a novel and indirect way to verify self-reported FGM prevalence (Efferson et al., 2015). One study in Sudan measured FGM prevalence by photographing henna on girls' feet based on the fact that henna was applied during the FGM ceremony among this particular community (Efferson et al., 2015). Self-reports were used to corroborate findings and researchers determined that using the cultural markers was a valid way to examine FGM prevalence for this population (Efferson et al., 2015). The structured interview tool includes an open-ended question to determine if there are any cultural markers researchers can use to verify the self-reported prevalence with their population.
A complimentary qualitative, participatory method to measure FGM prevalence included in the in-depth interview guide is the lifeline activity. In this activity, participants map out the lifeline of a typical woman in their community from birth to age 45. Participants are then asked specifically whether a “typical” woman undergoes FGM and if so at what age, providing an indirect way to determine FGM prevalence.
The Ascertain Normative Factors section provides indicators to measure injunctive norms, descriptive norms, and outcome expectancies (see Table 3). It is critical to assess all these factors to unpack the role of social norms approaches in promoting social and behavior change. All questions in this section were created following the literature review and based upon the inputs from the expert's workshops.
The injunctive norms indicator measures the proportion of individuals that believe others in their community approve of FGM abandonment. In this section of the structured interview tool, participants are asked whether they think groups on various levels of the social ecological model (family, peers, community, society in general) approve of FGM continuation or abandonment. Participants are also asked whether they personally believe in FGM abandonment or continuation. Discrepancies between personal and perceived approval indicates that social norms may be at play (Mackie et al., 2015). Likewise, if participants personally do not approve, but falsely believe others at multiple levels approve, it suggests the existence of pluralistic ignorance (Miller et al., 2000; Yanovitzky and Rimal, 2006).
Descriptive norms are operationalized as beliefs about what other people do; specifically, beliefs about whether others are continuing or abandoning FGM. Like with injunctive norms, the structured interview tool asks whether participants think groups on various levels of the social ecological model are continuing or abandoning FGM. Likewise, they are asked how many girls and women in their community at different age groups and overall have been cut out of 10 (using their fingers as a visual aid) to measure perceived prevalence. Perceived prevalence of FGM may be operationalized in three ways: the current perceived prevalence, the perceived prevalence 5 years ago, and the perceived prevalence 5 years from now. Participants are also asked whether they are expected to continue or abandon FGM. This enables perceived prevalence to be compared with perceived behavioral expectancy.
The six indicators to operationalize outcome expectancies are listed in Table 3. The structured interview tool asks participants to reflect upon the social benefits and sanctions associated with FGM abandonment. The questions are open ended, so participants can list as many things as they like. Participants are asked whether they agree with these rewards and sanctions in a binary format and whether they would be willing to impose these rewards and sanctions upon others using a 0–10 point scale. For abandonment or replacement norms to take root, they must be promoted and “out-compete” the old norm of practicing FGM (Evans et al., 2019). Individuals who can articulate and identify the benefits of abandoning FGM are more likely to change their perception of the practice and abandon it. So too are those who agree with the rewards associated with FGM abandonment and those who are willing to enact these rewards upon FGM abandoners.
A novel participatory, mixed-methods tool for examining norms and outcome expectancies are the 2 × 2 tables for social norms included in the focus group discussion guide. Participants in work through two 2 × 2 tables that ask about abandonment and continuation of FGM. The first is the “approval” table, which measures injunctive norms. Participants are asked whether they personally approve of continuation or abandonment, and whether they think that others whose opinions matter to them approve of continuation or abandonment. The second is the “behavioral expectation” table, which measures descriptive norms. Participants are asked whether they think that others are continuing or abandoning FGM, and whether others expect them to continue or abandon the practice.
For each table, responses fit into one of four quadrants with each participant representing one tally mark. This allows for quantitative analysis concerning the proportion of individuals who fall into the various quadrants. The proportions per quadrant are then compared between the “approval” and “behavioral expectation” table. In this way, discrepancies between injunctive and descriptive norms can be examined. The probes for the activity include discussion questions about the reasons for the discrepancies between quadrants, why they fell into the quadrant they did on each table, and the social rewards and social sanctions of FGM abandonment and continuation.
The “C” of the ACT framework encompasses the constructs (1) Consider the Context, Especially Gender and Power and (2) Collect Information on Social Networks and Social Support. Social norms change is not possible unless power dynamics are addressed (Mackie et al., 2015). Thus, examining whether FGM persists due to power imbalances (power over) is critical. If FGM is persisting in part due to power imbalances, program planners should determine how individuals or groups can be empowered to abandon the practice. Aside from gender and power dynamics, reference groups (a network of people to whom we identify and compare ourselves) are critical in the creation and maintenance of norms (Lapinski and Rimal, 2005). Likewise, the level of social support received from those in our social networks affects behavior adoption and maintenance (Holt-Lunstad and Uchino, 2015).
The ACT framework draws upon CARE's (2013) theoretical framework for empowerment, which encompasses three overlapping domains that must be addressed for meaningful change to occur (Hillenbrand et al., 2015). The first domain is individual agency, which includes self-efficacy and attitudes and beliefs about gender and women's rights. The second domain is relations, which relates to decision-making power, mobility, and communication among spouses (Hillenbrand et al., 2015). Finally the structure domain consists of level of ownership and contribution toward household assets, social cohesion, and participation in collective action, among others (Hillenbrand et al., 2015). The various components of CARE's (2013) theoretical framework for empowerment are captured within the Consider the Context construct (as well as other cross-cutting indicators of the ACT framework, for example, spousal communication regarding FGM is an indicator of Collect Information on Social Networks and Social Support and also measures CARE's relations).
Two indicators in the ACT framework focus on measuring the level of empowerment women experience: (1) the proportion of women who exercise agency and (2) the degree that women are a part of decision-making in the family environment (see Table 4). The Women's Empowerment Scale is employed in the structured interview tool to assess agency across three areas: mobility, freedom from family domination, and security and contribution to family support (Nanda, 2011). A qualitative method to compliment the Women's Empowerment Scale included in the in-depth interview guide is the “I am…” free listing activity. To complete the activity, participants list all the words that come to mind given the prompt “I am…”. This provides indirect information on agency through assessing participant's self-concept (Weller and Romney, 1988; Brewer, 2002; Ulin et al., 2005).
The indicator for degree of decision making power women possess within the family environment is operationalized through the Participation of Women in Household Decision-Making Index used in the DHS [Measure Evaluation (n.d)]. This index includes a series of items asking who has the “final say” on several family decisions concerning: visiting friends, family planning, healthcare, food to cook each day, small purchases, and large investments. This facilitates measurement of the relations and structure domains of CARE's framework (discussed above). Response categories in the ACT framework range from a joint decision to mainly the decision of the respondent. In this way, questions capture what types of decisions women can make independently, which are mainly made by men, and which are made jointly.
Gender Norms indicators are: (1) the percent of the population who hold progressive gender role beliefs and (2) the percent of the population who hold egalitarian beliefs about men and women (see Table 4). The Gender Norm Attitudes scale and the Attitude Toward Wife Beating Scale from the DHS were adapted for these indicators. The Gender Norm Attitudes scale includes questions concerning gender roles and traditional vs. progressive gender beliefs (Nanda, 2011). The Equity for Girls subscale contains four items that specifically address progressive gender role beliefs and egalitarian beliefs about men and women (Nanda, 2011). The Attitude Toward Wife Beating Scale measures beliefs about spousal abuse (Nanda, 2011). Participants are given a series of situations and probed as to whether it would be appropriate for a husband to beat his wife in this situation (Nanda, 2011). Higher agreement with wife beating represents a more traditional gender belief system, while disagreement with wife beating represents progressive beliefs. Relevant items from both scales are used to operationalize both indicators in this section. The gender boxes participatory activity in the focus group discussion guide provides complimentary qualitative data. Participants fill out “gender boxes” by writing the qualities, roles, and behaviors expected of a “typical” woman and “typical” man inside the gender box both in general and relative to FGM. They then write what happens when a woman or man does not match what society expects outside of the gender box. The boxes for men and women are then compared and discussed.
All Social Networks indicators focus both on the degree to which FGM is discussed in general, as well as the degree to which participants discus the gender norms upholding FGM (see Table 4). The structured interview tool includes several questions to examine whether participants have discussed FGM and related gender norms (“yes/no” binary format), and if so, how often (scale), and what the most common topics of discussion are (open-ended). Participants are then asked who they discuss FGM with to facilitate measurement of individual and community level social networks (i.e., reference groups). They are then probed for who initiated the discussion to shed light on (1) who in the community is discussing FGM as they may be influential in promoting or abandoning the practice and (2) whether participants feel empowered to initiate conversations. The same questions are then repeated with regards to spousal communication. Data suggests that men and women typically do not discuss FGM, as FGM is often delegated as a women's issue (UNICEF, 2013). However, data also shows that men tend to support FGM abandonment more compared to women (UNICEF, 2013). This presents an opportunity to promote interspousal communication concerning FGM to ultimately bring the practice to an end. Therefore, understanding the nuances of interspousal communication around FGM is an important part of program planning, monitoring, and evaluation.
Social support includes many facets, such as emotional support and empathy, tangible goods and services, information and advice, and feedback and affirmations (Holt-Lunstad and Uchino, 2015). In the ACT framework, social support is operationalized in terms of the number of relationships that offer actual social support in the form of information support (advice) and instrumental support (supplies and services) toward FGM abandonment. In the structured interview tool, participants are asked directly who they turn to and who turns to them for advice and help (beyond advice i.e., supplies, money, transportation) related to FGM in order to establish multi-way networks of social support. If participants list people who have given them advice or help they are probed for what this advice or help entailed and whether it was helpful. All questions in the series are open-ended.
A qualitative, participatory method included in the in-depth interview and focus group discussion guide to capture data for the social networks and social support indicators is social network mapping. Social network maps can take many forms; the maps used in the ACT framework are a series of concentric circles, with the participant in the center. Participants are asked to identify different types of people they discuss FGM with at different levels of the social ecological model (family, peer, community, and social). As participants list types of people, they are recorded in the respective circle. Among these contacts, participants are then probed for who the allies and barriers to communication are and who they would turn to for support regarding FGM. Other probes include who initiated the conversation, whether it was helpful, and what the topics of conversation were.
The final constructs of the ACT framework are Track Individual and Social Change Over Time and Triangulate All Data Analysis. To Track Individual and Social Change Over Time the ACT framework provides sample indicators and means of verification to measure outputs, exposure, and short-term outcomes (see Table 5). The ACT framework can only provide sample indicators and questions because exact indicators and questions will vary by the specific program activities. Researchers can use the indicators and question format by altering the exact activity to match what their program did. For example, changing “advocacy for FGM abandonment” to “meetings with religious leaders.” The final construct, Triangulate All Data Analysis, does not contain indicators but instead provides information on how data triangulation is inherent within the ACT framework and why triangulation is a critical component of M&E.
Output indicators focus on the direct activities of the program, such as the number of radio shows aired, or the number of meetings held with community members. One suggested method provided in the ACT framework for measuring outputs is content analysis, which is a set of techniques to analyze the messages and materials distributed as part of the program (Krippendorf, 2004). The ACT framework also provides information on assessing fidelity, or the extent to which communication activities were implemented according to plan as determined by established benchmarks.
Short-term outcomes focus on whether, and to what extent, the intended audience actually engaged in the communication activities of the program (i.e., with the outputs) (Sood et al., 2019). The sample indicators measuring short-term outcomes are: (1) the number of individuals who have participated in advocacy for FGM abandonment or replacement; (2) the number of individuals who participated in public activities on FGM abandonment or replacement; and (3) the number of communities that made a joint, public pledge to abandon FGM or replace it with an innovation being promoted by communication activities. First participants are asked whether they have ever participated in the communication activity in a binary (“yes/no”) format. If they have, they are then probed using a series of open-ended, self-report items asking them to describe the communication activity, what they did as part of it, and what they did as a result of it. The ACT framework provides information on a qualitative activity called most significant change that can be used to corroborate quantitative findings. In this activity, individuals express what parts of the program had the most impact on their lives and what this impact was (Patton, 2002; Davies and Dart, 2005). The activities that participants identify illustrate the degree to which short-term outcomes were actually achieved with greater nuance than self-reports alone.
The encoded exposure indicators of the ACT framework assess exposure (the extent to which messages actually reached the audience), dose (the degree to which these messages created sustainable affects), and recall (whether participants correctly understood and remembered the information) (Sood et al., 2019). All three are needed to establish attribution and contribution (Sood et al., 2019). In turn, the communication activities of the program may be linked, both directly (attribution) and indirectly (contribution), to what people know, feel, and do, social norms, social networks and social support, and the contextual factors of gender and power. Ultimately, these factors enable program planners to better determine program effectiveness and to refine their efforts to increase FGM abandonment. The questions in this section, like the one above, are provided as examples which researchers will use as a guide by inserting their exact program activities and messages. The structured interview tool contains sample questions for radio, TV, print publications, social media, and interpersonal counseling. Respondents are asked whether they have heard of FGM abandonment through each channel. If they answer yes, they are asked what the name of the program/person/group was, when they last heard FGM abandonment information from that source, and what the information concerned.
The final element of the ACT framework triangulate all data analysis does not contain a set of indicators. Instead, this section includes information on how data triangulation is built into the ACT framework as well as why triangulation is important during M&E. The benefits of triangulation include validation of data, enrichment of data, holistic interpretation of data, and fostering a feedback loop.
Having multiple sources of data for the same indicator is an important way to minimize response bias (such when participants give the socially desirable response rather than what they truly think). This is especially true for FGM because growing public discourse and support for abandonment have driven the practice underground (UNICEF Innocenti Research Centre, 2010). Validating data through multiple means of verification is required to truly explicate the role of social norms regarding FGM abandonment. Such triangulation is built into the ACT framework through the multiple means of verification provided for each indicator. Each indicator can be measured with both quantitative and qualitative means as outlined in the framework. Some questions are also cross-cutting, providing another layer of verification. These relationships are all outlined in the complete ACT package along with how to analyze data to ensure triangulation is optimized throughout data analysis.
In addition to helping validate quantitative data, the participatory qualitative methods provide a level of enrichment not achievable through structured interviews alone. Mixed-methods data provides more nuanced measurement necessary for examining the complexity of social norms. Likewise, participants may be more apt to reveal personal information in the in-depth interview and focus group formats where the use of participatory activities serves to build rapport among facilitators and participants as well as spark ideas participants may have otherwise overlooked.
Using mixed-methods also allows for a more holistic interpretation of the data collected for the various indicators both individually and as a whole. The structured interview tool allows for quantitative analysis of data over time and among specific groups (such as control and intervention) which allows hypotheses to be proven and disproven. However, the participatory activities are cross-cutting meaning they collect data on multiple indicators simultaneously. This allows for gaps between indicators to be revealed and allows the data to tell a holistic story. In turn, data is interpreted subjectively allowing researchers to observe relationships and differences that otherwise might not be evident.
The creation of a feedback loop, where the findings from monitoring and evaluation are fed into future social norms programming, is a final benefit of triangulation. In order for this to occur, it is critical to understand how the approaches and channels adopted by the program directly (attribution) and indirectly (contribution) affect individual and social change. The participatory research activities within the ACT framework offer several strengths with regards to establishing attribution and contribution. First, they allow for tracking change among program audiences and beneficiaries through proxy indicators, in turn measuring the efficacy of programmatic activities. Second, the participatory activities are a mechanism to identify how design and implementation can be improved because they encourage participants to reflect on what worked and did not work and to voice their opinions freely. Several activities described in the Track Individual and Social Change Over Time construct (including the most significant change activity described herein) can be used to assess the degree of implementation, identify outcomes directly attributable to program activities, and, critically, capture the processes by which these results are attained. The ACT framework also includes information for researchers on program planners on how to use the tools overtime from planning through implementation and monitoring and finally evaluation to foster an evidence base which is continually applied to programmatic efforts. Concerning the Joint Program, such data can be shared among countries to gather evidence on the most effective approaches toward ending FGM among a diverse range of populations.
The ACT framework is currently being validated in two countries in Africa where FGM is practiced. Thus, far the framework includes a structured interview tool as well as focus group discussion and in-depth interview guides with several of the participatory, qualitative tools discussed herein. ACT also includes information that can be used by program staff through the research phases to best implement the framework, and to analyze and interpret the data collected so that it may be used to guide future efforts. Following the validation, several meetings will be held with data collectors, joint program staff, and field experts to finalize the tools and framework as a whole. The overarching goal is to create a comprehensive yet adaptable framework to examine the effectiveness of communication approaches to address FGM related social norms, which can serve as a guide for programming across countries and contexts.
The practice of FGM involves a complex mixture of normative influence. Therefore, it is important to utilize multiple social and behavioral theories in developing this macro-level ACT framework. By proposing comprehensive measurement of the conceptual model based on the ACT framework, we hope that communication efforts to address FGM related social norms will better target the social norms and behaviors of the highest impact in any given context. Additionally, given the multiple types of norms and behaviors measured and evaluated, we hope this framework will more descriptively illustrate movement on the continuum of change. Aside from its immediate uses, in the long run, this framework will serve as a means to conceptualize and measure the role of communication efforts to address social norms associated with other harmful traditional practices, most notably child marriage, open defecation, and violence against children. Finally, we hope to contribute to the field of global communication as a whole by examining the role of communication efforts vis a vis attribution and contribution toward social and individual change.
The datasets generated for this study are available on request to the corresponding author.
SSo was the principle investigator and conceived the framework. KK, CL, CC, SSt, and MJ helped refine the framework and are a part of the present validation. SSo, KK, and SSt contributed to manuscript drafting, revision, and approval of the submitted version. RO and TK were involved in the development of the framework and providing expert feedback.
This work was supported through institutional contract #43214515 to Drexel University by UNICEF issued under long term arrangement #42104841.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
We would like to acknowledge UNICEF and UNFPA as well as the UNICEF country offices in Ethiopia and Guinea, all of whom made this work possible.
Ajzen, I. (1991). The theory of planned behavior. Organ. Behav. Hum. Decis. Process 50, 179–211. doi: 10.1016/0749-5978(91)90020-T
Ajzen, I., and Fishbein, M. (1980). Understanding Attitudes and Predicting Social Behavior. Englewood Cliigs, NJ: Prentice-Hall.
Banks, E., Meirik, O., Farley, T., Akande, O., Bathija, H., Ali, M., et al. (2006). Female genital mutilation and obstetric outcome: WHO collaborative prospective study in six African countries. Lancet 367, 1835–1841. doi: 10.1016/S0140-6736(06)68805-3
Bellemare, M. F., Novak, L., and Steinmetz, T. L. (2015). All in the family: explaining the persistence of female genital cutting in West Africa. J. Dev. Econ. 116, 252–265. doi: 10.1016/j.jdeveco.2015.06.001
Bendor, J., and Swistak, P. (2001). The evolution of norms. Am. J. Sociol. 106, 1493–1545. doi: 10.1086/321298
Berg, R. C., and Denison, E. (2012). Interventions to reduce the prevalence of female genital mutilation/cutting in African countries. Camp. Syst. Rev. 9, 1–155. doi: 10.4073/csr.2012.9
Bicchieri, C. (2006). The Grammar of Society: The Nature and Dynamics of Social Norms. New York, NY: Cambridge University Press. doi: 10.1017/CBO9780511616037
Bicchieri, C. (2017). Norms in the Wild: How to Diagnose, Measure, and Change Social Norms. New York, NY: Oxford University Press. doi: 10.1093/acprof:oso/9780190622046.001.0001
Bicchieri, C., and Muldoon, R. (2014). “Social norms,” in The Stanford Encyclopedia of Philosophy, ed E. N. Zalta (Spring). Available online at: https://plato.stanford.edu/archives/spr2014/entries/social-norms/
Brewer, D. D. (2002). Supplementary interviewing techniques to maximize output in free listing tasks. Field Methods 14, 108–118. doi: 10.1177/1525822X02014001007
CARE (2013). WE-MEASR: A New Tool for Measuring Women's Empowerment in Health Programs Technical Update. CARE.
CARE (2017). Applying Theory to Practice: CARE's Journey Piloting Social Norms Measures for Gender Programming. CARE.
Cialdini, R. B., and Melanie, R. T. (1998). Social Influence: Social Norms, Conformity, and Compliance. New York, NY: Oxford University Press, Inc.
Cialdini, R. B., Reno, R. R., and Kallgren, C. A. (1990). A focus theory of normative conduct: recycling the concept of norms to reduce littering in public places. J. Pers. Soc. Psychol. 58, 1015–1026. doi: 10.1037/0022-3514.58.6.1015
Cislaghi, B., Gillespie, D., and Mackie, G. (2016). Values Deliberation and Collective Action: Community Empowerment in Rural Senegal. Palgrave Macmillan.
Cislaghi, B., and Heise, L. (2017). “Measuring Gender-Related Social Norms, Learning Report 1,” in Learning Group on Social Norms and Gender-related Harmful Practices (Baltimore, MD: London School of Hygiene & Tropical Medicine (LSHTM) and STRIVE: Tackling the Structural Drivers of HIV), 2–38. Available online at: http://strive.lshtm.ac.uk/system/files/attachments/STRIVE%20Norms%20Report%201.pdf
Davies, R., and Dart, J. (2005). The ‘Most Significant Change’ (MSC) Technique: A Guide to its Use. Available online at: http://www.mande.co.uk/docs/MSCGuide.pdf
Efferson, C., Vogt, S., Elhadi, A., Ahmed, H. E. F., and Fehr, E. (2015). Female genital cutting is not a social coordination norm. Science 349, 1446–1447. doi: 10.1126/science.aaa7978
El-Damanhoury, I. (2013). The Jewish and Christian view on female genital mutilation. Afr. J. Urol. 19, 127–129. doi: 10.1016/j.afju.2013.01.004
Evans, W. D., Donahue, C., Snider, J., Bedri, N., Elhussein, T. A., and Elamin, S. A. (2019). The Saleema initiative in Sudan to abandon female genital mutilation: outcomes and dose response effects. PLoS ONE 14:e0213380. doi: 10.1371/journal.pone.0213380
Gastaldo, D., Magalhães, L., Carrasco, C., and Davy, C. (2012). Body-Map Storytelling as Research: Methodological Considerations for Telling the Stories of Undocumented Workers Through Body Mapping. Available online at: http://www.migrationhealth.ca/undocumented-workers-ontario/body-mapping (accessed August 15, 2016).
Gillespie, D., and Melching, M. (2010). The transformative power of democracy and human rights in nonformal education: the case of tostan. Adult Educ. Q. 60, 477–498. doi: 10.1177/0741713610363017
Gillespie, G. (2013). Tostan FAQ: FGC vs. FGM. Available online at: https://www.tostan.org/tostan-faq-fgc-vs-fgm/ (accessed April 3, 2020).
Hillenbrand, E., Mohanraj, P., Karim, N., and Wu, D. (2015). Measuring Gender-Transformative Change: A Review of Literature and Promising Practices CARE. Available online at: https://www.care.org/sites/default/files/documents/working_paper_aas_gt_change_measurement_fa_lowres.pdf
Holt-Lunstad, J., and Uchino, B. N. (2015). “Social support and health,” in Health Behavior: Theory, Research, and Practice, 5th Edn, eds K. Glanz, B. Rimer and K. Viswanath (San Francisco, CA: Jossey-Bass), 183–204.
Ibrahim, A. H., Belay, D. G., Tiruneh, A. Z., and Kia, T. T. (2018). Social and health risks of female genital mutilation for medication and braveness. Int. J. Risk Conting. Manage. 7, 20–36. doi: 10.4018/IJRCM.2018010102
Institute for Reproductive Health (2019). Resources for Measuring Social Norms: A Practical Guide for Program Implementers. Washington, DC: Learning Collaborative to Advance Normative Change.
Kandala, N. B., and Komba, P. N. (2015). Geographic variation of female genital mutilation and legal enforcement in sub-Saharan Africa: a case study of Senegal. Am. J. Trop. Med. Hyg. 92, 838–847. doi: 10.4269/ajtmh.14-0074
Kincaid, D. L. (2000). Social networks, ideation, and contraceptive behavior in Bangladesh: a longitudinal analysis. Soc. Sci. Med. 50, 215–231. doi: 10.1016/S0277-9536(99)00276-2
Kincaid, D. L. (2004). From innovation to social norm: bounded normative influence. J. Health Commun. 9(Suppl. 1), 37–57. doi: 10.1080/10810730490271511
Kincaid, D. L., and Figueroa, M. E. (2004). “Ideation and communication for social change”, in Health Communication Partnership Seminar.
Kincaid, D. L., Figueroa, M. E., Storey, D., and Underwood, C. R. (2007). A Social Ecology Model of Communication for Social and Behavioral Change: A Brief Summary. Baltimore, MD: Johns Hopkins University Bloomberg School of Public Health, Center for Communication Programs.
Kincaid, D. L., Figueroa, M. E., Storey, J. D., and Underwood, C. R. (2006). “Attitude, ideation, and contraceptive behaviour: the relationships observed in five countries,” in Proceedings: World Bank Congress on Communication for Development (Rome).
Krippendorf, K. (2004). Content Analysis: An Introduction to its Methodology. Thousand Oaks, CA: Sage Publications.
Lapinski, M. K., and Rimal, R. N. (2005). An explication of social norms. Commun. Theory 15, 127–147. doi: 10.1111/j.1468-2885.2005.tb00329.x
LeJeune, J., and Mackie, G. (2008). Social Dynamics of Abandonment of Harmful Practices: A New Look at the Theory. Florence: UNICEF Innocenti Research Centre.
Mackie, G. (1996). Ending footbinding and infibulation: a convention account. Am. Sociol. Rev. 61, 999–1017. doi: 10.2307/2096305
Mackie, G. (2000). Female genital cutting: the beginning of the end, in Female Circumcision in Africa: Culture, Controversy and Change, eds B. Shell-Duncan and Y. Hernlund (Boulder, CO: Lynne Rienner Publishers), 253–281.
Mackie, G., Moneti, F., Shakya, H., and Denny, E. (2015). What are Social Norms? How are They Measured? San Diego, CA: UNICEF/University of California San Diego Center on Global Justice.
Marcus, R., and Harper, C. (2015). Social Norms, Gender Norms and Adolescent Girls: A Brief Guide. Knowledge to action resource series: ODI. ODI.
Measure Evaluation (n.d). Participation of Women in Household Decision-Making Index. Available online at: https://www.measureevaluation.org/prh/rh_indicators/crosscutting/wgse/participation-of-women-in-household-decision (accessed April 5, 2020).
Miller, D. T., Monin, B., and Prentice, D. A. (2000). “Pluralistic ignorance and inconsistency between private attitudes and public behaviours,” in Attitudes, Behaviours and Social Context: The Role of Social Norms and Group Membership, eds D. J. Terry and M. A. Hogg (Mahwah, NJ: Lawrence Erlbaum Associates, Inc.), 95–114. doi: 10.4324/9781410603210-6
Morison, L., Sherf, C., Ekpo, G., Paine, K., West, B., Coleman, R., et al. (2001). The long-term reproductive health consequences of female genital cutting in rural Gambia: a community-based survey. Trop. Med. Int. Health 6, 643–653. doi: 10.1046/j.1365-3156.2001.00749.x
Osterwalder, A., and Pigneur, Y. (2010). Business Model Generation. Hoboken, NJ: John Wiley & Sons, Inc.
Patton, M. Q., (ed.). (2002). “Particularly appropriate qualitative applications,” in In Qualitative Research & Evaluation Methods. (Thousand Oaks, CA: SAGE), 196–197.
Petit, V., and Zalk, T. N. (2019). Everybody Wants to Belong: A Practical Guide to Tackling and Leveraging Social Norms in Behavior Change Programming. New York, NY: UNICEF.
Population Council (2016-2017). Evidence to end FGM: Research to help girls and women thrive in Study Summaries. Population Council.
Rimal, R. N. (2008). Modeling the relationship between descriptive norms and behaviors: A test and extension of the theory of normative social behavior (TNSB). Health Commun. 23, 103–116. doi: 10.1080/10410230801967791
Rimal, R. N., and Lapinski, M. K. (2015). A re-explication of social norms, ten years later. Commun. Theor. 25, 393–409. doi: 10.1111/comt.12080
Rimal, R. N., and Real, K. (2005). How behaviors are influenced by perceived norms: a test of the theory of normative social behavior. Commun. Res. 32:389–414. doi: 10.1177/0093650205275385
Rosenstock, I. M. (1974). The health belief model and preventive health behavior. Health Educ. Monogr. 2, 354–386. doi: 10.1177/109019817400200405
Shell-Duncan, B., Hernlund, Y., Wander, K., and Moreau, A. (2010). Contingency and Change in the Practice of Female Genital Cutting: Dynamics of Decision Making in Senegambia. Geneva: World Health Organization.
Shell-Duncan, B., Wander, K., Hernlund, Y., and Moreau, A. (2011). Dynamics of change in the practice of female genital cutting in Senegambia: testing predictions of social convention theory. Soc. Sci. Med. 73, 1275–1283. doi: 10.1016/j.socscimed.2011.07.022
Shell-Duncan, B., Wander, K., Hernlund, Y., and Moreau, A. (2013). Legislating change? Responses to criminalizing female genital cutting in Senegal. Law Soc. Rev. 47, 803–835. doi: 10.1111/lasr.12044
Sood, S., Cronin, C., Sengupta, A., Stevens, S., Gordon, M., Figueroa, N., et al. (2019). Technical Guidance for Communication for Development Programmes Addressing Violence Against Children. New York, NY: UNICEF.
Storey, D., and Figueroa, M. E. (2012). “Toward a global theory of health behavior and social change,” in The Handbook of Global Health Communication, eds R. Obregon and S. Waisbord (Hoboken, NJ: Wiley Blackwell), 70–94. doi: 10.1002/9781118241868.ch4
Ulin, P. R., Robinson, E. T., and Tolley, E. E. (2005). Qualitative Methods in Public Health. San Francisco, CA: Jossey-Bass.
UNFPA (2016). Female genital mutilation [FGM] frequently asked questions. Available online at: https://www.unfpa.org/resources/female-genital-mutilation-fgm-frequently-asked-questions#banned_by_law (accessed April 3, 2020).
UNFPA (2019). Female Genital Mutilation [FGM] Frequently Asked Questions. Available online at: https://www.unfpa.org/resources/female-genital-mutilation-fgm-frequently-asked-questions#linkages_fgm_hiv (accessed April 4, 2020).
UNICEF (2013). Female Genital Mutilation/Cutting: A Statistical Overview and Exploration of the Dynamics of Change. New York, NY: UNICEF.
UNICEF Innocenti Research Centre (2010). The Dynamics of Social Change Towards the Abandonment of Female Genital Mutilation/Cutting in Five African Countries. Available online at: https://www.unicefirc.org/publications/pdf/fgm_insight_eng.pdf
United Nations Population Fund and United Nations Children's Fund (2015). UNFPA and UNICEF Joint Programme on Female Genital Mutilation/Cutting: Accelerating Change. Annual Report. Available online at: http://www.unfpa.org/publications/2015-annual-report-unfpa-unicef-jointprogramme-female-genital-mutilationcutting (accessed April 29, 2020).
Weller, S. C., and Romney, A. K. (1988). Systematic Data Collection. Newbury Park, CA: Sage Publications. doi: 10.4135/9781412986069
World Health Organization (2012). Understanding and Addressing Violence Against Women: Female Genital Mutilation. World Health Organization.
Keywords: female genital mutilation, harmful traditional practices, social norms, social and behavior change communication, conceptual framework, measurement and evaluation framework
Citation: Sood S, Kostizak K, Lapsansky C, Cronin C, Stevens S, Jubero M, Kilbane T and Obregon R (2020) ACT: An Evidence-Based Macro Framework to Examine How Communication Approaches Can Change Social Norms Around Female Genital Mutilation. Front. Commun. 5:29. doi: 10.3389/fcomm.2020.00029
Received: 26 February 2020; Accepted: 16 April 2020;
Published: 02 June 2020.
Edited by:
Iccha Basnyat, James Madison University, United StatesReviewed by:
Tobias Reynolds-Tylus, James Madison University, United StatesCopyright © 2020 Sood, Kostizak, Lapsansky, Cronin, Stevens, Jubero, Kilbane and Obregon. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Suruchi Sood, c3MzNzI0QGRyZXhlbC5lZHU=
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.