 Oliver Wedderhoff
Oliver Wedderhoff Anita Chasiotis
Anita Chasiotis Tom Rosman
Tom Rosman Anne-Kathrin Mayer
Anne-Kathrin Mayer- Leibniz Institute for Psychology Information, Trier, Germany
Although there is a multitude of taxonomies of health information sources, these taxonomies only partly include how information users classify these sources. The present paper complements this research by developing a taxonomy which is based on individuals' subjective perceptions of the “universe” of health information sources. In our study, nine non-redundant sources of health information were presented to N = 150 participants who rated all 36 possible combinations of source pairs regarding their perceived similarity. Results of non-metric multidimensional scaling suggested three basic dimensions underlying the similarity ratings: “expertise” (lay vs. professional), “interaction” (interpersonal vs. impersonal), and “accessibility” (low vs. high). Thus, the wide array of health information sources can be structured by means of the new taxonomy arranging them on three dimensions. This allows researchers to classify each source and with this, to draw on common ground when interpreting the varying use of health information sources.
Introduction
When experiencing a health problem, a fundamental need for health information arises. In today's information society, individuals are confronted with a wide range of potential information sources they can turn to (Johnson and Case, 2012). A vast body of research exists on individuals' health information seeking behavior with regard to the preference for specific sources of health information (e.g., Dutta-Bergman, 2004; Rutten et al., 2005, for a review; Pecchioni and Sparks, 2007; Smith, 2011; Dobransky and Hargittai, 2012). In this line of research, seeker characteristics, such as sociodemographic or personality variables, are at the researchers' main focus. Various prediction models for the perception or use of specific sources have been tested (e.g., doctor, nurse, dietician, and homeopath; Lawson et al., 2011; books, magazines, brochures, and newspapers; Marrie et al., 2013). For example, Blanch-Hartigan and Viswanath (2015) showed that higher education levels are associated with more use of the internet and support organizations as sources of health information.
While this approach undoubtedly provides meaningful insights on a micro-level, it suffers from a few shortcomings. First, to generalize and contrast the results of different studies, a common basis for the objects under observation is required. One way to achieve this could be the same selection of information sources in each study. In the scientific practice, however, this can be hardly implemented. Since there are countless possibilities to obtain health information, it is nearly impossible to include every existing source. Therefore, researchers are forced to consider a selection of sources or build umbrella terms with varying degrees of abstraction. This selection and chosen abstraction level is often driven by the context determined by the research question (e.g., Lariscy et al., 2010), which is why the range of sources is always somewhat arbitrary. A possible solution would be to look at the sources on a more general level. There have already been various approaches to this, such as Lu and Yuan (2010). However, we argue that these distinctions should rather be based on the user's point of view. Researchers ultimately want to predict the behavior of the user, which is why the subjective perception should be used to differentiate the objects of observation relevant to individual behavior. An additional benefit of such an approach would be the consideration of further research questions, which could not be answered by approaches mostly used so far. In fact, knowing that a specific source of information is preferred does not imply knowing why this is the case, i.e., to understand which source-immanent features—besides personality variables, prior experience, or situational context factors—drive this preference and how interindividual differences in preferred source types may be explained. Also, from an application-oriented perspective, it is essential to know why individuals prefer and use specific sources of health information in particular situations in order to be able to provide information tailored to an individual patient's needs.
In the field of communication research, the comprehensive model of information seeking (CMIS; Johnson and Meischke, 1993) can be used as a starting point to further investigate the perception of health information sources, as it is one of the most established models of information seeking and source selection. The model distinguishes between two categories that are relevant for the users' selection of a particular health information source: (1) factors associated with features of sources, for example the comprehensiveness and utility, and (2) factors associated with users, for example demographics and psychological needs. Previous approaches largely neglected the interaction between both categories and thus did not consider factors of users and sources simultaneously. In line with this, (Zhang, 2014, p. 913) points out that, “[…] most studies used the survey method, in which a list of predefined factors or criteria was provided for users to select. Thus, limited information about users' interpretations of the factors and criteria […] could be gained. […] As a result, more research is needed to achieve a systematic and comprehensive understanding of consumers' source selection behavior in health information searching.”
The uses-and-gratification-theory (UAGT; Katz et al., 1973-1974) has also provided a substantial contribution to a deeper understanding of the interaction between media and its users. A central assumption of UAGT is that much initiative in linking gratification and media exposure lies with the user. Consequently, the focus should be shifted even more toward information users and their subjective perceptions, which are highly relevant in the autonomous decision making processes in modern health contexts. Furthermore, UAGT suggests that the reasons of media use should be assessed from the users' perspective. Accordingly, there are a number of studies on individual needs and reasons for using particular health information sources based on theoretically derived relevant source characteristics, (e.g., Ruppel and Rains, 2012). However, it is pertinent to take into account not only phenomenological source characteristics, but also subjective perceptions of these sources and their role in how individuals themselves categorize the “universe” of health information sources. As it could turn out that specific sources may be very similar on a phenomenological level, but nevertheless perceived differently by the users, this is also of practical relevance. In the worst case, this could lead to recommendations of sources or conceptions of interventions, which are based on inaccurate assumptions of their user's needs.
As previously mentioned, a more generalized view on how individuals perceive different health information sources, by means of a typology of their subjective properties, would address these problems. With this, future research could draw conclusions from data which are comparable since they are based on a common ground. Findings would be more generalizable and study concepts could be replicated in and transferred to varying contexts, without the risk of omitting context specific sources. Moreover, by using a taxonomy, a researcher does not have to make extra assumptions about which sources she wishes to integrate in her study. Another disadvantage of traditional approaches is that new sources may emerge while existing sources can change or may even disappear over time. A taxonomy, in contrast, is largely independent of time. While this argument is also valid for theoretically derived taxonomies, it may be even more so for their empirical counterparts since the risk of different researchers coming to different conclusions on how to classify information sources is reduced. Furthermore, in line with the CMIS, a taxonomy should well-benefit from integrating information users' subjective perceptions. In fact, the CMIS suggests that information carrier factors and seeker-related antecedents are to be taken into account simultaneously, and we strongly agree with this point. Not least, on a methodological level, the identification of such dimensions would enable researchers to make use of more sophisticated statistical procedures because source properties can be conceived as interval-scaled rather than nominal-scaled (as is the case with non-aggregated sources).
Against this background, the basic idea guiding our research is that individuals will prefer certain information sources because of specific source properties that are seen through the “lens” of their individual perceptions. Following this rationale, it should be possible to characterize each information source by the value individuals attribute to it on a limited number of source dimensions. Identifying the relevant source features and assessing the preference of individuals for these features might then help, on a broader level, to explain information users' preferences for specific sources. For example, a relevant generalized source feature might be its “interpersonal” character, i.e., the amount of social interaction the use of a specific source implies (e.g., Zimmer et al., 2007). If, in threatening situations, people report a preference for highly interactive information, one would expect them to prefer sources which enable real interaction (e.g., with family, friends or professionals) or virtual interaction, e.g., on internet platforms. Therefore, health practitioners might benefit from knowing which basic properties of information sources motivate individuals to choose specific sources, too. Their knowledge would enable them to provide information or recommend specific sources that fit the individual's preferences and needs. If, for example, a person reports a preference for information which is highly accessible, practitioners should recommend information sources which are easy to use, or provide the relevant information directly instead of leaving the process of information seeking to the individual.
Following this line of reasoning, identifying the basic dimensions underlying the subjective perception of health information sources is crucial when striving for a meaningful and comprehensible interpretation of individual preferences for particular sources. On a basic level, information sources have been categorized by surface features such as online/offline or human/computerized. For example, Rains (2007) differentiates between the use of the internet on the one hand, and the use of “traditional” health information sources such as doctors and family on the other hand. Similarly, Hall et al. (2015) compare “users” and “nonusers” of online health information. Redmond et al. (2010) investigate participants' preventive health behavior depending on their use of two groups of information sources: “multimedia” and “interpersonal.” However, these categorizations do not take into account individuals' subjective conceptualization of sources. While they are doubtlessly plausible from a phenomenological point of view, it remains unclear whether they correspond to participants' perceptions of the sources.
The same pertains to other existing approaches which have tried to classify health information sources based on theoretical considerations (Gray et al., 2005; e.g., Lu and Yuan, 2010; Zhang, 2014). Most of these approaches, for example, agree that “quality of information” is a dimension of major importance. However, further dimensions vary considerably with regard to number, contents, and level of abstraction, including for example, relevance, usefulness, usability, trustworthiness, credibility, previous experience, and saliency (Gray et al., 2005; Zhang, 2014). Thus, approaches which are mainly based on theoretical considerations bear the risk of low comparability due to differing foci and levels of abstraction. An integrated taxonomy based on subjective perceptions would help to reduce this risk.
Therefore, the present paper aims at developing an empirically based taxonomy of health information sources that takes into account information users' subjective perceptions that they use to structure the “universe” of health information sources. Our study investigated the following research question:
Which are the basic feature dimensions underlying individuals' perceptions of health information sources? In our study, using a rigorous methodological approach, we aim at empirically identifying these subjective dimensions. By asking individuals to rate pairs of health information sources with regard to their perceived similarity, a set of distance measures (where a small distance means two sources are perceived as similar) was created that includes every possible pairwise combination of sources from a predefined set. Based on the perceived distances, sources can then be arranged on various dimensions. Multidimensional scaling (MDS; Torgerson, 1952; Kruskal and Wish, 1990) is a prominent statistical method to deal with distance measures when aiming to arrange objects (e.g., information sources) on dimensions so that they best fit the data.
Although other studies already provide useful theoretically derived dimensions to classify health information sources (e.g., Gray et al., 2005; Lu and Yuan, 2010; Zhang, 2014), to our knowledge, none has yet derived them on an empirical basis by considering individuals' perceptions of source similarity vs. dissimilarity. Thus, we aimed at complementing theoretical classifications of health information sources by providing empirical evidence for the categories and/or dimensions proposed by them. For this purpose, we implemented exploratory multidimensional scaling to empirically identify basic dimensions of health information sources underlying individuals' judgements about the pairwise similarity of health information sources.
Materials and Method
Participants and Procedure
Data were collected in an unsupervised online study on health information behavior. Participants were recruited via a mailing list of a large German university as well as via Facebook groups which aim at recruiting experimental subjects in psychology studies. The final sample included N = 150 participants with an age range from 19 to 60 years (M = 27.13, SD = 7.27 years). 66.7 percent of the participants were females. Survey completion took about 90 minutes. Participants received a 15 € (about 18 $) coupon for an online shop as compensation.
In accordance with the German Research Foundation (Deutsche Forschungsgemeinschaft, DFG) guidelines an ethics approval was not necessary (DFG, 2018). All study measures and methods were in compliance with the Declaration of Helsinki and the APA Ethics Code (American Psychological Association, 2002). Since the study was conducted online, no written informed consent could be obtained. However, we provided an information sheet and consent form (for download) and subjects were only allowed to enter the study if they confirmed (by checking a box) that they agreed to the conditions specified in these documents.
Measurement of Source Similarity
To determine the underlying basic dimensions of health information sources, it is necessary to decide on a selection of sources for the subsequent similarity rating. First, four experts (three authors of the present paper and one additional researcher) in the field of health information literacy named all sources of health information they could think of. (Nearly) identical sources with different labels were merged (e.g., “acquaintances” and “colleagues”). Finally, the remaining sources were summarized into broader entities (e.g., journal papers, medical textbooks and guidebooks were subsumed under the label “textbooks”) with the aim of keeping the final pool of relevant sources non-redundant but as diverse as possible. Based on the experts' judgement, we included nine health information source categories in our study (see Table 1). To keep the conceptualization of sources as consistent as possible across participants, each of the nine sources was supplemented with at least one specific example (see Table 1).
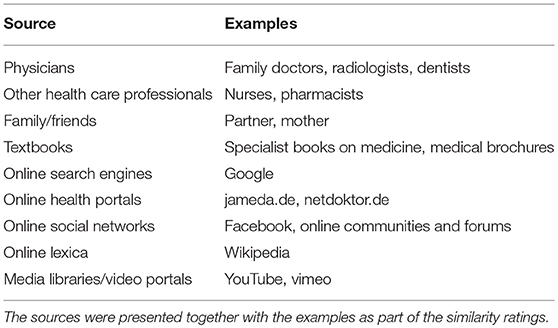
Table 1. Health information sources.
All possible pairwise combinations of the nine health information sources (i.e., n*[n-1]/2, thus, 36 pairs) had to be rated on a 7-point rating scale with regard to their perceived similarity (e.g., “How similar are physicians to textbooks as sources of health information?”). Low scale values indicated no or only a slight similarity.
Statistical Analysis
We used non-metric MDS to identify underlying dimensions of the perception of health information sources. MDS uses similarity data to map the compared objects (i.e., sources) in an n-dimensional space, aiming at maximizing data fit: The objects are iteratively arranged on n dimensions to reproduce the similarity ratings as accurately as possible. Thereby, both exploratory and confirmatory approaches are possible, i.e., the number of dimensions (the MDS solution) and their interpretation can be determined in advance or retrospectively (Borg and Groenen, 2005). The decision in favor of a particular MDS solution should be driven by theoretical explanations as well as by statistical indicators (Borg and Staufenbiel, 2007). With regard to the latter, the so called “stress measure” (Kruskal, 1964) is pertinent: It quantifies the deviation of objects arranged on the dimensions in the MDS solution from their “ideal” position in a solution with perfect fit to the data. Thus, the smaller the stress indicator, the better the fit. Kruskal (1964) provides a rule of thumb to facilitate the evaluation of the stress index. Accordingly, an index around 0.20 is regarded as poor, around 0.10 as fair, around 0.05 as good, around 0.025 as excellent and equal to 0 as perfect. With an increasing number of dimensions, the stress measure will decrease (i.e., the fit will improve). In order to assess the ideal configuration, a Scree plot of the stress indexes should be investigated (Cattell, 1986). By determining the point at which the resulting curve begins to level off, the appropriate number of dimensions can be identified.
In the present study, exploratory MDS was used because it was impossible to derive a hypothesis on the number of subjective source dimensions. To determine the visual configuration and the underlying dimensions of the information sources, we used the ALSCAL program by Young et al. (1978) implemented in SPSS. We first created a dissimilarities matrix by computing the perceived differences between the pairs of information sources. By means of non-metric MDS analysis, these dissimilarities were transferred into Euclidean distances. A rank order of these distances was then arranged for each source.
Results
Table 2 depicts the descriptive statistics of the perceived source similarities for each pairwise combination.
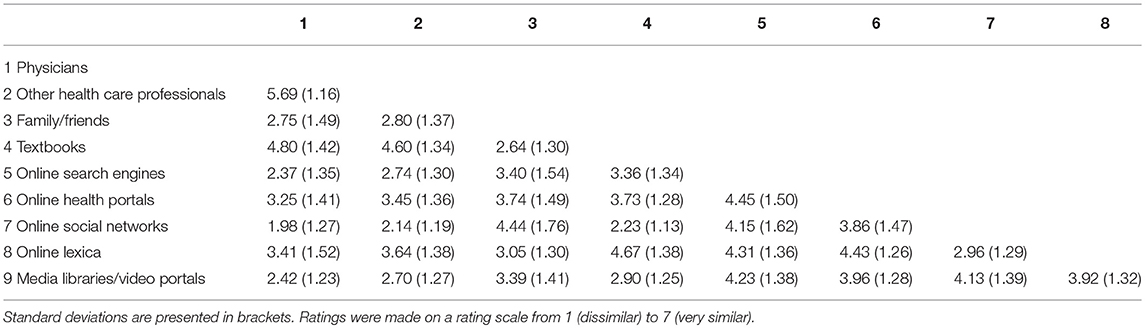
Table 2. Means and standard deviations of the pairwise similarity ratings of health information sources.
In order to determine the ideal number of dimensions, we first conducted a Scree test by plotting the stress indexes for all four configurations (Cattell, 1986). While the stress index of 0.224 for the one-dimensional solution was poor, it dropped to a “fair” value of 0.105 and reached a “good” value of 0.39 for the three-dimensional solution which did not improve markedly for the four-dimensional solution (“stress” = 0.015). Hence, the scree plot suggests a three dimensional classification of health information sources. The three-dimensional configuration of the information sources is depicted in Figures 1–3: Figure 1 displays the first and second dimension, and Figure 2 represents the second and third dimension. Figure 3 shows all three dimensions compiled in a three-dimensional graph.
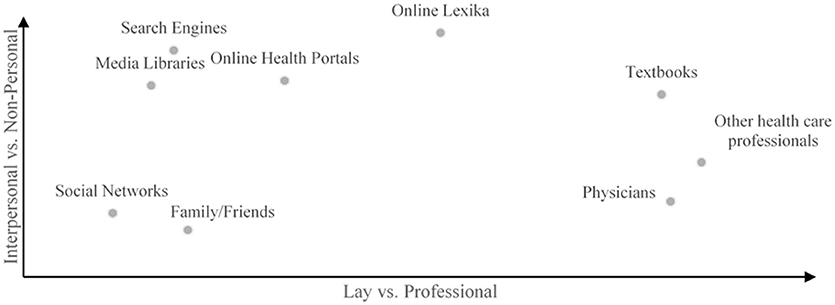
Figure 1. Configuration of the nine health information sources along the dimensions one and two of the three-dimensional solution derived from the MDS.
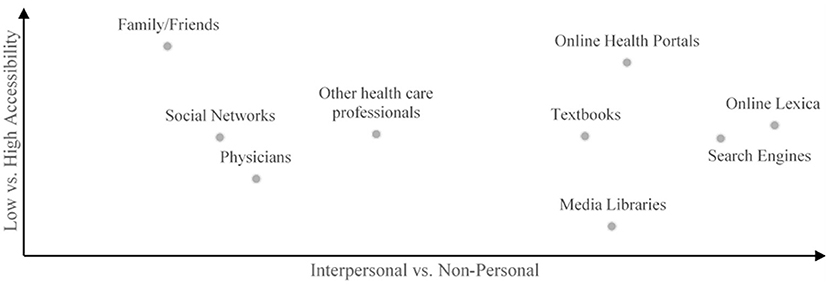
Figure 2. Configuration of the nine health information sources along the dimensions two and three of the three-dimensional solution derived from the MDS.
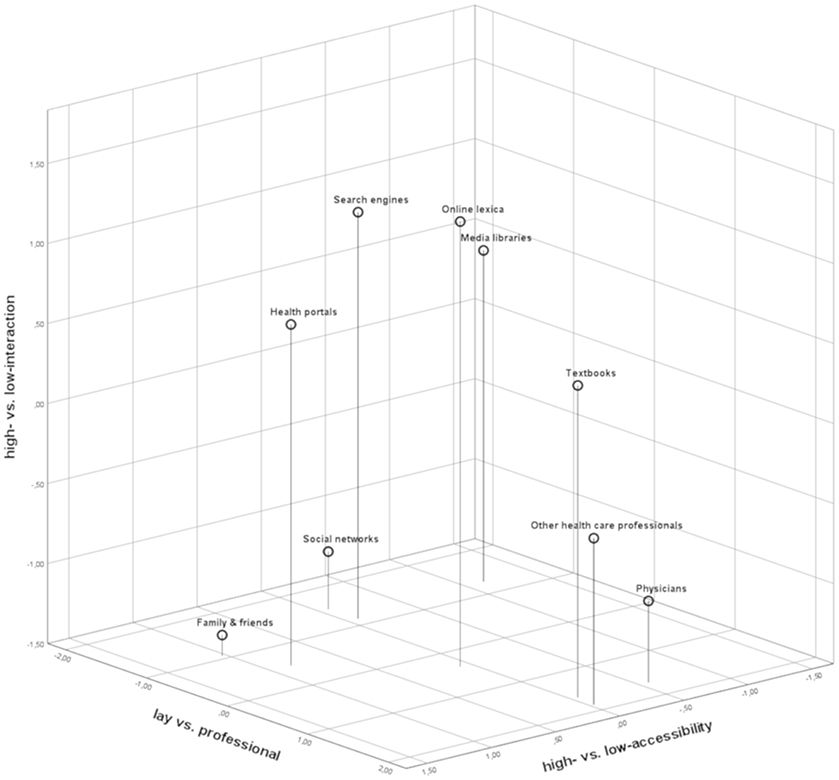
Figure 3. Configuration of the nine health information sources in a three-dimensional room as created by the final MDS solution.
To ensure that the three-dimensional classification is not only empirically adequate but also theoretically interpretable, four judges familiar with the research field of health information seeking discussed the preferred solution in comparison to the two- and four-dimensional solution and agreed on labeling the dimensions. As can be seen in Figure 1 (horizontal axis), the sources mapped at the end points of dimension 1 (“other health care professionals” and “physicians” vs. “social networks” and “family/friends”) indicate source differences with regard to the level of the professional background. Therefore, dimension 1 was labeled “expertise” and distinguishes between the endpoints “laypeople's knowledge” vs. “professionals' knowledge.”
Inspection of the configurations in Figures 1, 2 suggests to discriminate two groups of sources on dimension 2. One group of sources requires (or enables) face-to-face or computer-mediated social interaction, while the other can (or needs to) be explored all by oneself to get the desired information. Consequently, we chose the label “interaction” for this dimension with the endpoints “interpersonal” and “impersonal.” Concerning dimension 3 (see Figure 2), the interpretation was slightly less straightforward. On the end points of this dimension, the sources “family/friends” and “online health portals” stand in contrast to online media libraries and physicians. The main difference between these source types seems to lie in time and effort necessary to consult these information sources when facing a health problem, and, thus, in the accessibility of the specific information needed. Family and friends, for example, as well as online portals are easily accessible and their consultation does not imply barriers like making an appointment (which is the case with physicians). Similarly, extracting and aggregating information from a complex and heterogeneous sample of materials to obtain the desired information in a condensed format (which is the case when searching media channels like YouTube or using search engines) is not necessary. Accordingly, we labeled this third dimension “accessibility” with the endpoints “high/easy” vs. “low/difficult.”
The corresponding classification, which is based on our participants' subjective perceptions of the “universe” of health information sources, is depicted in Table 3.
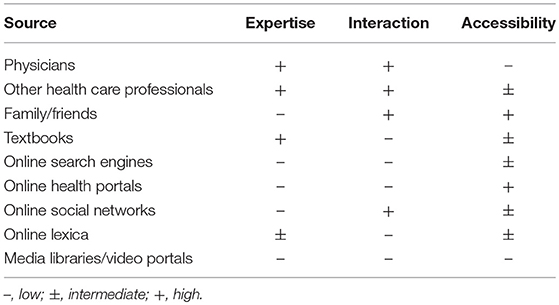
Table 3. Classification of health information sources according to the taxonomy.
Discussion
The aim of the present paper was to examine whether numerous health information sources may be empirically combined into a parsimonious taxonomy reflecting their subjective similarity. Therefore, we assessed perceptions of similarity with regard to nine relevant and non-redundant sources of health information and used a multidimensional scaling approach to identify dimensions which—from participants' view—are used to structure the “universe” of health information sources. Our results suggest that individuals implicitly or explicitly categorize health information sources along three basic and independent dimensions. These dimensions allow to distinguish between all types of health information sources with regard to the “expertise” they reflect, the amount of personal “interaction” their use implies, and their “accessibility.” Future research referring to these dimensions would thus be based on an empirically derived differentiation between sources. In this sense, our taxonomy usefully complements existing theoretical models of health information seeking by contributing empirically derived, and thereby subjectively relevant source dimensions, which can be integrated into existing theoretical models. In the CMIS (Johnson and Meischke, 1993; see above), for example, information carrier factors (i.e., characteristics and utilities), are considered as mediating the impact of seeker characteristics (such as experience and beliefs) on health information seeking actions (scope, depth, persistence). With the help of our taxonomy, it is now possible to specify the characteristics individuals refer to in order to differentiate between information carriers. As a consequence, the resulting information seeking actions encompassed by the model can be predicted and explained more precisely. A source characterized by high accessibility, low expertise and high interaction, for example, may elicit a specific seeking action pattern which is different from seeking behavior induced by another combination of source characteristics. In this case, the search can be hypothesized to be rather shallow and short with a broad scope, dependent on topics the interactive search process may bring up.
Another example is the Risk Information Seeking and Processing Model (RISP; Griffin et al., 1999). Here, perceived source characteristics are also an integral model component, however, only as moderators of the effect of information sufficiency on information behavior and processing. Similar to the possible application of our taxonomy exemplified in the CMIS, in the RISP, the characteristics we identified as individual means of differentiating between health information sources could be considered separately as such moderators.
The novelty of our study lies in the bottom-up approach of identifying distinctive features from the users' point of view, rather than on a phenomenological basis. In doing so, our aim was not to establish a wholly new taxonomy, but to complement and perhaps confirm already established classifications by taking the users' views into account. This includes, for example, a study by Lu and Yuan (2010), where three source attributes are considered as main factors influencing source selection: quality, accessibility, and a relational vs. non-relational-dimension. Accordingly, in a literature review of theoretically derived characteristics of health information sources that influence source selection, Zhang (2014) identifies four criteria, accessibility, quality, usability, and interactivity. Apparently, these criteria are very similar to the basic dimensions we identified as constituting the “universe” of health information sources based on users' perceptions. In contrast, in another study (Gray et al., 2005), experience, saliency and credibility were identified as the three core characteristics of health information sources from the literature. Evidently, when drawing on relevant source characteristics that have been derived from the literature by studies in which they had been proposed and then empirically tested in a specific context, researchers may come to varying conclusions with regard to the most decisive source characteristics. This is not surprising and in itself not problematic as different contexts and situations elicit different evaluations with regard to the relevance of some characteristics. At this point, our approach enables researchers to integrate these–at first sight–conflicting results. As we considered the users' perspective by implementing similarity judgements, we were able to ensure identifying basic, situation-independent characteristics individuals use to differentiate between health information sources in general. Credibility, saliency, and experience, on the other hand, are characteristics that build upon these basic ones and come into effect and are relevant to individuals in specific, narrowly defined situations. For example, a source might be high in expertise, and therefore, one deems it credible (this does not work the other way round). One also might find it more or less important with regard to a current information need, which results in its actual saliency. Because it is also high in personal interaction and accessible (and these are characteristics one might prefer), one might have considerable experience in using it. Thus, the basic dimensions we identified may constitute a comprehensive hermeneutic foundation that further relevant perceived characteristics are derived from. To sum up, these fundamental characteristics provide a fertile ground for other, equally relevant source properties, which, however, are either context-specific or can be deduced directly from the basic characteristics we identified.
The first dimension, “expertise,” has also been theoretically proposed by Morrison and Vancouver (2000), and focuses on differences in perceived level of professional qualification which is reflected by a health information source. People with no medical background (e.g., family/friends) are located at one end of this dimension, whereas healthcare professionals are assigned to the other end. You would not expect your best friend to be able to explain the medical background and causes for your recently diagnosed diabetes. To acquire this kind of information, affected individuals tend to see a physician or look up the relevant literature (Longo et al., 2010). However, when experiencing rather common and/or chronic symptoms (e.g., lower back problems), it can be helpful to get information from people with similar conditions, e.g., about their ways of coping with the symptoms (e.g., Hartzler and Pratt, 2011; Powell et al., 2011). The empirically driven identification of this subjective dimension might prove useful to predict and explain health information behavior. If, for example, a person scores high on this dimension and for this reason, tends to visit a health professional even when experiencing symptoms that are commonly known as harmless, researchers and practitioners would know one possible reason why this is the case (the person wants to receive professional information about the problem). This person could, for example, be helped by providing professional information material that can be accessed at home, ultimately rendering some visits to the doctor for mere information purposes unnecessary.
The second dimension has already been theoretically proposed by Zimmer et al. (2007). It focuses on the necessity to interact with others in order to obtain the desired information, either by direct face-to-face interaction or by the use of miscellaneous information technologies. Communicating with strangers via online social networks still requires social interaction, although perhaps not as much as the direct conversation with a physician during an appointment. On the other hand, it is possible to gather health information without any personal interaction at all (e.g., from a textbook or traditional media). The distinction between sources requiring more or less social interaction is especially valuable with regard to sensitive and potentially “shameful” health issues. It is, for example, much less stressful for someone to look up information about symptoms of a sexually transmitted disease online and anonymously than to consult a physician (Gray et al., 2002; Magee et al., 2012). Furthermore, individuals could be willing to search for information on their own without requiring any interaction because they have been disappointed by previous personal interactions with potential information carriers. Accordingly, Tustin (2010) found that individuals were more likely to browse online for health information the lower they rated the perceived empathy of their physician and the quality of time they spent talking to them. Powell et al. (2011) also found that anonymity was one of the main reasons to search for health information and discuss health issues online, although individuals were mostly aware of some significant shortcomings of accessing information online, like the questionable trustworthiness of some sources. Thus, the possibility to avoid personal face-to-face interaction in some health contexts appears to be relevant. As with the first dimension, the identification of this subjective dimension could prove useful for the prediction and explanation of health information behavior. If, for example, a person experiencing some serious symptoms prefers to acquire health information via online social networks, one might argue that this is because she probably is a “digital native” and likes to surf the internet. However, as this person scored high on the “interaction”-dimension and might therefore try to connect with others via social networks, one could try to meet the needs of this person by providing (online) personal contact with health professionals. Thereby, perhaps, potential negative attitudes toward professionals that may have emerged because of previous dissatisfying interactions (see above) could be modified. A prominent example in Germany is an online platform called “washabich.de” (“What disease do I have?”) where trained advanced medical students explain diagnoses and medical terms previously submitted by patients.
The third dimension has also already been proposed theoretically by Zimmer et al. (2007). It focuses on variations in accessibility, in terms of the (perceived) difficulties one has to manage before being able to find and use the needed information, either prior to the information searching process or during the process itself. For example, to get information from a physician, several hurdles must be overcome: finding an appropriate physician for the respective health issue, making an appointment, waiting for the appointment, getting to the doctor's office, etc. These barriers all occur prior to the information gathering process. Furthermore, using sources may also be challenging, regarding aspects like usability of websites, or vocabulary used. Finding the suitable health information in the wide arrays of the internet or understanding the complex language of medical textbooks can be a considerable obstacle (Arora et al., 2008; see Diviani et al., 2015, for a review). In contrast, asking your mother is relatively easy. This subjective dimension is therefore useful for the distinction of health information sources regarding their “practicability” in daily life and the requirements needed to use the source appropriately. The usefulness of this dimension may be illustrated by the prominent “Dr Google” (Lee et al., 2014) issue describing individuals primarily relying on search engine results when it comes to symptoms and health problems. We now may test the hypothesis that people prefer to “consult” Google first: it's easy to use and highly accessible. Therefore, it is fundamental to provide individuals who score high on this third dimension with easily accessible, clear and comprehensible information.
Not only every single dimension, when regarded separately, provides an independent and significant contribution, but the combination of all three also offers fundamental explanatory content. The combination allows to create specific profiles for various relevant situations or groups of persons. This enables a deeper understanding of the arising information need and potential interactions between persons and situations. On an individual level, combining the three dimensions into information seeking preference profiles would help to offer strategies to provide information to address individual needs. Or in other cases, to uncover the manifold reasons of dissatisfaction with provided information and an unwillingness to seek any information at all (Case et al., 2005; Sweeny et al., 2010; Barbour et al., 2012). This approach would be in accordance with UAGT (Katz et al., 1973-1974) which highlights individual needs and preferences when it comes to choosing specific information sources.
To sum up, by identifying individuals' preferences on the three dimensions of the new taxonomy, their fundamental reasons to use particular information sources may be uncovered. Thereby, it is not only possible to research information preferences on a more general basis. Information can also be provided in accordance with individual needs, while at the same time fostering persons' adaptive information behavior.
Limitations
Several limitations have to be considered when interpreting the results of our studies. First, one might question whether the three-dimensional MDS solution is able to map the vast amount of available health information sources sufficiently precisely. As MDS results are heavily dependent on the selection of the objects to be classified, we cannot rule out that additional dimensions exist which we were not able to reveal because important information sources were omitted or specific source types were overrepresented in the pool of comparison objects. To minimize these problems, we took great care to compile a list of health information sources which is comprehensive but also non-redundant; the latter was achieved by categorizing single sources into overarching groups. The downside of presenting source categories instead of single sources is that potential within-category dissimilarities between sources cannot be revealed by the MDS procedure. However, reducing the pool of comparison objects was essential to keep the number of comparison objects reasonable for our participants. We assume that our categories which are based on expert consensus reflect the spectrum of the most important sources, enabling us to identify the central dimensions on which participants' similarity judgements are based.
Relatedly, one might argue that there are individual differences in the conceptualization of source categories, i.e., that individuals have a different understanding of the specific content of categories. We reduced this problem by supplementing each source type with examples to illustrate what is meant by the respective source label. This does not rule out the possibility of individual differences which result from weighting the examples or interpreting them selectively. However, our sample size seems large enough to compensate for potential individual differences in the interpretation of the source categories.
Finally, one may argue that the interpretation of an MDS solution is always subject to context-specific considerations (Borg and Staufenbiel, 2007), and, thus, labeling the dimensions is somewhat arbitrary: The expertise dimension, for example, might have been labeled “quality” or “trust.” However, we chose labels that were as fundamental as possible and would, due to their very basic meaning, supposedly achieve the highest agreement between individuals independently labeling the dimensions. In this sense, “trustworthiness” (e.g., Gray et al., 2005) and “quality” (e.g., Zhang, 2014) are not as fundamental as expertise; rather, trust and quality might be considered mere consequences of the basic property of the sources, the amount of professional medical knowledge the provided information bears upon. The same principle holds true for the other two dimensions (e.g., “user friendliness” may be the consequence of accessibility, and “emotional support” may be the consequence of personal interaction, but not the other way round). Nonetheless, to further validate our dimensions, future studies might apply an approach by Robinson and Bennett (1995). In their study, participants were not only asked to rate objects regarding their perceived similarity, but also to state the criteria they used to distinguish between the objects of comparison. Independent judges could then rate the fit of these criteria with regard to the research objects (information sources, in our case). Subsequent regression analyses determine the extent of the judged interrelation between the dimension labels and the distinguishing criteria.
Conclusions
In this article, we presented a multidimensional taxonomy for the classification of health information sources, which is based on subjective source perceptions, and thereby, is in line with the basic assumptions of UAGT (Katz et al., 1973-1974). With this, for the first time, basic dimensions of health information sources have been empirically assessed based on information users' perceptions of similarities and dissimilarities between sources. We thereby fruitfully complement research by Ruppel and Rains (2012), for example, who take into account individual reasons for using particular sources based on characteristics that are theoretically derived. The basic dimensions we identified partly correspond to dimensions that have been proposed before (e.g., Lu and Yuan, 2010). Thus, one major insight of this paper is that the subjective view of the differences between health information sources, are mostly in line with already established phenomenological classifications. However, in our opinion, it is an intriguing finding that by indirectly asking individuals to structure health information sources (namely, via similarity ratings), dimensions emerge that are similar to those that have already been proposed by other researchers. Researchers may use this taxonomy, particularly the underlying continuous dimensions of health information sources, to interpret their results with regard to individual reasons for the use of health information sources. Furthermore, already established ongoing surveys like the Health Information National Trends Survey (HINTS) and the Annenberg National Health Communication Survey (ANHCS), which used standard sets of health information sources beforehand, may adapt the taxonomy and include questions concerning source preferences based on individually perceived source dimensions in particular health specific situations. With this, combined knowledge about preferred sources and source properties would enable researchers to identify individual reasons for the use of health information sources.
Future research should address potential relationships between source preferences and individual factors. To fully understand why individuals choose inappropriate or biased sources, and to find out how preferences for different sources and information types in diverse situations can be explained, a sophisticated approach is needed. Above, we exemplarily described some situations in which persons might prefer specific source features over others. When experiencing symptoms associated with a sexually transmitted disease, for example, one might at first prefer information sources where no interpersonal contact is necessary. However, these assumptions were not yet empirically tested. Future studies should aim at providing evidence concerning these practical implications.
Another promising research approach would be to predict the use of a particular source by explicitly asking participants to classify the source with regard to the three dimensions and the perceived utility of the dimensions in a certain situation. In so doing, one would gain a deeper understanding of the underlying reasons why health information seeking behavior varies between persons and health contexts. Independent from context, some individuals might perceive high accessibility as most useful, whereas others might deem source expertise or the possibility of personal interaction as more important (depending on personal characteristics; e.g., Sun and Zhang, 2016). However, in certain contexts, such differences might disappear. For example, there is a significant time pressure in the case of an epileptic seizure, which is why accessibility of health information might be perceived most useful by almost everyone in this situation. Thus, to investigate person*situation-interactions, personality and contextual factors should be taken into account simultaneously. By this means, we aim to establish a psychological framework, which takes UAGT (Katz et al., 1973-1974) as a basis and aims at explaining and predicting individual preferences for specific health information sources according to individual needs, skills and motivation. We expect such a framework to have considerable value in a research area that has started to thrive only recently, and expect our taxonomy to be a fruitful starting point for such efforts.
Data Availability Statement
Datasets are available on request. The raw data supporting the conclusions of this manuscript will be made available by the authors, without undue reservation, to any qualified researcher.
Author Contributions
OW, AC, and A-KM conceived of the initial idea, planned and carried out the studies. OW and AC performed the analytic calculations, interpreted the results, and wrote the manuscript in consultation with A-KM and TR, who also contributed to the final manuscript. A-KM supervised the project.
Conflict of Interest Statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
References
American Psychological Association (2002): ethical principles of psychologists and code of conduct. Am. Psychol. 57, 1060–1073. doi: 10.1037//0003-066X.57.12.1060.
Arora, N. K., Hesse, B. W., Rimer, B. K., Viswanath, K., Clayman, M. L., and Croyle, R. T. (2008). Frustrated and confused: the American public rates its cancer-related information-seeking experiences. J. Gen. Intern. Med. 23, 223–228. doi: 10.1007/s11606-007-0406-y
Barbour, J. B., Rintamaki, L. S., Ramsey, J. A., and Brashers, D. E. (2012). Avoiding health information. J. Health Commun. 17, 212–229. doi: 10.1080/10810730.2011.585691
Blanch-Hartigan, D., and Viswanath, K. (2015). Socioeconomic and sociodemographic predictors of cancer-related information sources used by cancer survivors. J. Health Commun. 2, 204–210. doi: 10.1080/10810730.2014.921742
Borg, I., and Groenen, P. J. (2005). Modern Multidimensional Scaling: Theory and Applications. New York, NY: Springer.
Borg, I., and Staufenbiel, T. (2007). Theorien und Methoden der Skalierung [Theory and Method of Scaling]. Bern: Huber.
Case, D. O., Andrews, J. E., Johnson, J. D., and Allard, S. L. (2005). Avoiding versus seeking: the relationship of information seeking to avoidance, blunting, coping, dissonance, and related concepts. J. Med. Library Assoc. 93, 353–362.
Cattell, R. B. (1986). “The meaning and strategic use of factor analysis,” in Handbook of Multivariate Experimental Psychology, 2nd Edn, eds R. B. Cattell and J. R. Nesselroade (New York, NY: Plenum), 131–203.
DFG (2018). DFG- Deutsche Forschungsgemeinschaft - FAQ: Informationen aus den Geistes- und Sozialwissenschaften. [online] Available online at: http://www.dfg.de/foerderung/faq/geistes_sozialwissenschaften/index.html (Accessed August 27, 2018).
Diviani, N., van den Putte, B., Giani, S., and van Weert, J. C. (2015). Low health literacy and evaluation of online health information: a systematic review of the literature. J. Med. Internet Res. 17:e112. doi: 10.2196/jmir.4018
Dobransky, K., and Hargittai, E. (2012). Inquiring minds acquiring wellness: uses of online and offline sources for health information. Health Commun. 27, 331–343. doi: 10.1080/10410236.2011.585451
Dutta-Bergman, M. J. (2004). Primary sources of health information: comparisons in the domain of health attitudes, health cognitions, and health behaviors. Health Commun. 16, 273–288. doi: 10.1207/S15327027HC1603_1
Gray, N. J., Klein, J. D., Cantrill, J. A., and Noyce, P. R. (2002). Adolescent girls' use of the Internet for health information: issues beyond access. J. Med. Syst. 26, 545–553. doi: 10.1023/A:1020296710179
Gray, N. J., Klein, J. D., Noyce, P. R., Sesselberg, T. S., and Cantrill, J. A. (2005). Health information-seeking behaviour in adolescence: the place of the internet. Soc. Sci. Med. 60, 1467–1478. doi: 10.1016/j.socscimed.2004.08.010
Griffin, R. J., Dunwoody, S., and Neuwirth, K. (1999). Proposed model of the relationship of risk information seeking and processing to the development of preventive behaviors. Environ. Res. 80, 230–245. doi: 10.1006/enrs.1998.3940
Hall, A. K., Bernhardt, J. M., and Dodd, V. (2015). Older adults' use of online and offline sources of health information and constructs of reliance and self-efficacy for medical decision making. J. Health Commun. 7, 751–758. doi: 10.1080/10810730.2015.1018603
Hartzler, A., and Pratt, W. (2011). Managing the personal side of health: how patient expertise differs from the expertise of clinicians. J. Med. Internet Res. 13:e62. doi: 10.2196/jmir.1728
Johnson, J. D., and Meischke, H. (1993). A comprehensive model of cancer-related information seeking applied to magazines. Hum. Commun. Res. 19, 343–367. doi: 10.1111/j.1468-2958.1993.tb00305.x
Katz, E., Blumler, J. G., and Gurevitch, M (1973-1974). Uses gratifications research. Pub. Opin. Q. 37, 509–523. doi: 10.1086/268109
Kruskal, J. B. (1964). Multidimensional scaling by optimizing goodness of fit to a nonmetric hypothesis. Psychometrika 29, 1–27. doi: 10.1007/BF02289565
Lariscy, R. W., Reber, B. H., and Paek, H. J. (2010). Examination of media channels and type as health information sources for adolescents: comparisons for black/white, male/female, urban/rural. J. Broadcast. Electron. Media, 54, 102–120. doi: 10.1080/08838150903550444
Lawson, R., Forbes, S., and Williams, J. (2011). Patterns of trust in sources of health information. N. Z. Med. J. 124, 98–105. Available online at: http://www.nzma.org.nz/journal/read-the-journal/all-issues/2010-2019/2011/vol-124-no-1328/article-lawson
Lee, K., Hoti, K., Hughes, J. D., and Emmerton, L. (2014). Dr Google and the consumer: a qualitative study exploring the navigational needs and online health information-seeking behaviors of consumers with chronic health conditions. J. Med. Internet Res. 16:e262. doi: 10.2196/jmir.3706
Longo, D. R., Schubert, S. L., Wright, B. A., LeMaster, J., Williams, C. D., and Clore, J. N. (2010). Health information seeking, receipt, and use in diabetes self-management. Ann. Family Med. 8, 334–340. doi: 10.1370/afm.1115
Lu, L., and Yuan, Y. C. (2010). Shall I Google it or ask the competent villain down the hall? The moderating role of information need in information source selection. J. Assoc. Inform. Sci. Technol. 62, 133–145. doi: 10.1002/asi.21449
Magee, J. C., Bigelow, L., DeHaan, S., and Mustanski, B. S. (2012). Sexual health information seeking online: a mixed-methods study among lesbian, gay, bisexual, and transgender young people. Health Educ. Behav. 39, 276–289. doi: 10.1177/1090198111401384
Marrie, R. A., Salter, A. R., Tyry, T., Fox, R., and Cutter, G. (2013). Preferred sources of health information in persons with multiple sclerosis: degree of trust and information sought. J. Med. Internet Res. 15, 1–12. doi: 10.2196/jmir.2466
Morrison, E. W., and Vancouver, J. B. (2000). Within-person analysis of information seeking: the effects of perceived costs and benefits. J. Manage. 26, 119–137. doi: 10.1177/014920630002600101
Pecchioni, L. L., and Sparks, L. (2007). Health information sources of individuals with cancer and their family members. Health Commun. 21, 143–151. doi: 10.1080/10410230701307162
Powell, J., Inglis, N., Ronnie, J., and Large, S. (2011). The characteristics and motivations of online health information seekers: cross-sectional survey and qualitative interview study. J. Med. Internet Res. 13:e20. doi: 10.2196/jmir.1600
Rains, S. A. (2007). Perceptions of traditional information sources and use of the world wide web to seek health information: findings from the health information national trends survey. J. Health Commun. 12, 667–680. doi: 10.1080/10810730701619992
Redmond, N., Baer, H. J., Clark, C. R., Lipsitz, S., and Hicks, L. S. (2010). Sources of health information related to preventive health behaviors in a national study. Am. J. Prev. Med. 38, 620–627. doi: 10.1016/j.amepre.2010.03.001
Robinson, S. L., and Bennett, R. J. (1995). A typology of deviant workplace behaviors: a multidimensional scaling study. Acad. Manage. J. 38, 555–572.
Ruppel, E. K., and Rains, S. A. (2012). Information sources and the health information seeking process: an application and extension of channel complementarity theory. Commun. Monograp. 79, 385–405. doi: 10.1080/03637751.2012.697627
Rutten, L. J., Arora, N. K., Bakos, A. D., Aziz, N., and Rowland, J. (2005). Information needs and sources of information among cancer patients: a systematic review of research (1980-2003). Patient Educ. Couns. 57, 250–261. doi: 10.1016/j.pec.2004.06.006
Smith, D. (2011). Health care consumer's use and trust of health information sources. J. Commun. Healthc. 4, 200–210. doi: 10.1179/1753807611Y.0000000010
Sun, Y., and Zhang, Y. (2016). “Individual differences and online health information source selection” in Proceedings of the 2016 ACM on Conference on Human Information Interaction and Retrieval. (Chapel Hill, NC: ACM), 321–324.
Sweeny, K., Melnyk, D., Miller, W., and Shepperd, J. A. (2010). Information avoidance: Who, what, when, and why. Rev. Gen. Psychol. 14, 340–353. doi: 10.1037/a0021288
Torgerson, W. S. (1952). Multidimensional scaling: I. Theory and method. Psychometrika 17, 401–419. doi: 10.1007/BF02288916
Tustin, N. (2010). The role of patient satisfaction in online health information seeking. J. Health Commun. 15, 3–17. doi: 10.1080/10810730903465491
Young, F. W., Takane, Y., and Lewyckyj, R. (1978). ALSCAL: a nonmetric multidimensional scaling program with several individual differences-options. Behav. Res. Methods Instrument. 10, 451–453. doi: 10.3758/BF03205177
Zhang, Y. (2014). Beyond quality and accessibility: source selection in consumer health information searching. J. Assoc. Inform. Sci. Technol. 65, 911–927. doi: 10.1002/asi.23023
Keywords: health information, health communication, information sources, uses and gratifications theory, multidimensional scaling
Citation: Wedderhoff O, Chasiotis A, Rosman T and Mayer A-K (2018) Unveiling the Subjective Perception of Health Information Sources: A Three-Dimensional Source Taxonomy Based on Similarity Judgements. Front. Commun. 3:57. doi: 10.3389/fcomm.2018.00057
Received: 10 September 2018; Accepted: 03 December 2018;
Published: 13 December 2018.
Edited by:
Rukhsana Ahmed, University at Albany, United StatesReviewed by:
Peter Johannes Schulz, University of Lugano, SwitzerlandKyong Eun Oh, Simmons College, United States
Copyright © 2018 Wedderhoff, Chasiotis, Rosman and Mayer. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Oliver Wedderhoff, ow@leibniz-psychology.org
Anita Chasiotis, ac@leibniz-psychology.org