 Gemma Mestre-Bach1,2
Gemma Mestre-Bach1,2 Trevor Steward1,2
Trevor Steward1,2 Roser Granero2,3
Roser Granero2,3 Fernando Fernández-Aranda1,2,4
Fernando Fernández-Aranda1,2,4 María Teresa Talón-Navarro5
María Teresa Talón-Navarro5 Àngel Cuquerella5
Àngel Cuquerella5 Marta Baño1
Marta Baño1 Laura Moragas1
Laura Moragas1 Amparo del Pino-Gutiérrez6
Amparo del Pino-Gutiérrez6 Neus Aymamí1
Neus Aymamí1 Mónica Gómez-Peña1
Mónica Gómez-Peña1 Núria Mallorquí-Bagué1,2Cristina Vintró-Alcaraz1,2Pablo Magaña7
Núria Mallorquí-Bagué1,2Cristina Vintró-Alcaraz1,2Pablo Magaña7 José Manuel Menchón1,4,8
José Manuel Menchón1,4,8 Susana Jiménez-Murcia1,2,4*
Susana Jiménez-Murcia1,2,4*
- 1Pathological Gambling Unit, Department of Psychiatry, Institut d’Investigació Biomédica de Bellvitge (IDIBELL), Bellvitge University Hospital, Barcelona, Spain
- 2Ciber Fisiopatología Obesidad y Nutrición (CIBERObn), Instituto de Salud Carlos III, Madrid, Spain
- 3Department de Psicobiologia i Metodologia, Autonomous University of Barcelona, Barcelona, Spain
- 4Department of Clinical Sciences, Faculty of Medicine, University of Barcelona, Barcelona, Spain
- 5Institute of Legal Medicine and Forensic Sciences of Catalonia, Barcelona, Spain
- 6Nursing Department of Mental Health, Public Health, Maternal and Child Health, Nursing School, University of Barcelona, Barcelona, Spain
- 7Department of Law, Pompeu Fabra University, Barcelona, Spain
- 8Ciber de Salud Mental (CIBERSAM), Instituto de Salud Carlos III, Madrid, Spain
Gambling disorder (GD) is a psychiatric condition that was recently recategorized as a non-substance-related addiction in the Diagnostic and Statistical Manual of Mental Health Disorders. Criminal activity is commonly associated with gambling; however, few empirical studies to date have examined sociodemographic and psychological variables in this population. In this study, we explored criminal behavior history in a sample of consecutively recruited treatment-seeking gamblers (n = 382) and compared subjects with a history of illegal acts (n = 103, 26.9%) to those with no criminal record (n = 279, 73.1%). Impulsivity and personality traits were specifically explored, along with other gambling-related severity factors. We found that gamblers who engaged in illegal activity were more likely to endorse high levels of urgency (i.e., the tendency to act out when experiencing heightened emotional states) and increased lack of premeditation. Gamblers with a history of criminal behavior also had greater GD severity levels and gambling-related debts. Additionally, these gamblers reported lower levels of self-directedness, which is characterized by difficulty in establishing and redirecting behavior toward one’s goals. Likewise, gamblers who had conducted criminal acts showed a tendency to engage in greater risk-taking behavior. These results shed new light on this understudied population and provide insights for developing targeted harm-prevention interventions and treatment protocols.
Introduction
Gambling Disorder (GD) Conceptualization
Gambling disorder is characterized by a maladaptive pattern of gambling behavior that persists despite negative consequences in major areas of life functioning. It was recently recategorized as a non-substance-related addiction in the Diagnostic and Statistical Manual of Mental Health Disorders (DSM-5) (1). This disorder more frequently occurs in men (2) and is often characterized by specific personality traits, high impulsivity levels, and cognitive distortions, such as illusion of control (3–5).
One of the DSM-IV-TR diagnostic criteria for pathological gambling (6) included carrying out criminal acts in order to support gambling behavior. However, after much debate, the scientific community considered that this criterion provided little accuracy, leading to the removal of the “illegal acts” criterion from DSM-5 (1). Many researchers in the field of criminology believe that committing criminal offenses in order to finance gambling behavior should be considered as an indicator of disorder severity, instead of as an independent diagnostic criterion (7, 8). Moreover, it has been argued that GD-related criminal acts seldom occur in the absence of other GD criteria (9). However, the clinical and societal importance of this criterion has been subject to considerable discussion (10). After a classification and regression tree analysis, Themcheff et al. (11) highlighted that the “illegal acts” criterion showed high discriminative capacity between social and problem gamblers, and suggested that policy makers take this information into account. Nonetheless, this framework requires additional empirical support before informed decisions can be made.
Criminal Behavior Related to GD
The self-reported prevalence of criminal behaviors in individuals diagnosed with GD ranges from 14 to 30% (8, 12). This relatively high mismatch between results could be explained bearing in mind that crime and GD are related in a complex and multifactorial way, including high comorbidity with other disorders, the presence of associated risk behaviors, sociodemographic factors, and gambling-related circumstances (e.g., financial debts) (12–14). In an attempt to coalesce a functional theoretical framework, most of the existing body of research on this topic has focused on two main associations between these factors (15). On one hand, gambling behaviors could be part of a criminal lifestyle, related to antisocial personality disorder (16); on the other, criminal activity could be precipitated by GD, especially when money becomes scarce (13). Data suggest that the latter is more habitual, since individuals with GD usually do not have a criminal record or a history of norms transgression prior to developing gambling problems (17).
When considered within the framework of the general strain theory, gamblers who face negative events or emotions, such as extreme financial difficulties, might be more prone to turn to illegal activity to support their habit (18, 19). Likewise, these difficulties could also subsequently increase the probability of carrying out illegal acts in order to try to relieve financial hardships (20). GD-related crimes are frequently reported as being committed in desperation in order to amend financial predicaments brought about by gambling-related losses, or, in some cases, to fund additional gambling episodes (21).
Nevertheless, not all individuals with GD and financial burdens engage in criminal behavior. Several attempts have been made to explain the risk factors associated with GD-related crime in greater depth. For example, substance abuse has been found to be prevalent in patients with GD (14, 22). This frequent comorbidity adds another complex factor as to why gamblers may commit crimes, although no longitudinal studies to date have established a causal relationship between substance abuse and gambling-related criminal acts. Results from another study suggested that stimulant substance abuse may potentially facilitate gambling-related illegal acts due to their disinhibitory effects (12). Similarly, GD severity positively correlates, in most cases, with the occurrence of criminal behaviors (23). Therefore, engagement in criminal acts to support one’s gambling behavior is, in all likelihood reflective of GD severity reaching its nadir (8, 12, 21, 24, 25). During early stages of the disorder, crime is commonly reported to be carried out with remorse, and gamblers often claim that they have the intention of returning fraudulently obtained goods when their debts, derived from gambling behavior, have been settled. This logic for justifying criminal behavior greatly differs from others who commit crimes such as petty theft or fraud (26). However, when GD is consolidated and debts are increased, an individual with GD has more difficulties regulating their behavior according to their basic moral principles and signs of repentance are blurred (21, 27).
In addition to GD comorbidity and other clinical factors, sociodemographic and personality features are also associated with crime (12). One study identified different subtypes of GD patients who committed crimes, taking sociodemographic variables, personality traits and clinical information related to GD into account (28). Psychopathology levels and poor impulse control were some of the main characteristics that best distinguished GD groups with a criminal record. Although some findings in the criminology literature have suggested that GD patients present different typologies of criminal behavior, obtaining money to finance gambling behavior is usually the primary motive for these crimes (29). Specifically, the most common criminal offenses in this population are petty theft, theft, fraud and forgery (30). GD patients do not usually show a propensity for violent behavior; however, financially motivated violent crimes do occasionally occur in this population (31).
Assuming the “generality of deviance” perspective (32), which suggests that varied forms of risk-taking behaviors tend to cooccur among individuals, the spectrum of deviant and criminal behaviors appears to have a common denominator: the tendency to seek immediate reward or relief without concern for long-term negative consequences (33). Therefore, the authors suggest that self-control is a main factor in determining the likelihood of engaging in criminal acts (34). These behavioral patterns, such as personality traits associated with risk (sensation seeking, impulsivity and low self-control) and multiple domains of risky attitudes, are also common in patients with GD (35–37). The authors highlight the existence of a key wedge factor of common variance “the generality of deviance” in gamblers, suggesting that shared personality traits, such as greater risk taking, may be a driver of deviant behavior (38). In this vein, Mishra et al. (39) suggested that GD was strongly associated with progambling and risk-taking attitudes.
Impulsivity is increasingly understood to be an early risk factor for the development of both GD (40) and delinquency (41). Impulsivity is a multidimensional construct encompassing facets such as the dysregulation of outward behavior due to decreased inhibitory control or a prejudicial decision-making style (e.g., choosing immediate gratification over larger, delayed rewards) (35). In recent years, the UPPS-P framework of impulsivity has become one of the most utilized models of impulsivity in psychiatric research. This questionnaire divides impulsivity levels into five subscales: lack of premeditation, lack of perseverance, positive and negative urgency, and sensation seeking (42). Specifically, urgency, defined as emotionally charged impulsive behaviors in response to positive or negative moods, has been found to be crucial in distinguishing between clinically dysfunctional GD patients and recreational gamblers (43).
During adolescence (the age at which most individuals begin to gamble) (44), cognitive impulsivity has also been found to be associated with a more rapid acceleration into criminal behavior (41). Likewise, urgency and lack of premeditation are known to significantly correlate with each other in adolescents (45). Researchers have also observed that an impulsive decision-making style and high levels of urgency are associated with an increased acceptance of erroneous beliefs (e.g., believing that a series of losses must be followed by a win) during gambling behavior, thereby worsening economic consequences (46, 47). Given that gamblers encompass a very heterogeneous group of patients, one might postulate that gambling-related illegal acts could be more commonplace in younger, impulsive gamblers than in older gamblers whose gambling motivations might be driven by altered emotion regulation capacity (29, 35). To our knowledge, however, no studies to date have examined the role that impulsivity plays in criminal behavior within the context of gambling.
GD, Criminal Behavior, and the Spanish Court System
Within Spanish civil law/civil code, legal mechanisms exist which aim to limit the capacity of an individual with GD to inflict financial damage onto themselves or others. Namely, revoking legal guardianship or declaring civil incapacity allows for capital losses resulting from GD to be protected (48). Similarly, GD patients have the option to voluntarily bar themselves access to gambling establishments, either online or land-based, as part of a state-sponsored harm reduction program. Enrollment in the program can be indefinite; although participants may opt out of it at any time.
The Spanish Criminal Code does not specifically mention gambling as a mitigating or extenuating circumstance capable of reducing the gravity of an offense with regards to sentencing or moral opprobrium. However, in practice, the Spanish court system tends to apply discretion by imposing minimum penalties in cases characterized by reduced freewill that exhibit a clear causal relationship between the committed crime and gambling addiction (17).
Aims and Hypothesis
The primary aim of this study was to compare impulsivity traits in a sample of treatment-seeking GD patients who committed illegal acts to those who did not. Furthermore, we aimed to explore differences between these groups in terms of sociodemographic and psychological variables, and the type of illegal act committed in order to ascertain which variable(s) best predicted the presence of a history of criminal behavior.
As stated above, high levels of debt and significant financial problems because of gambling behavior is often indicated a primary motive for committing a crime (21); therefore, we hypothesized that the GD patients with a history of criminal behavior would present higher levels of debt than those without a criminal record. We also hypothesized that GD patients with a history of criminal behavior would be characterized by greater levels of GD severity, impulsivity, and overall psychopathology (8, 12). Likewise, we hypothesized that those gamblers with a history of committing multiple offenses would present increased psychopathology, GD severity and levels of accumulated debt (49).
Materials and Methods
Participants and Procedure
The sample consisted of 382 patients with a diagnosis of GD who were being treated at the Gambling Disorder Unit within the Department of Psychiatry at Bellvitge University Hospital (Barcelona, Spain). This public hospital is certified as a tertiary care center for the treatment of addictive behaviors and oversees the treatment of very complex cases. Patients were derived to the Bellvitge University Hospital Gambling Disorder Unit through general practitioners or via another healthcare professional; some patients were derived from prison health services, though their treatment was not compulsory in the majority of cases. Nonetheless, in a few cases, a judge may have dictated the need for specific GD treatment at our unit. All treatment services for GD within the public Spanish healthcare system are provided free of charge.
Sociodemographic, clinical and criminal additional information was taken, and patients individually completed all the questionnaires required for this study (requiring approximately 2 h) before initiating outpatient treatment. Only patients who sought treatment for GD as their primary mental health concern and who met DSM-5 criteria for GD (1) were included in our sample. Exclusion criteria were: the presence of an organic mental disorder, intellectual disability, a neurodegenerative condition, such as Parkinson’s disease, or an active psychotic disorder. Participants were classified in two groups according the presence (n = 279) or absence (n = 103) of criminal behaviors related to GD. Criminal behavior was assessed via a structured interview with a staff clinical psychologist.
The present study was carried out in accordance with the latest version of the Declaration of Helsinki. The University Hospital of Bellvitge Ethics Committee of Clinical Research approved the study, and written informed consent was obtained from all participants.
Measures
GD Severity
DSM-5 Criteria (1)
Patients were diagnosed with pathological gambling if they met DSM-IV-TR criteria (6). It should be noted that with the release of the DSM-5 (1), the term pathological gambling was replaced with GD. All patient diagnoses were reassessed and recodified post hoc and only patients who met DSM-5 criteria for GD were included in our analysis.
South Oaks Gambling Screen (SOGS) (50)
This self-report 20-item screening questionnaire discriminates between probable pathological, problem and non-problem gamblers. The Spanish validation used in this work showed excellent internal consistency (α = 0.94) and test–retest reliability (r = 0.98) (51).
Impulsivity Traits
Impulsive Behavior Scale (UPPS-P) (52)
The UPPS-P measures five facets of impulsive behavior through self-report on 59 items: negative urgency; positive urgency; lack of premeditation; lack of perseverance; and sensation seeking. Individuals are asked to consider acts/incidents during the last 6 months when rating their behavior and attitudes. The Spanish-language adaptation shows good reliability (Cronbach’s α between 0.79 and 0.93) and external validity (53).
Psychopathology
Symptom Checklist-Revised (SCL-90-R) (54)
This is a 90-item questionnaire measuring psychological distress and psychopathology. The items assess nine symptom dimensions: somatization, obsessive-compulsive, interpersonal sensitivity, depression, anxiety, hostility, phobic anxiety, paranoid ideation, and psychoticism. The global score [Global Severity Index (GSI)] is a widely used index of psychopathological distress and was the only variable from this questionnaire used in this study. The Spanish adapted version was used in this study (55).
Personality
Temperament and Character Inventory-Revised (TCI-R) (56)
The TCI-R is a reliable and valid 240-item questionnaire measured on a 5-point Likert-type scale to evaluate personality traits. It is structured using seven primary personality dimensions: four temperamental factors (novelty seeking, harm avoidance, reward dependence, and persistence) and three character dimensions (self-directedness, cooperativeness, and self transcendence). The Spanish revised version used in this study (57) showed adequate internal consistency (Cronbach’s alpha a mean value of 0.87).
Alcohol and Other Drugs use-abuse
Alcohol Use Disorders Identification Test (AUDIT) (58)
This test was developed as a simple screening method for excessive alcohol consumption. Internal consistency has been found to be high, and test–retest data have suggested a high reliability (0.86) and a sensitivity of around 0.90. Specificity in different settings and for different criteria averages 0.80 or more (59). In this work, cutoff points of 8 and 20 were used to identify individuals with alcohol abuse and alcohol dependence, respectively (60).
Drug Use Disorders Identification Test (DUDIT) (61)
The DUDIT is an 11-item screening instrument developed to identify non-alcohol drug use patterns and various drug-related problems in the general public, as well as in individuals in clinical settings who are likely to meet criteria for a substance dependence diagnosis (61). The first nine items are scored on a 5-point Likert scale ranging from 0 to 4, and the last two are scored on 3-point scales (values of 0, 2, 4). Total scores can range from 0 to 44, with higher scores being indicative of a more severe drug problem. The following risk levels have been suggested for DUDIT scores: no drug-related problems (total scores 0–5/1); possible drug-related problems, that is, risky or harmful drug habits that might be diagnosed as substance abuse/harmful use or dependence (6/2–24); likely heavily dependent on drugs (scores ≥ 25) (61).
Other Sociodemographic and Clinical Variables
Additional demographic, clinical, and social/family variables related to gambling were measured using a semi-structured face-to-face clinical interview described elsewhere (62). The gambling behavior variables covered included the age of onset of gambling behavior and of gambling-related problems, the average amount of money spent in a single gambling episode, the maximum amount ever bet in a single episode, and the total amount of accumulated gambling debts. In addition, the interview explored lifetime criminal activity related to GD in order to supplement the information obtained through the eighth DSM-IV-TR criterion (6). Crime-centered typologies were used to group subjects into three categories: those who conducted petty theft (the most frequent criminal behavior in our clinical population); those who committed other offenses (including counterfeiting or crimes against the public, among others); and those with multiple types of offenses.
Statistical Analyses
Statistical analyses were carried out with Stata 13.1. Comparison between groups was based on chi-square tests (χ2) for categorical variables, t-test procedures for two mean comparisons in independent groups, and analysis of variance for mean comparisons in three or more independent groups.
The predictive capacity of impulsivity (UPPS-P raw scores) for the presence of illegal acts was based on binary logistic regression (adjusted for the covariates age of onset, GD duration, cumulate debts from gambling and GD severity). Goodness of fit was assessed through Hosmer–Lemeshow test (p > 0.05 was considered adequate fitting), global predictive capacity through Nagelkerke’s pseudo-R2 coefficient and global discriminative capacity through the area under the ROC curve.
Increases in Type-I error due to multiple statistical comparisons was controlled through Finner’s correction, a procedure included in Familywise error rate stepwise procedures which offers more powerful results than Bonferroni correction (63). Effect size for comparisons between groups was estimated through Cohen’s-d coefficient (moderate effect size was considered for |d| > 0.50 and good for |d| > 0.80), and through the 95% confidence interval (95% CI) for the logistic regression.
Since this study was planned posterior to the data recruitment, the calculation of the required sample was not possible. However, a power calculation for statistical analysis based on two independent mean comparisons was carried out with the following parameters: total sample size equal to n = 382, bilateral contrasts and expected mean values for the groups equal to 50 and 55 (these means were selected based on T-standardized scores commonly employed in clinical research, whose distributions include the parameters: mean μ = 50 and SD σ = 10 in community samples). Estimated power resulted in 0.983 (risk β = 0.017, less than 2%). For the chi-square test which compares two independent proportions (set at 60 and 75%), the power estimated resulted in 0.870 (risk β = 0.130).
Results
Sample Description
The first section of Table 1 includes the sociodemographic characteristics of the sample stratified by the presence/absence of a history of illegal behavior. Most participants were born in Spain (95.3%), had finished primary school (57.6%), were single or separated/divorced (59.2%), were employed (55.5%) and were in a middle-low to low socioeconomic status level (51.3%) (Hollingshead, Unpublished manuscript)1. No statistically significant differences in sociodemographic characteristics between patient groups were found.
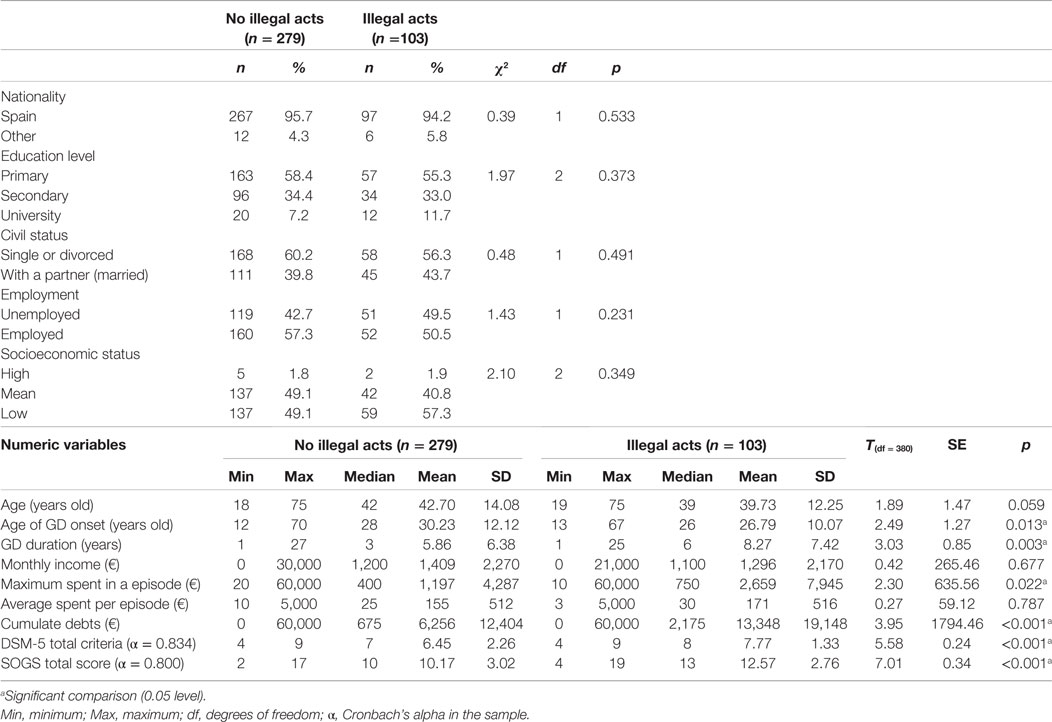
Table 1. Sample description.
The second section of Table 1 includes GD-related variables. No differences in chronological age, monthly income, and mean amount spent per gambling episode between groups were found. However, patients who reported engaging in illegal activities endorsed a younger age of gambling onset and longer duration of GD. Patients with a criminal record also had higher GD severity levels on the SOGS as well as greater gambling-related debts.
Comparison between Patients with and without a History of Criminal Behavior
Table 2 includes a comparison of impulsivity/personality traits, psychopathology, and substance use behaviors in patients who reported a history of engaging in illegal activity. Patients with a criminal history reported higher levels in positive and negative urgency, lack of premeditation and lack of perseverance compared to GD patients with no criminal record. GD patients who reported having committed gambling-related crimes also had higher levels of psychopathology (according to the SCL-90-R). In terms of personality traits, GD patients with a criminal record presented higher levels of novelty seeking and lower levels of self-directedness and cooperativeness compared to GD patients without a criminal record. No differences between groups were found with regards to substance use/abuse.
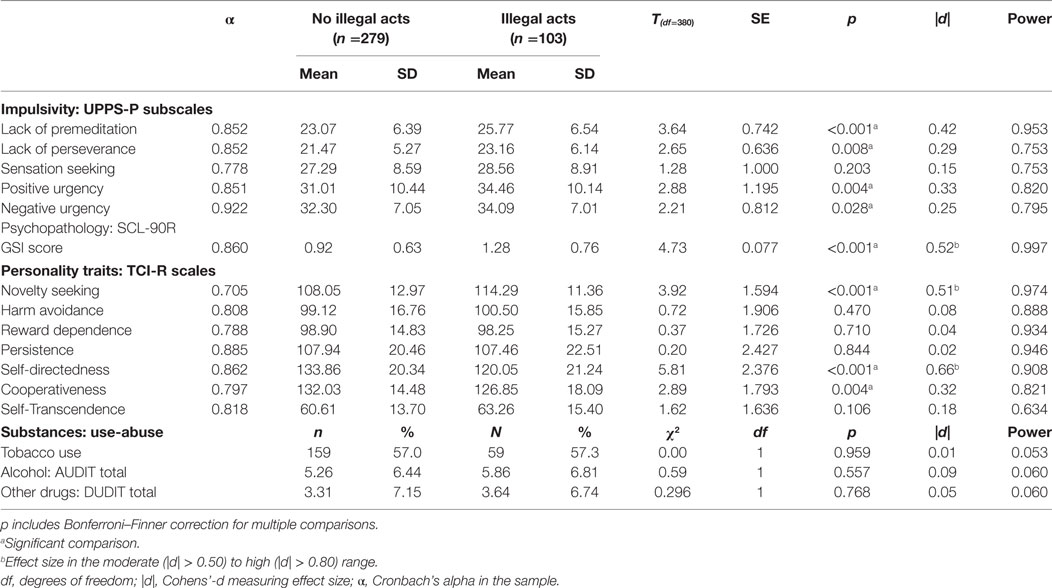
Table 2. Clinical comparison between patients with and without illegal acts.
Predictive Capacity of Impulsivity Levels on Criminal Behavior
The upper part of Table 3 includes the logistic regression measuring the predictive capacity of impulsivity levels (measured through the UPPS-P scales) on the presence of illegal acts in the entire sample. The model was carried out in two blocks/steps: the first block included and set the covariates age of onset and GD duration and second block added the five UPPS-P subscales. After adjusting for the covariates, the odds of having a history of criminal behavior was increased for patients with higher scores in the lack of premeditation and positive urgency impulsivity subscales. Goodness of fit was obtained (Hosmer–Lemeshow: p = 0.167), and the model showed moderate predictive capacity (the increase/change in the R2 coefficient comparing first and second block was ΔR2 = 0.12) and moderate discriminative capacity (AUC = 0.68).
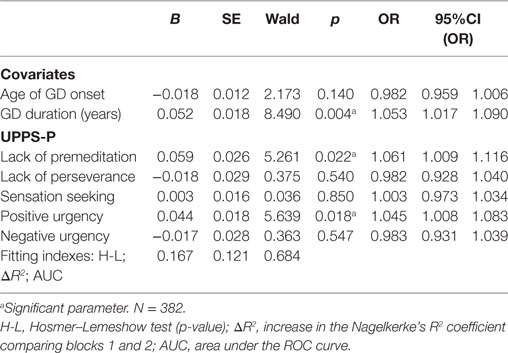
Table 3. Predictive capacity of impulsivity profile (UPPS-P scores) on the presence of illegal acts: logistic regression adjusted for age of gambling disorder onset and GD duration.
Table S1 in Supplementary Material contains a new predictive model including also two additional GD-related measures as covariates into the first block: cumulate debts and disorder severity (SOGS total score). In the resulting logistic predictive regression, UPPS-P positive urgency raw score remained a significant predictor.
Comparison Based on Type of Illegal Act
Table 4 contains a comparison between the n = 103 GD patients who reported a history of illegal activity based on the type of crime(s) committed (theft, other, or multiple). A number of patients (n = 25) chose not to specify which type of gambling-related illegal act they committed and these patients were excluded from this analysis. Patients who reported committing multiple types of illegal acts obtained the highest means in cumulate debts due to gambling, and higher GD severity levels according to the SOGS.
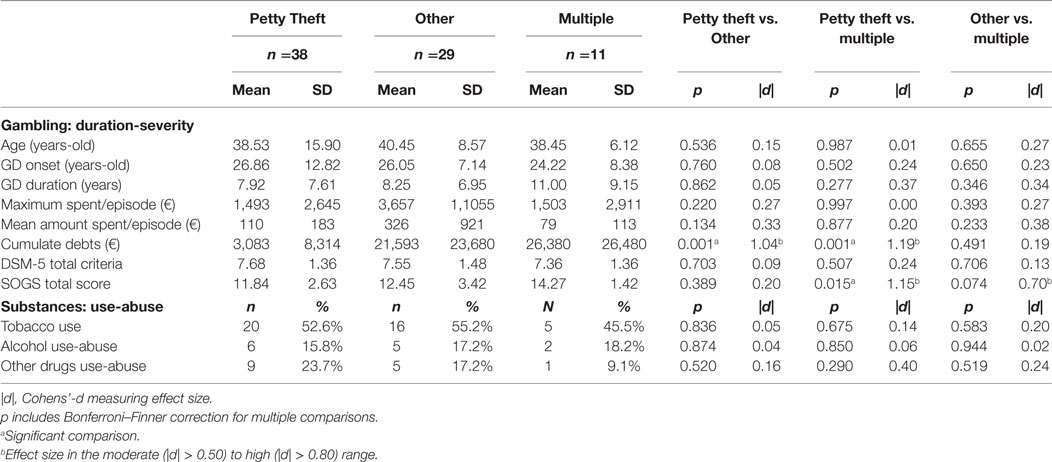
Table 4. Clinical comparison for patients based on type of illegal act committed.
Discussion
This study analyzed differences in impulsivity and personality traits between treatment-seeking GD patients who committed illegal acts and those who did not. Moreover, we sought to examine the interplay between criminal typology, sociodemographic features, and psychological variables.
Regarding the multidimensional nature of risk factors for engaging in crime, as suggested by previous studies, sociodemographic (especially gender and age) (64), education (65), and economic factors (such as socioeconomic status) (12) were determinants of the incidence of crime. In Western populations, the association between age and crime mainly follows a bell-shaped pattern, known as the age-of-crime curve, showing a reduction in criminal activity as an individual progress into adulthood (66, 67). Surprisingly, no differences were found between GD patients who committed crimes and those who did not, even though we hypothesized that the GD patients with a criminal record would be younger. It is worth noting, however, that our sample was made up patients voluntarily seeking treatment for GD and that we did not explore at what age these patients began engaging in illegal activity to finance their gambling behavior.
On the other hand, earlier studies have shown that education may counteract the risk of committing crimes, being that those with a higher level of education have higher expectations regarding the amount of income they can derived from legal ventures (65). Moreover, the inverse relationship between social stratification and delinquency turns out to be one of the main points of interest in criminology (68). However, contrary to expectations, this study did not find significant differences between groups in years of schooling. These results may partly be explained by the fact that our sample consisted of gamblers who sought treatment of their own volition and therefore our results are not necessarily representative of gamblers as a whole. Similar issues arise in the case of substance abuse as most individuals report first using drugs at a younger age and not seeking treatment until they are often much older (69). In this vein, an additional explanation could be that only crimes related to gambling behavior have been evaluated and those subjects whose main clinical problem was exclusively GD were included in the study.
Keeping with our hypothesis, patients who committed GD-related crimes reported greater GD severity, higher maximum bets and more cumulated debts in comparison with those who did not. This result dovetails with previous studies also reporting that GD patients with gambling-related crimes experienced more severe gambling symptoms than did other gamblers (15, 16, 21, 27). These findings suggest that greater gambling-related economic expenditures (more money spent during gambling episodes and more overall gambling-related debts) would increase an individual’s likelihood of resorting to illegal behaviors in order to obtain money rapidly and, consequently, to be able to continue addictive-like gambling behavior.
Another finding to emerge from the present study is the difference in age of onset of GD between both groups, showing earlier onset in the illegal acts group. In our study, the measure to determine “onset” referred to the moment when the patients identified that gambling behavior had become harmful and uncontrollable. In this vein, previous studies showed that several factors are associated with early GD onset, including higher trait impulsivity and substance use disorders (70, 71).
Relatedly, our stepwise analyses identified both positive urgency and lack of premeditation to be predictors of the presence of illegal activity in GD patients. Both of these impulsivity traits have been found to commonly be higher in younger individuals and could potentially be seen as a risk factor, though longitudinal are needed to support this claim (35, 72). With regards to personality traits, GD patients with a history of criminal behaviors also reported lower levels of self-directedness. Self-directedness is characterized by possessing an external locus of control and, therefore, encountering more difficulties in planning, decision-making and achieving goals (56). This finding is consistent with other studies highlighting low levels of self-directedness across psychiatric disorders (73–75). Contrary to our hypothesis, no differences were found in substance use/abuse prevalence between GD patients who did and did not report committing gambling-related crimes. This may be partly due to the fact that we only assessed current substance-use patterns in our sample and that all of our patients were voluntarily seeking treatment.
Although some demographic risk factors have been identified for criminal recidivism (in particular gender, age, and race), in recent years there has been much debate about whether sociodemographic factors in themselves can fully account for the complexity behind reoccurring criminal behaviors (76, 77). In our sample, GD patients who had committed multiple offenses endorsed greater GD severity levels and greater amounts of gambling-related debts. These results coincide with other studies supporting the existence of subgroups of gamblers that are distinguishable according to their gambling-related criminal behaviors (27).
Ethical Issues Raised by the Study
Our analysis seems to prompt at least two important moral issues. The first pertains to autonomy. If GD patients with a history of criminal behavior tend to report lower levels of self-directedness, it can be argued that their capacity for autonomous action is, in some sense, diminished. This is important because autonomy is tied to responsibility. The less autonomous an individual is, the less responsible we hold them for their actions. If GD patients who engaged in illegal acts tend to display lower levels of autonomy, we should take this fact into account when making attributions of responsibility. This overlaps with our previous discussion of the Spanish court system and its de facto concern for gambling-related instances of reduced free will. The second issue arises once we realize that both positive urgency and lack of premeditation are predictors of the presence of illegal activity in GD patients. Given the serious risk of adding stigmatization to this population, we should set a high bar in terms of predictive value before using such variables as proxy for policy-making. And if this becomes unavoidable, then efforts should be made to minimize the risk of stigmatization as much as possible. However, given the self-acknowledged limitations of this analysis, this should be considered (i.e., whether such predictors are robust enough for determining future policies) an open question.
Limitations
Our results must be interpreted in light of their limitations. The main weakness of this study was that exploring criminal behaviors through self-report in a clinical interview and not administering a validated psychometric instrument may have generated false negatives and limited the thoroughness of the obtained information. Second, our sample was made up exclusively of male GD patients, and taking into account that male gender is one of the indicators most associated with gambling-related crimes (12), the generalizability of the results to other populations is discouraged (78). Finally, the present study was focused exclusively on criminal behaviors carried out with the aim of financing debts derived from gambling or ensuring the continuity of gambling behavior. Future studies should consider the full scope of illegal behaviors carried out by GD patients, even those not directly related to gambling.
Conclusion
This study provides greater empirical understanding of the associations between GD, impulsivity, and criminal behavior. Our findings suggest that high levels of trait impulsivity, especially lack of premeditation and positive urgency, are predictors of the occurrence of crime in those who gamble. Further research should be undertaken to examine the effectiveness of interventions targeting impulse traits and recidivism risk management in gambling populations. Such detailed information would be useful in improving GD treatment and harm reduction interventions.
Author Contributions
GM-B, TS, FF-A, RG, JM, and SJ-M designed the experiment based on previous results and the clinical experience of M-TN, AC, MB, LM, AP-G, NA, MG-P, CV-A, and NM-B. RG, GM-B, TS, FF-A, and SJ-M conducted the experiment, analyzed the data, and wrote a first draft of the manuscript. SJ-M, TS, GM-B, RG, PM, and FF-A further modified the manuscript.
Conflict of Interest Statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Funding
This manuscript and research were supported by grants from Instituto de Salud Carlos III (ISCIII) (FIS PI14/00290) and cofounded by FEDER funds/European Regional Development Fund (ERDF), a way to build Europe. CIBER Fisiopatología de la Obesidad y Nutrición (CIBERobn) and CIBER Salud Mental (CIBERsam) are supported by ISCIII. This work was also supported by the Ministerio de Economía y Competitividad (PSI2015-68701-R). GM-B is supported by an AGAUR predoctoral grant (2017FI_B1 00145). CVA is supported by a predoctoral Grant from the Ministerio de Educación, Cultura y Deporte (FPU16/01453).
Supplementary Material
Supplementary Material for this article can be found online at http://www.frontiersin.org/articles/10.3389/fpsyt.2018.00006/full#supplementary-material.
Footnote
- ^Hollingshead, A. A. Four-factor index of social status. Unpublished manuscript, Yale University, New Haven, CT (1975).
References
1. American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders. 5th ed. Washington, DC: American Psychiatric Association (2013).
2. Granero R, Penelo E, Martínez-Giménez R, Álvarez-Moya E, Gómez-Peña M, Aymamí MN, et al. Sex differences among treatment-seeking adult pathologic gamblers. Compr Psychiatry (2009) 50:173–80. doi:10.1016/j.comppsych.2008.07.005
3. Mann K, Lemenager T, Zois E, Hoffmann S, Nakovics H, Beutel M, et al. Comorbidity, family history and personality traits in pathological gamblers compared with healthy controls. Eur Psychiatry (2017) 42:120–8. doi:10.1016/j.eurpsy.2016.12.002
4. Chamberlain SR, Stochl J, Redden SA, Odlaug BL, Grant JE. Latent class analysis of gambling subtypes and impulsive/compulsive associations: time to rethink diagnostic boundaries for gambling disorder? Addict Behav (2017) 72:79–85. doi:10.1016/j.addbeh.2017.03.020
5. Mathieu S, Barrault S, Brunault P, Varescon I. Gambling motives: do they explain cognitive distortions in male poker gamblers? J Gambl Stud (2017):1–13. doi:10.1007/s10899-017-9700-8
6. American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders, Fourth Edition, Text Revision (DSM-IV-TR). Washington, DC: American Psychiatric Association (2000).
7. Petry NM, Blanco C, Stinchfield R, Volberg R. An empirical evaluation of proposed changes for gambling diagnosis in the DSM-5. Addiction (2013) 108:575–81. doi:10.1111/j.1360-0443.2012.04087.x
8. Granero R, Penelo E, Stinchfield R, Fernández-Aranda F, Aymamí N, Gómez-Peña M, et al. Contribution of illegal acts to pathological gambling diagnosis: DSM-5 implications. J Addict Dis (2014) 33:41–52. doi:10.1080/10550887.2014.882730
9. Stinchfield R, Govoni R, Frisch GR. DSM-IV diagnostic criteria for pathological gambling: reliability, validity, and classification accuracy. Am J Addict (2005) 14:73–82. doi:10.1080/10550490590899871
10. Stinchfield R, McCready J, Turner NE, Jimenez-Murcia S, Petry NM, Grant J, et al. Reliability, validity, and classification accuracy of the DSM-5 diagnostic criteria for gambling disorder and comparison to DSM-IV. J Gambl Stud (2016) 32:905–22. doi:10.1007/s10899-015-9573-7
11. Temcheff CE, Paskus TS, Potenza MN, Derevensky JL. Which diagnostic criteria are most useful in discriminating between social gamblers and individuals with gambling problems? An examination of DSM-IV and DSM-5 criteria. J Gambl Stud (2016) 32:957–68. doi:10.1007/s10899-015-9591-5
12. Gorsane MA, Reynaud M, Vénisse J-L, Legauffre C, Valleur M, Magalon D, et al. Gambling disorder-related illegal acts: regression model of associated factors. J Behav Addict (2017) 6:64–73. doi:10.1556/2006.6.2017.003
13. Abbott MW, McKenna BG. Gambling and problem gambling among recently sentenced women in New Zealand prisons. J Gambl Stud (2005) 21:559–81. doi:10.1007/s10899-005-5563-5
14. Del Pino-Gutiérrez A, Fernández-Aranda F, Granero R, Tárrega S, Valdepérez A, Agüera Z, et al. Impact of alcohol consumption on clinical aspects of gambling disorder. Int J Ment Health Nurs (2017) 26:121–8. doi:10.1111/inm.12221
15. Kuoppamäki SM, Kääriäinen J, Lind K. Examining gambling-related crime reports in the National Finnish Police Register. J Gambl Stud (2014) 30:967–83. doi:10.1007/s10899-013-9393-6
16. Turner NE, Preston DL, Saunders C, McAvoy S, Jain U. The relationship of problem gambling to criminal behavior in a sample of Canadian male federal offenders. J Gambl Stud (2009) 25:153–69. doi:10.1007/s10899-009-9124-1
17. Echeburua Odriozola E, Amor Andrés PJ, Yuste García J. Atenuación de la responsabilidad penal en la ludopatía: Bases Psicopatológicas. Psicopatología clínica, legal y forense (2000) 1:59–77.
18. Agnew R. Foundation for a general strain theory of crime and delinquency. Criminology (1992) 30:47–87. doi:10.1111/j.1745-9125.1992.tb01093.x
19. Agnew R. Building on the foundation of general strain theory: specifying the types of strain most likely to lead to crime and delinquency. J Res Crime Delinq (2001) 38:319–61. doi:10.1177/0022427801038004001
21. Ledgerwood DM, Weinstock J, Morasco BJ, Petry NM. Clinical features and treatment prognosis of pathological gamblers with and without recent gambling-related illegal behavior. J Am Acad Psychiatry Law (2007) 35:294–301.
22. Konkolÿ Thege B, Hodgins DC, Wild TC. Co-occurring substance-related and behavioral addiction problems: a person-centered, lay epidemiology approach. J Behav Addict (2016) 5:614–22. doi:10.1556/2006.5.2016.079
23. Toce-Gerstein M, Gerstein DR, Volberg RA. A hierarchy of gambling disorders in the community. Addiction (2003) 98:1661–72. doi:10.1111/j.1360-0443.2003.00545.x
24. Carragher N, McWilliams LA. A latent class analysis of DSM-IV criteria for pathological gambling: results from the National Epidemiologic Survey on Alcohol and Related Conditions. Psychiatry Res (2011) 187:185–92. doi:10.1016/j.psychres.2010.12.022
25. Strong DR, Kahler CW. Evaluation of the continuum of gambling problems using the DSM-IV. Addiction (2007) 102:713–21. doi:10.1111/j.1360-0443.2007.01789.x
26. Mariano M, Pino MC, Peretti S, Valenti M, Mazza M. Understanding criminal behavior: empathic impairment in criminal offenders. Soc Neurosci (2016) 12:379–85. doi:10.1080/17470919.2016.1179670
27. Potenza MN, Steinberg MA, McLaughlin SD, Rounsaville BJ, O’Malley SS. Illegal behaviors in problem gambling: analysis of data from a gambling helpline. J Am Acad Psychiatry Law (2000) 28:389–403.
28. Granero R, Fernández-Aranda F, Aymamí N, Gómez-Peña M, Fagundo AB, Sauchelli S, et al. Subtypes of pathological gambling with concurrent illegal behaviors. J Gambl Stud (2015) 31:1161–78. doi:10.1007/s10899-014-9499-5
29. Blaszczynski A, McConaghy N, Frankova A. Crime, antisocial personality and pathological gambling. J Gambl Behav (1989) 5:137–52. doi:10.1007/BF01019760
30. Laursen B, Plauborg R, Ekholm O, Larsen CVL, Juel K. Problem gambling associated with violent and criminal behaviour: a Danish Population-Based Survey and Register Study. J Gambl Stud (2016) 32:25–34. doi:10.1007/s10899-015-9536-z
32. Gottfredson MR, Hirschi T. A General Theory of Crime. Stanford University Press (1990). Available from: http://psycnet.apa.org/psycinfo/1990-97753-000
33. Barnes GM, Welte JW, Hoffman JH, Dintcheff BA. Shared predictors of youthful gambling, substance use, and delinquency. Psychol Addict Behav (2005) 19:165–74. doi:10.1037/0893-164X.19.2.165
35. Steward T, Mestre-Bach G, Fernández-Aranda F, Granero R, Perales JC, Navas JF, et al. Delay discounting and impulsivity traits in young and older gambling disorder patients. Addict Behav (2017) 71:96–103. doi:10.1016/j.addbeh.2017.03.001
36. Mestre-Bach G, Granero R, Steward T, Fernández-Aranda F, Baño M, Aymamí N, et al. Reward and punishment sensitivity in women with gambling disorder or compulsive buying: implications in treatment outcome. J Behav Addict (2016) 5:658–65. doi:10.1556/2006.5.2016.074
37. Jiménez-Murcia S, Fernández-Aranda F, Mestre-Bach G, Granero R, Tárrega S, Torrubia R, et al. Exploring the relationship between reward and punishment sensitivity and gambling disorder in a clinical sample: a path modeling analysis. J Gambl Stud (2016) 33(2):579–97. doi:10.1007/s10899-016-9631-9
38. Mishra S, Lalumière ML, Morgan M, Williams RJ. An examination of the relationship between gambling and antisocial behavior. J Gambl Stud (2011) 27:409–26. doi:10.1007/s10899-010-9217-x
39. Mishra S, Lalumière ML, Williams RJ. Gambling, risk-taking, and antisocial behavior: a replication study supporting the generality of deviance. J Gambl Stud (2017) 33:15–36. doi:10.1007/s10899-016-9608-8
40. Dowling NA, Merkouris SS, Greenwood CJ, Oldenhof E, Toumbourou JW, Youssef GJ. Early risk and protective factors for problem gambling: a systematic review and meta-analysis of longitudinal studies. Clin Psychol Rev (2017) 51:109–24. doi:10.1016/j.cpr.2016.10.008
41. Loeber R, Menting B, Lynam DR, Moffitt TE, Stouthamer-Loeber M, Stallings R, et al. Findings from the Pittsburgh youth study: cognitive impulsivity and intelligence as predictors of the age-crime curve. J Am Acad Child Adolesc Psychiatry (2012) 51:1136–49. doi:10.1016/j.jaac.2012.08.019
42. Berg JM, Latzman RD, Bliwise NG, Lilienfeld SO. Parsing the heterogeneity of impulsivity: a meta-analytic review of the behavioral implications of the UPPS for psychopathology. Psychol Assess (2015) 27:1129–46. doi:10.1037/pas0000111
43. Canale N, Vieno A, Bowden-Jones H, Billieux J. The benefits of using the UPPS model of impulsivity rather than the Big Five when assessing the relationship between personality and problem gambling. Addiction (2017) 112:372–3. doi:10.1111/add.13641
44. Johansson A, Grant JE, Kim SW, Odlaug BL, Götestam KG. Risk factors for problematic gambling: a critical literature review. J Gambl Stud (2009) 25:67–92. doi:10.1007/s10899-008-9088-6
45. Tomko RL, Prisciandaro JJ, Falls SK, Magid V. The structure of the UPPS-R-Child impulsivity scale and its relations with substance use outcomes among treatment-seeking adolescents. Drug Alcohol Depend (2016) 161:276–83. doi:10.1016/j.drugalcdep.2016.02.010
46. Michalczuk R, Bowden-Jones H, Verdejo-Garcia A, Clark L. Impulsivity and cognitive distortions in pathological gamblers attending the UK National Problem Gambling Clinic: a preliminary report. Psychol Med (2011) 41:2625–35. doi:10.1017/S003329171100095X
47. Del Prete F, Steward T, Navas JF, Fernández-Aranda F, Jiménez-Murcia S, Oei TPS, et al. The role of affect-driven impulsivity in gambling cognitions: a convenience-sample study with a Spanish version of the Gambling-Related Cognitions Scale. J Behav Addict (2017) 6:51–63. doi:10.1556/2006.6.2017.001
48. Esbec E, y Delgado S. Aspectos periciales de la prodigalidad. Juego y ludopatía. In: Albarrán J, co-ordinator, Peritaje psicológico en procedimientos civiles y laborales. Madrid: Fundación Universidad Empresa (1998).
49. May-Chahal C, Humphreys L, Clifton A, Francis B, Reith G. Gambling harm and crime careers. J Gambl Stud (2017) 33:65–84. doi:10.1007/s10899-016-9612-z
50. Lesieur HR, Blume SB. The South Oaks Gambling Screen (SOGS): a new instrument for the identification of pathological gamblers. Am J Psychiatry (1987) 144:1184–8. doi:10.1176/ajp.144.9.1184
51. Echeburúa E, Báez C, Fernández J, Páez D. Cuestionario de juego patológico de South Oaks (SOGS): Validación española. [South Oaks Gambling Screen (SOGS): Spanish validation]. Anális Modif Cond (1994) 20:769–91.
52. Whiteside SP, Lynam DR, Miller JD, Reynolds SK. Validation of the UPPS Impulsive Behavior Scale: a four factor model of impulsivity. Eur J Pers (2005) 19(7):559–74. doi:10.1002/per.556
53. Verdejo-García A, Lozano Ó, Moya M, Alcázar MÁ, Pérez-García M. Psychometric properties of a Spanish version of the UPPS-P impulsive behavior scale: reliability, validity and association with trait and cognitive impulsivity. J Pers Assess (2010) 92:70–7. doi:10.1080/00223890903382369
54. Derogatis L. SCL-90-R. Administration, Scoring and Procedures Manual. Baltimore, MD: Clinical P (1990).
56. Cloninger CR. The Temperament and Character Inventory-Revised. St. Louis, MO: Center for St. Louis, MO (1999).
57. Gutiérrez-Zotes J, Bayón C, Montserrat C, Valero J, Labad A, Cloninger C, et al. Temperament and Character Inventory Revised (TCI-R). Standardization and normative data in a general population sample. Actas Españolas Psiquiatr (2004) 32:8–15.
58. Saunders JB, Aasland OG, Babor TF, de la Fuente JR, Grant M. Development of the Alcohol Use Disorders Identification Test (AUDIT): WHO Collaborative Project on early detection of persons with harmful alcohol consumption – II. Addiction (1993) 88:791–804. doi:10.1111/j.1360-0443.1993.tb02093.x
59. Martínez J. Validación de los cuestionarios breves: AUDIT, CAGE y CBA, para la detección de los problemas relacionados con el consumo de bebidas alcohólicas en atención primaria. Sevilla: Consejería (1999).
60. Reinert DF, Allen JP. The Alcohol Use Disorders Identification Test (AUDIT): a review of recent research. Alcohol Clin Exp Res (2002) 26:272–9. doi:10.1111/j.1530-0277.2002.tb02534.x
61. Berman AH, Bergman H, Palmstierna T, Schlyter F. Evaluation of the drug use Disorders Identification Test (DUDIT) in criminal justice and detoxification settings and in a Swedish population sample. Eur Addict Res (2005) 11:22–31. doi:10.1159/000081413
62. Jiménez-Murcia S, Aymamí-Sanromà M, Gómez-Peña M, Álvarez-Moya E, Vallejo J. Protocols de tractament cognitivoconductual pel joc patològic i d’altres addiccions no tòxiques. Barcelona, Spain: Hospital Universitari de Bellvitge, Departament de Salut, Generalitat de Catalunya (2006).
63. Finner H. On a monotonicity problem in step-down multiple test procedures. J Am Stat Assoc (1993) 88:920–3. doi:10.1080/01621459.1993.10476358
64. Ehrlich I. Participation in illegitimate activities: a theoretical and empirical investigation. J Polit Econ (1973) 81:521–65. doi:10.2307/1831025
65. Swisher RR, Dennison CR. Educational pathways and change in crime between adolescence and early adulthood. J Res Crime Delinq (2016) 53:840–71. doi:10.1177/0022427816645380
66. Farrington D. Age and crime. Crime Justice (1986). Available from: http://www.journals.uchicago.edu/doi/abs/10.1086/449114
67. Piquero A, Farrington D, Blumstein A. Key Issues in Criminal Career Research: New Analyses of the Cambridge Study in Delinquent Development. New York: Cambridge University Press (2007).
68. Hernández de Frutos T. Social stratification and delinquency. Forty years of sociological discrepancy. Rev Int Sociol (2006) LXIV:199–232. doi:10.3989/ris.2006.i45.21
69. Glass JE, Grant JD, Yoon HY, Bucholz KK. Alcohol problem recognition and help seeking in adolescents and young adults at varying genetic and environmental risk. Drug Alcohol Depend (2015) 153:250–7. doi:10.1016/j.drugalcdep.2015.05.006
70. Black DW, Shaw M, Coryell W, Crowe R, McCormick B, Allen J. Age at onset of DSM-IV pathological gambling in a non-treatment sample: early- versus later-onset. Compr Psychiatry (2015) 60:40–6. doi:10.1016/j.comppsych.2015.04.007
71. Castrén S, Basnet S, Salonen AH, Pankakoski M, Ronkainen J-E, Alho H, et al. Factors associated with disordered gambling in Finland. Subst Abuse Treat Prev Policy (2013) 8:24. doi:10.1186/1747-597X-8-24
72. Lopez-Vergara HI, Spillane NS, Merrill JE, Jackson KM. Developmental trends in alcohol use initiation and escalation from early to middle adolescence: prediction by urgency and trait affect. Psychol Addict Behav (2016) 30:1–10. doi:10.1037/adb0000173
73. Fassino S, Amianto F, Sobrero C, Abbate Daga G. Does it exist a personality core of mental illness? A systematic review on core psychobiological personality traits in mental disorders. Panminerva Med (2013) 55:397–413.
74. Granero R, Fernández-Aranda F, Steward T, Mestre-Bach G, Baño M, Del Pino-Gutiérrez A, et al. Compulsive buying behavior: characteristics of comorbidity with gambling disorder. Front Psychol (2016) 7:625. doi:10.3389/fpsyg.2016.00625
75. Granero R, Fernández-Aranda F, Mestre-Bach G, Steward T, Baño M, del Pino-Gutiérrez A, et al. Compulsive buying behavior: clinical comparison with other behavioral addictions. Front Psychol (2016) 7:914. doi:10.3389/fpsyg.2016.00914
76. Scurich N, Monahan J. Evidence-based sentencing: public openness and opposition to using gender, age, and race as risk factors for recidivism. Law Hum Behav (2015) 40:36–41. doi:10.1037/lhb0000161
77. Matejkowski J, Conrad A, Ostermann M. Does early onset of criminal behavior differentiate for whom serious mental illness has a direct or indirect effect on recidivism? Law Hum Behav (2017) 41:68–79. doi:10.1037/lhb0000231
Keywords: gambling disorder, impulsivity, criminal behavior, psychopathology, risk factors
Citation: Mestre-Bach G, Steward T, Granero R, Fernández-Aranda F, Talón-Navarro MT, Cuquerella À, Baño M, Moragas L, del Pino-Gutiérrez A, Aymamí N, Gómez-Peña M, Mallorquí-Bagué N, Vintró-Alcaraz C, Magaña P, Menchón JM and Jiménez-Murcia S (2018) Gambling and Impulsivity Traits: A Recipe for Criminal Behavior?. Front. Psychiatry 9:6. doi: 10.3389/fpsyt.2018.00006
Received: 15 November 2017; Accepted: 11 January 2018;
Published: 29 January 2018
Edited by:
Roumen Kirov, Institute of Neurobiology (BAS), BulgariaReviewed by:
Andreas Becker, University Medical Center Göttingen, GermanyMohamed Ali Gorsane, Centre hospitalier Sainte-Anne, France
Francine Ferland, Centre Intégré Universitaire de Santé et de Services Sociaux de la Capitale-Nationale (CIUSSSCN), Canada
Copyright: © 2018 Mestre-Bach, Steward, Granero, Fernández-Aranda, Talón-Navarro, Cuquerella, Baño, Moragas, del Pino-Gutiérrez, Aymamí, Gómez-Peña, Mallorquí-Bagué, Vintró-Alcaraz, Magaña, Menchón and Jiménez-Murcia. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Susana Jiménez-Murcia, c2ppbWVuZXpAYmVsbHZpdGdlaG9zcGl0YWwuY2F0