
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
MINI REVIEW article
Front. Nutr. , 06 November 2017
Sec. Food Chemistry
Volume 4 - 2017 | https://doi.org/10.3389/fnut.2017.00053
 Ines Banjari1Andreja Misir1Katarina Šavikin2Stela Jokić1Maja Molnar1
Ines Banjari1Andreja Misir1Katarina Šavikin2Stela Jokić1Maja Molnar1 H. K. S. De Zoysa3
H. K. S. De Zoysa3 Viduranga Y. Waisundara3*
Viduranga Y. Waisundara3*
Diabetes is a global pandemic which warrants urgent attention due to its rising prevalence and economic burden. Thus, many alternative therapies are being researched for antidiabetic properties, given the inefficacy of current medicinal treatments. From this perspective, Aronia melanocarpa or black chokeberry has been investigated for its therapeutic properties in many studies, especially for its ability to combat hyperglycemia-induced oxidative stress and the macrovascular complications of diabetes including cardiovascular disease. Though A. melanocarpa is native to the eastern areas of North America, it has been planted extensively in Europe and Asia as well. Several in vivo studies have displayed the antioxidant properties of A. melanocarpa berry juice and plant extract in rat models where oxidative stress markers were observed to have significant reductions. Some of the potent bioactive compounds present in the fruits and other parts of the plant were identified as (−)-epicatechin, chlorogenic acid, neochlorogenic acid, and cyanidin-3-galactoside. Overall, A. melanocarpa could be considered a good source of antioxidants which is effective in combating hyperglycemia-induced oxidative stress.
Diabetes mellitus is a metabolic disorder of the endocrine system and is currently considered a global pandemic. The disease is prevalent in all parts of the world and is especially on the rise in developing and newly developed nations. Individuals with diabetes are not able of producing or properly utilizing insulin in the body, thus resulting in elevated glucose levels. The cause of diabetes is multi-faceted, although both genetic and environmental factors such as obesity and lack of exercise appear to play critical roles (1–3). Ethnic and racial differences have also been found to contribute to the prevalence of diabetes, especially among heterogeneous populations within the same area (1). Additionally, scientific evidence leads to the belief that in the presence of a particular genetic predisposition, environmental factors trigger the development of diabetes. On the other hand, in type 2 diabetes mellitus, a chronic exposure of βTC3 cells to high glucose levels has been known to result in glucose toxicity via increased oxidative stress (4). The injury caused by hyperglycemia-induced oxidative stress can affect all organs. A growing amount of evidence indicates that the consumption of plant foods is correlated with a lower risk from development of oxidative stress-related diseases, especially diabetes (5). Although there are a number of antidiabetic medications, no single marketed drug has succeeded in lowering hyperglycemia-induced oxidative stress. Most therapies target at lowering HbA1c. However, these drugs—when used in combination with other pharmaceutical agents—tend to lose much of their efficacy after continuous usage (6). Weight gain is the primary side-effect of many of the antidiabetic therapies such as sulfonylureas, α-glucosidase inhibitors, and thiazolidinediones. Because many diabetic patients are already obese, this side-effect is particularly undesirable. When it comes to a point where oral therapies can no longer adequately control blood sugar, the only remaining option is injectable insulin therapy. Nevertheless, none of these interventions adequately address oxidative stress, and therefore, the complications arising from the disease condition worsen. As a result, there is an existing need for novel therapies, and more importantly, dietary interventions and changes in the lifestyle to provide both enhanced benefits for diabetic patients. The purpose of this mini review is to serve as an updated summary of the antidiabetic effects of A. melanocarpa and its applications in other disease conditions. Several recent studies focused on A. melanocarpa potential in this context. Figure S1 in Supplementary Material summarizes all the disease conditions for which A. melanocarpa has been used to date (including its traditional medicinal applications) and has been proven effective.
From the perspective of oxidative stress, plant-based products which are rich in anthocyanins have been shown to exhibit a plethora of pharmacological properties, such as anti-inflammatory, antitumor, and antioxidant activities. These properties have scientifically displayed beneficial effects for mitigating hyperglycemia-induced oxidative stress and its resulting complications (7–9). A. melanocarpa (Michx.) Elliott or black chokeberry is a fruit/plant which has been extensively investigated for its antidiabetic properties. Images of this plant are shown in Figure S2A–C in Supplementary Material and its major bioactive compounds in Figure S2D in Supplementary Material. Due to the astringent taste of these fruits and their smell of bitter-almonds, pure A. melanocarpa products are not particularly popular among many consumers, although they have been documented as a “functional food” in Russia since the 1940s (10).
Aronia melanocarpa preparations are sometimes consumed as a complementary and alternative therapy for conditions such as achlorhydria, avitaminoses, convalescence, and hemorrhoids (11). High anthocyanin contents in A. melanocarpa have led to investigating the bioactives present in its extracts (12, 13). A. melanocarpa juice (200 mL) was shown to have a potent effect on postprandial glucose in healthy subjects after an oral meal tolerance test (14). This effect was imparted regardless of the gender of the subjects and was additionally shown to reduce the activity of dipeptidyl peptidase IV, α-glucosidase, and angiotensin-converting enzyme (ACE) in a dose-dependent manner (14). Table 1 summarizes studies which have successfully demonstrated the hypoglycemic, hypolipidemic, and antioxidant effects of various parts and extracts of the plant. Table 2 summarizes the studies dedicated to identifying the components and bioactive compounds of interest along with their findings. Furthermore, reviews such as those by Jurikova and others (15), Chrubasik et al. (10), Kokotkiewicz et al. (11), and Parzonko and Naruszewicz (16) have appeared recently highlighting the antidiabetic effects of A. melanocarpa in relation to mitigating hyperglycemia-induced oxidative stress and other precipitating conditions of the disease.
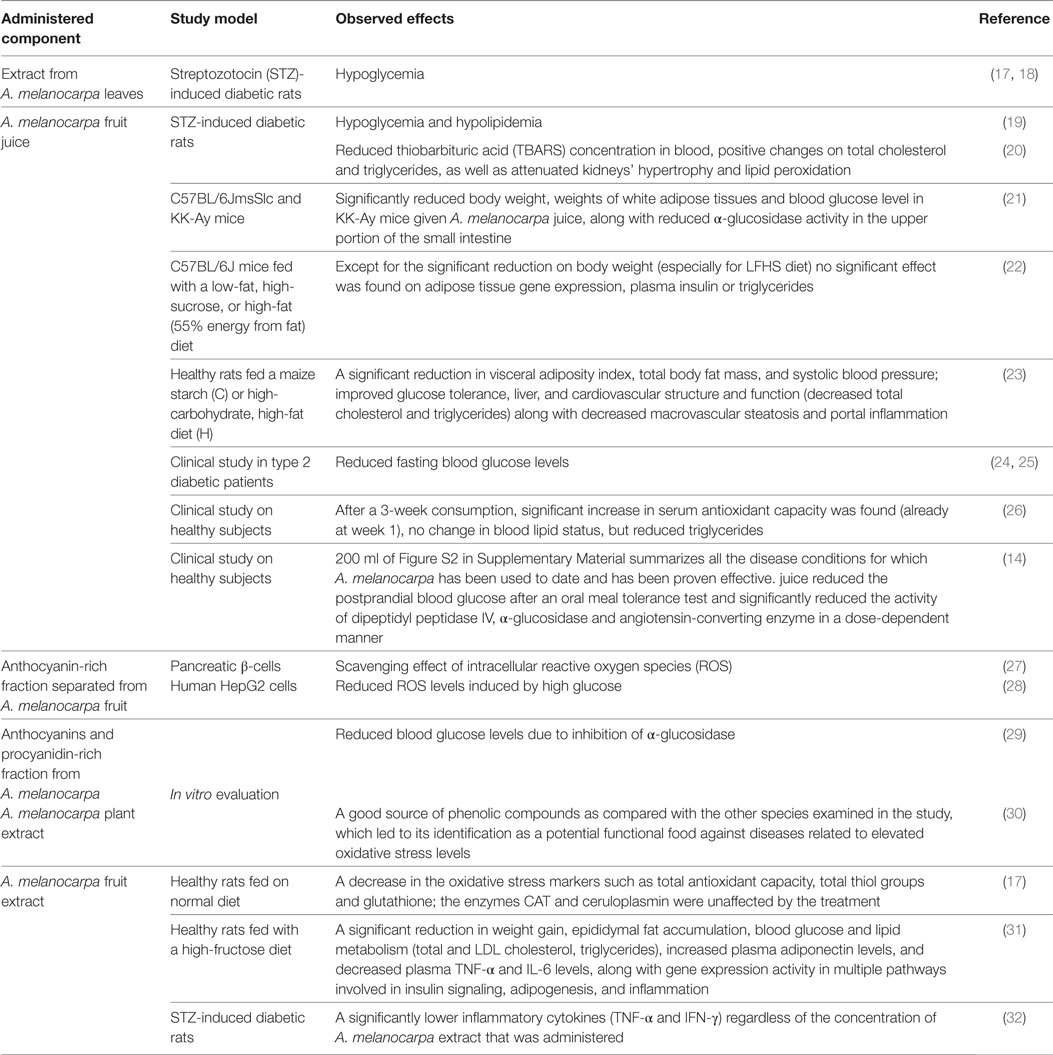
Table 1. Studies demonstrating the therapeutic properties of Aronia melanocarpa.
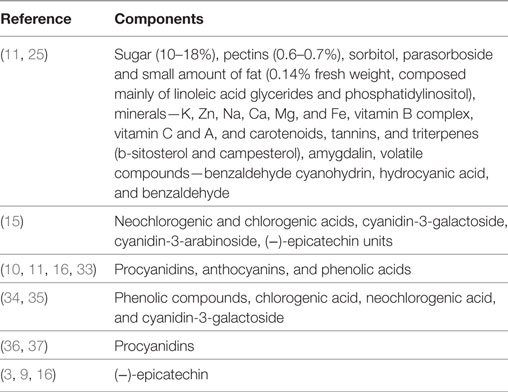
Table 2. Compositional details and bioactive compounds in Aronia melanocarpa fruits.
Although the number of published studies on A. melanocarpa increases by day, only a few have been conducted to evaluate its therapeutic effects clinically. According to Chrubasik et al. (10), only 13 clinical trials which encompassed various A. melanocarpa products for treatment of metabolic syndrome, hypercholesterolemia, and type 2 diabetes have been published to date, while 2 studies had been conducted on healthy participants, and another 3 on other health issues. Nevertheless, all studies showed significant improvements in the observed parameters at a clinical level. The initial use of A. melanocarpa by Native Americans was for the treatment of colds, but its popularity increased after it was introduced to Russia and Eastern Europe where it was extensively used as an anti-hypertensive drug (11). The anti-hypertensive potential of A. melanocarpa was proven by Kardum et al. (38). They conducted a 4-week intervention study with 200 mL of A. melanocarpa berry juice administered per day to subjects with pharmacologically untreated high normal blood pressure (BP) and grade I hypertension. In this study, the average 24-h and awake systolic (SBP) and diastolic BP (DBP) had significantly decreased, while these were higher in the group with a prevalence of sympathetic activity. Interestingly, reduction in SBP and DBP was more significant when a period of regular consumption of A. melanocarpa berry juice was followed (39). Another study by Broncel et al. (40) also demonstrated significant reductions in both SBP and DBP after 2 months of consumption of 300 mg of A. melanocarpa berry extract per day among patients with metabolic syndrome. Overall, these studies showed the potential of long-term consumption of A. melanocarpa berry juice, although periods of continuous usage were recommended to be accompanied with a period of abstain.
The therapeutic potential of A. melanocarpa was proven to be higher among people with increased cardiovascular risk (41), inferring that they should be one of the target populations to whom this plant extract should be administered. One of the underlying therapeutic mechanisms of action of A. melanocarpa is the stimulation of the endothelial formation of nitric oxide (NO) in coronary arteries (via phosphorilation of eNOS) (42). Yamane and others (43) showed that in spontaneously hypertensive rats, a diet containing freeze-dried A. melanocarpa berries significantly reduces SBP along with a significantly reduced ACE activity at 4 weeks. Inhibition of ACE activity has been attributed to anthocyanidins and flavonoids which are all highly abundant in A. melanocarpa (36, 37, 44, 45). More recently, the study by Bhaswant et al. (23) found similar beneficial effects on parameters related to the metabolic syndrome in rats fed with either A. melanocarpa juice or purple maize flour. The main conclusion of this study was that anthocyanins are the most probable bioactive components responsible for the observed beneficial effects in A. melanocarpa.
Another therapeutic potential of A. melanocarpa is its modulation of the lipoprotein profile (10, 11). This was particularly demonstrated in the study by Kardum and others (46) where significant reductions in the triglyceride content (TG) was observed among mildly hypertensive patients after 4 weeks of consumption of A. melanocarpa berry juice. Significant reduction in TG was also demonstrated in the study by Nowak and others (26), which was conducted in healthy individuals. In this study, men with mild hypercholesterolemia consumed 250 mL of the fruit juice for 3 weeks and achieved significant metabolic changes (40). It is important to note that regular consumption of A. melanocarpa is recommended even for people already on statin therapy (47).
The anti-inflammatory potential of A. melanocarpa juice was demonstrated in few studies through reduced levels of cytokines (38, 40), as well as in studies which used patients with cardiovascular disease (47). Badescu and others (32) demonstrated that the chronic inflammatory reaction related to diabetes mellitus improves under the action of polyphenols from A. melanocarpa, specifically through its ability to lower TNF-α and IFN-γ.
At present, approximately 415 million people around the world have been contracted with diabetes, while a constant increase in the number is expected. Furthermore, pre-diabetes (defined as impaired fasting glucose or impaired glucose tolerance) has observed to significantly increase the risk for developing diabetes and its complications, where the current prevalence is estimated to be 6.7% (48). The quality of life is affected by this disease while the life expectancy among diabetics is reduced by 5–10 years as compared with the healthy population, with cardiovascular complications representing the major cause of mortality. The financial burden occurring from this disease is evident to be substantial. Globally, 12% of the total health-care resources are being spent for diabetes treatment, ranging from 5 to 20% (48). However, along with reduced financial allocations toward health care, especially in terms of preventive measures and pharmaceuticals, the burden falls onto patients and their families. People with diabetes spend 2.5 times for health care from their own financial reserves than their healthy counterparts (49), especially if they have developed cardiovascular disease (50). Finding a way to bridge the gap between current treatments, preventive measures (directed toward pre-diabetes as well as delay of diabetes complications), possible adjuvant therapies, and dietary and lifestyle modification is strongly encouraged given this situation (48). As highlighted in this review, A. melanocarpa berry juice and plant extract has displayed evidence as a potent modulator of hyperglycemia-related oxidative stress which is directly correlated with its complications, in particular, cardiovascular disease. Nevertheless, continuous use of A. melanocarpa is recommended to be accompanied with the same period of abstain. Also, people with increased cardiovascular risk (i.e., with abdominal obesity, mild hypercholesterolemia, grade I hypertension) seem to benefit more from the consumption of A. melanocarpa berry juice and extract. Thus, overall, consumption of A. melanocarpa could be recommended as a possible approach to reducing the financial burden for both diabetics and their families, as well as that of national health-care systems in countries where diabetes poses a significant liability. Additionally, the fruit and its extract appear to have a multitude of beneficial effects against other disease conditions, which could potentially be explored and scientifically substantiated through systematic studies and investigations.
IB, AM, KŠ, SJ, MM, HZ, and VW equally contributed to the acquisition of information, drafting the manuscript, and approving the final version.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
The Supplementary Material for this article can be found online at http://www.frontiersin.org/article/10.3389/fnut.2017.00053/full#supplementary-material.
Figure S1. Disease conditions for which administration/consumption of A. melanocarpa has proven to be effective.
Figure S2. Images of (A) A. melanocarpa in fields during summer-time (B), bushes with fruits, (C) fruits & leaves and (D) the chemical structures of some of the potent bioactive compounds present in A. melanocarpa.
1. Li W, Zheng H, Bukuru J, De Kimpe N. Natural medicines used in the traditional Chinese medical system for therapy of diabetes mellitus. J Ethnopharmacol (2004) 92(1):1–21. doi:10.1016/j.jep.2003.12.031
2. Torgerson JS, Hauptman J, Boldrin MN, Sjöström L. Xenical in the prevention of diabetes in obese subjects (XENDOS) study. Diabetes Care (2004) 27(1):155–61. doi:10.2337/diacare.27.1.155
3. Tuomilehto J. Finnish Diabetes Prevention Study Group: prevention of type 2 diabetes mellitus by changes in lifestyle among subjects with impaired glucose tolerance. N Engl J Med (2001) 344:1343–50. doi:10.1056/NEJM200105033441801
4. Robertson RP. Chronic oxidative stress as a central mechanism for glucose toxicity in pancreatic islet beta cells in diabetes. J Biol Chem (2004) 279(41):42351–4. doi:10.1074/jbc.R400019200
5. Coman C, Rugina OD, Socaciu C. Plants and natural compounds with antidiabetic action. Not Bot Horti Agrobot Cluj Napoca (2012) 40(1):314–25. doi:10.15835/nbha4017205
7. Liu J, Zhang W, Jing H, Popovich DG. Bog Bilberry (Vaccinium uliginosum L.) Extract reduces cultured Hep-G2, Caco-2, and 3T3-L1 cell viability, affects cell cycle progression, and has variable effects on membrane permeability. J Food Sci (2010) 75(3):H103–7. doi:10.1111/j.1750-3841.2010.01546.x
8. Zafra-Stone S, Yasmin T, Bagchi M, Chatterjee A, Vinson JA, Bagchi D. Berry anthocyanins as novel antioxidants in human health and disease prevention. Mol Nutr Food Res (2007) 51(6):675–83. doi:10.1002/mnfr.200700002
9. Zhang B, Kang M, Xie Q, Xu B, Sun C, Chen K, et al. Anthocyanins from Chinese bayberry extract protect β cells from oxidative stress-mediated injury via HO-1 upregulation. J Agric Food Chem (2011) 59(2):537–45. doi:10.1021/jf1035405
10. Chrubasik C, Li G, Chrubasik S. The clinical effectiveness of chokeberry: a systematic review. Phytother Res (2010) 24(8):1107–14. doi:10.1002/ptr.3226
11. Kokotkiewicz A, Jaremicz Z, Luczkiewicz M. Aronia plants: a review of traditional use, biological activities, and perspectives for modern medicine. J Med Food (2010) 13(2):255–69. doi:10.1089/jmf.2009.0062
12. Zdunczyk Z, Frejnagel S, Wróblewska M, Juśkiewicz J, Oszmiański J, Estrella I. Biological activity of polyphenol extracts from different plant sources. Food Res Intern (2002) 35(2):183–6. doi:10.1016/S0963-9969(01)00181-8
13. Kähkönen MP, Hopia AI, Vuorela HJ, Rauha J-P, Pihlaja K, Kujala TS, et al. Antioxidant activity of plant extracts containing phenolic compounds. J Agric Food Chem (1999) 47(10):3954–62. doi:10.1021/jf990146l
14. Yamane T, Kozuka M, Wada-Yoneta M, Sakamoto T, Nakagaki T, Nakano Y, et al. Aronia juice suppresses the elevation of postprandial blood glucose levels in adult healthy Japanese. Clin Nutr Exp (2017) 12:20–6. doi:10.1016/j.yclnex.2017.01.002
15. Jurikova T, Mlcek J, Skrovankova S, Sumczynski D, Sochor J, Hlavacova I, et al. Fruits of black chokeberry Aronia melanocarpa in the prevention of chronic diseases. Molecules (2017) 22(6):944. doi:10.3390/molecules22060944
16. Parzonko A, Naruszewicz M. Cardioprotective effects of Aronia melanocarpa anthocynanins. From laboratory experiments to clinical practice. Curr Pharm Des (2016) 22(2):174–9. doi:10.2174/1381612822666151112152143
17. Oprea E, Manolescu BN, Fărcăşanu IC, Mladin P, Mihele D. Studies concerning antioxidant and hypoglycaemic activity of Aronia melanocarpa fruits. Revista Farmacia (2014) 62(2):254–63.
18. Maslov D, Ipatova O, Abakumova O, Tsvetkova T, Prozorovskiĭ V. Hypoglycemic effect of an extract from Aronia melanocarpa leaves. Voprosy meditsȋnskoiĭ khimii (2002) 48(3):271–7.
19. Valcheva-Kuzmanova S, Kuzmanov K, Tancheva S, Belcheva A. Hypoglycemic and hypolipidemic effects of Aronia melanocarpa fruit juice in streptozotocin-induced diabetic rats. Methods Find Exp Clin Pharmacol (2007) 29(2):1–5. doi:10.1358/mf.2007.29.2.1075349
20. Jurgonski A, Juskiewicz J, Zdunczyk Z. Comparison of the effects of chokeberry fruit extract, chicory flour and their dietary combination on blood parameters and antioxidant status of healthy and diabetic rats. Pol J Food Nutr Sci (2008) 58(2):273–8.
21. Yamane T, Kozuka M, Konda D, Nakano Y, Nakagaki T, Ohkubo I, et al. Improvement of blood glucose levels and obesity in mice given Aronia juice by inhibition of dipeptidyl peptidase IV and α-glucosidase. J Nutr Biochem (2016) 31:106–12. doi:10.1016/j.jnutbio.2016.02.004
22. Baum JI, Howard LR, Prior RL, Lee S-O. Effect of Aronia melanocarpa (black chokeberry) supplementation on the development of obesity in mice fed a high-fat diet. J Berry Res (2016) 6(2):203–12. doi:10.3233/JBR-160134
23. Bhaswant M, Shafie SR, Mathai ML, Mouatt P, Brown L. Anthocyanins in chokeberry and purple maize attenuate diet-induced metabolic syndrome in rats. Nutrition (2017) 41:24–31. doi:10.1016/j.nut.2016.12.009
24. Simeonov S, Botushanov N, Karahanian E, Pavlova M, Husianitis H, Troev D. Effects of Aronia melanocarpa juice as part of the dietary regimen in patients with diabetes mellitus. Folia Med (2002) 44(3):20–3.
25. Kulling SE, Rawel HM. Chokeberry (Aronia melanocarpa) – a review on the characteristic components and potential health effects. Planta Med (2008) 74(13):1625–34. doi:10.1055/s-0028-1088306
26. Nowak D, Grabczewska Z, Gośliński M, Obońska K, Dabrowska A, Kubica J. Effect of chokeberry juice consumption on antioxidant capacity, lipids profile and endothelial function in healthy people: a pilot study. Czh J Food Sci (2016) 34(1):39–46. doi:10.17221/258/2015-CJFS
27. Rugină D, Diaconeasa Z, Coman C, Bunea A, Socaciu C, Pintea A. Chokeberry anthocyanin extract as pancreatic β-cell protectors in two models of induced oxidative stress. Oxid Med Cellular Longev (2015) 2015:1–10. doi:10.1155/2015/429075
28. Zhu W, Jia Q, Wang Y, Zhang Y, Xia M. The anthocyanin cyanidin-3-O-β-glucoside, a flavonoid, increases hepatic glutathione synthesis and protects hepatocytes against reactive oxygen species during hyperglycemia: Involvement of a cAMP–PKA-dependent signaling pathway. Free Radic Biol Med (2012) 52(2):314–27. doi:10.1016/j.freeradbiomed.2011.10.483
29. Bräunlich M, Slimestad R, Wangensteen H, Brede C, Malterud KE, Barsett H. Extracts, anthocyanins and procyanidins from Aronia melanocarpa as radical scavengers and enzyme inhibitors. Nutrients (2013) 5(3):663–78. doi:10.3390/nu5030663
30. Teleszko M, Wojdyło A. Comparison of phenolic compounds and antioxidant potential between selected edible fruits and their leaves. J Funct Foods (2015) 14:736–46. doi:10.1016/j.jff.2015.02.041
31. Qin B, Anderson RA. An extract of chokeberry attenuates weight gain and modulates insulin, adipogenic and inflammatory signalling pathways in epididymal adipose tissue of rats fed a fructose-rich diet. Br J Nutr (2012) 108(4):581–7. doi:10.1017/S000711451100599X
32. Badescu M, Badulescu O, Badescu L, Ciocoiu M. Effects of Sambucus nigra and Aronia melanocarpa extracts on immune system disorders within diabetes mellitus. Pharm Biol (2015) 53(4):533–9. doi:10.3109/13880209.2014.931441
34. Oszmiański J, Wojdylo A. Aronia melanocarpa phenolics and their antioxidant activity. Eur Food Res Technol (2005) 221(6):809–13. doi:10.1007/s00217-005-0002-5
35. Wu X, Gu L, Prior RL, McKay S. Characterization of anthocyanins and proanthocyanidins in some cultivars of Ribes, Aronia, and Sambucus and their antioxidant capacity. J Agric Food Chem (2004) 52(26):7846–56. doi:10.1021/jf0486850
36. Rop O, Mlček J, Juríková T, Valšíková M, Sochor J, Řezníček V, et al. Phenolic content, antioxidant capacity, radical oxygen species scavenging and lipid peroxidation inhibiting activities of extracts of five black chokeberry (Aronia melanocarpa (Michx.) Elliot) cultivars. J Med Plant Res (2010) 4:2431–7.
37. Do Thi N, Hwang E-S. Bioactive compound contents and antioxidant activity in Aronia (Aronia melanocarpa) leaves collected at different growth stages. Prev Nutr Food Sci (2014) 19(3):204–12. doi:10.3746/pnf.2014.19.3.204
38. Kardum N, Konić-Ristić A, Šavikin K, Spasić S, Stefanović A, Ivanišević J, et al. Effects of polyphenol-rich chokeberry juice on antioxidant/pro-oxidant status in healthy subjects. J Med Food (2014) 17(8):869–74. doi:10.1089/jmf.2013.0135
39. Skoczyñska A, Jêdrychowska I, Porêba R, Affelska-Jercha A, Turczyn B, Wojakowska A, et al. Influence of chokeberry juice on arterial blood pressure and lipid parameters in men with mild hypercholesterolemia. Pharm Rep (2007) 59(Suppl 1):177–82.
40. Broncel M, Kozirog M, Duchnowicz P, Koter-Michalak M, Sikora J, Chojnowska-Jezierska J. Aronia melanocarpa extract reduces blood pressure, serum endothelin, lipid, and oxidative stress marker levels in patients with metabolic syndrome. Med Sci Monit (2010) 16(1):CR28–34.
41. Kardum N, Takić M, Šavikin K, Zec M, Zdunić G, Spasić S, et al. Effects of polyphenol-rich chokeberry juice on cellular antioxidant enzymes and membrane lipid status in healthy women. J Funct Foods (2014) 9:89–97. doi:10.1016/j.jff.2014.04.019
42. Zheng J, Zhou Y, Li S, Zhang P, Zhou T, Xu D-P, et al. Effects and mechanisms of fruit and vegetable juices on cardiovascular diseases. Int J Mol Sci (2017) 18(3):555. doi:10.3390/ijms18030555
43. Yamane T, Kozuka M, Imai M, Yamamoto Y, Ohkubo I, Sakamoto T, et al. Reduction of blood pressure by aronia berries through inhibition of angiotensin-converting enzyme activity in the spontaneously hypertensive rat kidney. Funct Foods Health Dis (2017) 7(4):280–90.
44. Guerrero L, Castillo J, Quiñones M, Garcia-Vallvé S, Arola L, Pujadas G, et al. Inhibition of angiotensin-converting enzyme activity by flavonoids: structure-activity relationship studies. PLoS One (2012) 7(11):e49493. doi:10.1371/journal.pone.0049493
45. Persson IA-L, Persson K, Andersson RG. Effect of Vaccinium myrtillus and its polyphenols on angiotensin-converting enzyme activity in human endothelial cells. J Agric Food Chem (2009) 57(11):4626–9. doi:10.1021/jf900128s
46. Kardum N, Milovanović B, Šavikin K, Zdunić G, Mutavdžin S, Gligorijević T, et al. Beneficial effects of polyphenol-rich chokeberry juice consumption on blood pressure level and lipid status in hypertensive subjects. J Med Food (2015) 18(11):1231–8. doi:10.1089/jmf.2014.0171
47. Naruszewicz M, Łaniewska I, Millo B, Dłużniewski M. Combination therapy of statin with flavonoids rich extract from chokeberry fruits enhanced reduction in cardiovascular risk markers in patients after myocardial infraction (MI). Atherosclerosis (2007) 194(2):e179–84. doi:10.1016/j.atherosclerosis.2006.12.032
48. International Diabetes Federation. IDF Diabetes Atlas 6th. Brussels, Belgium: International Diabetes Federation (2015).
49. Health Care Cost Institute. Per Capita Health Care Spending on Diabetes: 2009–2013. Washington DC, USA: Health Care Cost Institute (2015).
Keywords: Aronia melanocarpa, cardiovascular disease, diabetes, oxidative stress, phenolic compounds
Citation: Banjari I, Misir A, Šavikin K, Jokić S, Molnar M, De Zoysa HKS and Waisundara VY (2017) Antidiabetic Effects of Aronia melanocarpa and Its Other Therapeutic Properties. Front. Nutr. 4:53. doi: 10.3389/fnut.2017.00053
Received: 18 September 2017; Accepted: 18 October 2017;
Published: 06 November 2017
Edited by:
Marcello Iriti, Università degli Studi di Milano, ItalyReviewed by:
Jesus Osada, University of Zaragoza, SpainCopyright: © 2017 Banjari, Misir, Šavikin, Jokić, Molnar, De Zoysa and Waisundara. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) or licensor are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Viduranga Y. Waisundara, dmlkdXJhbmdhQGdtYWlsLmNvbQ==
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.